
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Microwave ablation sequential 125I radioactive seed implantation for invasive breast cancer with ipsilateral axillary lymph node metastasis: Case report
Xiao-Guang Li*; Yu-Feng Wang
Department of Minimally Invasive Tumor Therapies Center, Beijing Hospital, National Center of Gerontology, Institute of Geriatric Medicine, Chinese Academy of Medical Sciences, and Peking Union Medical College, Chinese Academy of Medical Sciences, Beijing, China.
*Corresponding Author : Xiao-Guang Li
Department of Minimally Invasive Tumor Therapies Center, Beijing Hospital, National Center of Gerontology, Institute of Geriatric Medicine, Chinese Academy of Medical Sciences, 1 Dahua Street, Dongcheng District, Beijing, 100370, China.
Email: xglee88@126.com
Received : Mar 05, 2025
Accepted : Mar 26, 2025
Published : Apr 02, 2025
Archived : www.jcimcr.org
Copyright : © Xiao-Guang L (2025).
Abstract
Microwave ablation and 125I radioactive seed implantation are two well-established minimally invasive interventional techniques that are widely used for multi-system solid tumors. This case presents an 85-year-old elderly female breast cancer patient with axillary lymph node metastasis. She underwent a combination of microwave ablation for intramammary lesions and sequential radioactive particle implantation in enlarged axillary lymph nodes. During the follow-up period, no systemic therapy was combined, imaging did not indicate any recurrence, no adverse events occurred, and the patient tolerated the treatment well. This case may provide a new therapeutic idea for the clinical management of elderly breast cancer patients.
Keywords: Breast cancer; Microwave ablation; Radioactive seed.
Citation: Xiao-Guang L, Yu-Feng W. Microwave ablation sequential 125I radioactive seed implantation for invasive breast cancer with ipsilateral axillary lymph node metastasis: Case report. J Clin Images Med Case Rep. 2025; 6(4): 3535.
Introduction
Breast cancer is a prevalent malignant tumor and has the highest incidence rate among females [1]. Early-stage breast cancer usually has no typical signs and symptoms and prone to be ignorance. It is generally identified through a physical examination or imaging screening. Patients often inadvertently discover a single, firm, irregularly shaped, and superficially uneven mass in the breast. Most breast cancers present as painless lumps, with only a few causing vague or stabbing pain. More than 1/3 of breast cancer patients admitted to hospitals have axillary lymph node metastasis. Firm, scattered, moveable, enlarged axillary lymph nodes may be palpated in the early stage. The lymph nodes gradually fuse and become adherent to the surrounding tissues as the disease progresses. In advanced stages, metastatic lymph nodes may be palpated in the supraclavicular and contralateral axilla [2]. The combination of CA15-3 and CEA significantly increases the sensitivity for detecting tumor recurrence and metastasis. However, it can be elevated in benign diseases and other malignant tumors, making it unsuitable for breast cancer screening and diagnosis. Ultrasound is indicated for all suspected breast lesions and can be performed on both the breast and axillary lymph nodes. Furthermore, ultrasound-guided fine needle or hollow core aspiration biopsy can help confirm the diagnosis [3]. Immunohistochemical staining for Estrogen Receptor (ER), Progesterone Receptor (PR), and HER-2 should be performed in all cases of invasive breast cancer. Assessment helps identify the patients who will benefit from endocrine or targeted therapy. Treatment strategies available: [1] Mastectomy with breast preservation plus Radiation Therapy (RT); [2] Modified radical mastectomy with breast reconstruction as appropriate; [3] Total mastectomy with Sentinel Lymph Node Biopsy (SLNB); [4] Elderly breast cancer: Localized enlarged or total mastectomy with SLNB as appropriate. Patients with positive estrogen-progestin receptors require endocrine therapy administration.
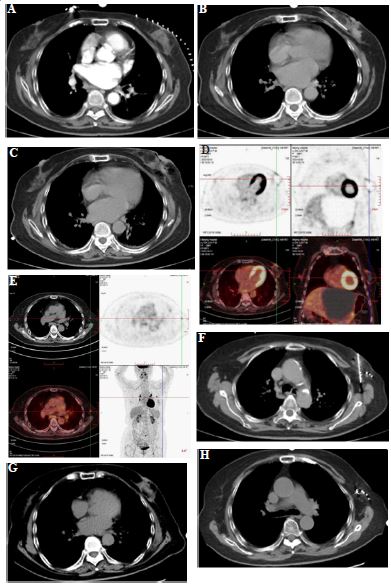
(B) The antenna was punctured into the lesion for ablation with parameters: 30w/5mins, 30w/5mins, 30w/2mins.
(C) Repeat CT plain scan after ablation: the lesion was adequately ablated, and the ablated area was hypodense, accompanied by a small amount of fluid exudation.
(D/E) The localized glands in the left breast were dense, with a circumferential increase in radioactivity uptake, SUVmax 4.0. The left axillary lymph nodes demonstrated increased radioactive uptake, with a diameter of approximately 0.5 cm and a SUVmax of 5.8.
(F) An 18G needle was punctured into the axillary lymph nodes and 20 radioactive 125I seeds (0.6 mCi, 120 Gy) were implanted.
(G/H) One year later, CT examination showed irregular streaky shadow in the left breast and multiple dense shadows in the left axilla, with no signs of disease recurrence.
Case report
The 85-year-old female, ultrasonography detected a solid nodule in the left breast, 2.1×1.5×1.3 cm, BI-RADS grade 4c; left axillary lymph node, 0.5×0.4 cm, metastasis considered. Biopsy results indicate: Left breast infiltrating ductal carcinoma (Grade II), immunohistochemistry results: ER (90%), PR (30%), HER-2 (1+), Ki67 (20%), P63 (-+); left axillary lymph node metastatic cancer, pT2N1aM0IIB stage, Luminal B-type. The patient refused surgical resection due to advanced age. She was admitted to our center for minimally invasive treatment. Contrast-enhanced CT scans were performed to locate the target lesion. A MWA antenna was punctured into the lesion. Place an ice pack on the surface of the breast. MWA was then performed on 3 sites under ultrasound monitoring, parameters: 30w 5 mins, 30w 5 mins, 30w 2 mins. The CT scan showed coverage of tumor volume postoperatively. One month later, the patient was admitted to our therapy center again. After completing the preoperative examinations, under CT guidance, an 18G needle was punctured into the axillary lymph nodes, and 20 radioactive 125I seeds (0.6 mCi, 120 Gy) were implanted. Regular outpatient follow-ups were conducted. The patient received no systemic treatment after two interventions, and the imaging review showed no signs of recurrence.
Discussion
Breast cancer is the most common malignant tumor among women. Treatment protocols for breast cancer are multimodal and multidisciplinary. In general, patients with early-stage breast cancer are curable, including reserved mastectomy/mastectomy and SLNB with RT as appropriate. Adjuvant systemic therapy may be administered based on tumor characteristics, such as size, grade, number of involved lymph nodes, and the expression status of ER/PR and HER-2 receptors. Clinically, elderly females tend to have larger lesions with lymph node involvement [4]. The guidelines recommend local extended or total mastectomy (based on surgical and anesthetic risk), endocrine therapy for receptor-positive patients, and SLNB as appropriate. However, the elderly often receive relatively conservative treatments that do not strictly adhere to clinical guidelines [5]. Radiotherapy following partial mastectomy is now a standard treatment and is well tolerated by patients. In a randomized trial, breast-conserving mastectomy was performed on elderly patients with T1N0M0 breast cancer. Patients who received tamoxifen and radiotherapy after mastectomy had a recurrence rate of 2% compared to 10% with tamoxifen alone [6,7]. Approximately 85% of elderly female patients express ER/PR receptors, while fewer than 10% have HER-2 overexpression. Patients with ER/PR-positive receptors ought to receive endocrine therapy regardless of age [8]. Endocrine therapy reduces the 10-year risk of recurrence and breast cancer-specific mortality in the elderly [9]. Cardiotoxicity, neurologic impairment, renal impairment, and myelosuppression are adverse events that require vigilance. It may lead to more severe toxicities in the elderly, but this does not materially affect the advantages of adjuvant chemotherapy. For some patients with high-risk features and a life expectancy of more than 5 years, some scholars recommend chemotherapy [10]. Targeted therapy can improve the prognosis of patients with HER-2 overexpression. In patients over 60 years old, trastuzumab reduced the relative risk by 47%, but the incidence of serious cardiotoxicity was 5%. In patients over 70 years old, the incidence of cardiotoxicity was 20%, but it may be associated with the simultaneous administration of anthracyclines [11]. The elderly are subject to challenges when making clinical decisions. Individualized protocols are necessary, considering co-morbidities, physical condition, and life expectancy, rather than just age. Hence, the MWA sequential radioactive seed implantation protocol was implemented for this patient. MWA induces coagulative necrosis of tumor tissues through hyperthermia and is widely utilized for multi-system solid tumors, such as the liver, kidneys, and lungs. For lesions ≤3 cm it is even comparable to surgical resection [12-14]. Compared to surgical resection, its’ advantages include less trauma, shorter procedure time, repeatability, and good tolerance. Radioactive 125I seed implantation is a low-dose, continuous irradiation, and repeatable internal radiotherapy technique. Compared with external beam radiation,125I seeds can increase the radiation dose in the tumor target region. The radiation dose in the target region is relatively high, while the surrounding tissues only experience mild damage [15]. By sequential application of the two interventional techniques, primary lesions and lymph node metastases of breast cancer were well controlled. Endocrine therapy, targeted therapy, and chemotherapy were not administered. There was no recurrence and no grade II-IV adverse event during follow-up. The protocol may provide new ideas for the management of elderly breast cancer patients.
Conflicts of interest: The authors declare no conflicts of interest associated with this work.
References
- The Society of Breast Cancer China Anti-Cancer Association, Breast Oncology Group of the Oncology Branch of the Chinese Medical Association. Guidelines for breast cancer diagnosis and treatment by China Anti-cancer Association (2024 edition) [J]. Chin Oncol. 2023; 33(12): 1092-1187.
- Bar zaman K, Karami J, Zarei Z, et al. Breast cancer: Biology, biomarkers, and treatments. Int Immunopharmacology. 2020; 84: 106535.
- National Health Commission of the People’s Republic of China. Guidelines for the Diagnosis and Treatment of Breast Cancer (2022 edition) [J]. Chin J Cancer Res. 2022; 10(19): 1-20.
- Eppenberger-Castori S, Moore D H J, Thor A D, et al. Age-associated biomarker profiles of human breast cancer. [J]. Int J Biochem Cell Biol. 2002; 34(11): 1318-1330.
- Lavelle K, Sowerbutts AM, Bundred N, et al. Is lack of surgery for older breast cancer patients in the UK explained by patient choice or poor health? A prospective cohort study. [J]. Br J Cancer. 2014; 110(3): 573-583.
- Kunkler IH, Audisio R, Belkacemi Y, et al. Review of current best practice and priorities for research in radiation oncology for elderly patients with cancer: the International Society of Geriatric Oncology (SIOG) task force. Ann Oncol. 2014; 25(11): 2134-2146.
- Hughes KS, Schnaper LA, Bellon JR, et al. Lumpectomy plus tamoxifen with or without irradiation in women age 70 years or older with early breast cancer: long-term follow-up of CALGB 9343. J Clin Oncol. 2013; 31(19): 2382-2387.
- Mouridsen H, Chaudri-Ross HA. Efficacy of first-line letrozole versus tamoxifen as a function of age in postmenopausal women with advanced breast cancer. Oncologist. 2004; 9(5): 497-506.
- Wildiers H, Kunkler I, Biganzoli L, et al. Management of breast cancer in elderly individuals: recommendations of the International Society of Geriatric Oncology. Lancet Oncol. 2007; 8(12): 1101-1115.
- Muss HB, Berry DA, Cirrincione C, et al. Toxicity of older and younger patients treated with adjuvant chemotherapy for node-positive breast cancer: the Cancer and Leukemia Group B Experience. J Clin Oncol. 2007; 25(24): 3699-3704.
- Denegri A, Moccetti T, Moccetti M, Spallarossa P, Brunelli C, et al. Cardiac toxicity of trastuzumab in elderly patients with breast cancer. J Geriatr Cardiol. 2016; 13(4): 355-363.
- Bertolotti L, Bazzocchi MV, Iemma E, et al. Radiofrequency Ablation, Cryoablation, and Microwave Ablation for the Treatment of Small Renal Masses: Efficacy and Complications. [J]. Diagnostics (Basel), 2023; 13(3).
- Peng JZ, Wang CE, Bie ZX, et al. Microwave Ablation for Inoperable Stage I Non-Small Cell Lung Cancer in Patients Aged ≥70 Years: A Prospective, Single-Center Study. J VASC INTERV RADIOL. 2023; 34(10): 1771-1776.
- Wicks JS, Dale BS, Ruffolo L, et al. Comparable and Complimentary Modalities for Treatment of Small-Sized HCC: Surgical Resection, Radiofrequency Ablation, and Microwave Ablation. J Clin Med. 2023; 12(15): 5006.
- Wang Z, Lu J, Gong J, et al. CT-guided radioactive ¹²⁵I seed implantation therapy of symptomatic retroperitoneal lymph node metastases. Cardiovasc Intervent Radiol. 2014; 37(1): 125-131.