
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Unexpected presence of colloid-laden macrophages in lymph nodes following follicular thyroid carcinoma: A rare case report
Mehrnoosh Ebadi1; Marino Leon2*
1Department of Anatomy and Cell biology, Carver College of Medicine, University of Iowa Health Care, 51 Newton Road, 100 Bowen Science Building, Iowa City, IA 52242, USA.
2Department of Pathology, Immunology and Laboratory Medicine, College of Medicine, University of Florida Health, 1600 SW Archer Rd, Gainesville, FL 32610, USA.
*Corresponding Author : Marino Leon
Department of Pathology, Immunology and Laboratory Medicine, College of Medicine, University of Florida Health, 1600 SW Archer Rd, Gainesville, FL 32610, USA.
Email: marino.leon@ufl.edu
Received : Mar 06, 2025
Accepted : Mar 27, 2025
Published : Apr 03, 2025
Archived : www.jcimcr.org
Copyright : © Leon M (2025).
Abstract
We present a case report of a 67-year-old woman who was diagnosed of bilateral thyroid nodules. She underwent a total thyroidectomy; a 4 cm nodule was diagnosed as minimally invasive follicular thyroid carcinoma (FTC). Her resection was followed by radioactive iodine therapy and levothyroxine. Despite stopping her levothyroxine, her thyroid function remained stable. About a year after her surgery, new nodules were found bilaterally in her thyroid bed. A fine needle aspiration (FNA) was performed which showed follicular cells with atypia. A surgical resection these bilateral thyroid bed nodules and lymph nodes was performed. The resected nodules were benign; however, the lymph nodes showed sinusoisal macro- phages/histiocytes with cytoplasmic thyroid colloid content. This finding was unusual because FTC typically spreads through the blood to organs like the lungs and bones, not through the lymph nodes. Further testing confirmed that these macrophages were not cancerous but benign immune cells that had likely phagocytize thyroid colloid material disrupted during her initial surgery and radioactive iodine therapy. These findings prevented unnecessary additional treatment. This rare finding adds to the understanding of how post-surgical changes can look unusual under the microscope, sometimes mimicking signs of cancer recurrence. For patients like this woman, recognizing these harmless cells helps prevent over-treatment and allows doctors to focus on genuine concerns. Her case highlights the importance of careful tissue evaluation and the role of the immune system in healing after surgery.
Citation: Ebadi M, Leon M. Unexpected presence of colloid-laden macrophages in lymph nodes following follicular thyroid carcinoma: A rare case report. J Clin Images Med Case Rep. 2025; 6(4): 3536.
Introduction
Follicular Thyroid Carcinoma (FTC) is a form of thyroid cancer known for its follicular structure and has potential for hematogenous metastasis. Papillary thyroid carcinoma usually spreads via lymphatics, but FTC shows and presents with distant metastases, including to the lungs and bones [1]. Occasionally, FTC may be challenging to differentiate the residual or recurrent disease from benign post-surgical changes or residual thyroid tissue. Colloid-laden macrophages in cases of FTC in lymph nodes are an unusual finding. Typically, thyroid colloid exists in thyroid follicles, and its migration to lymph nodes is uncommon. This phenomenon may be due to extensive disease activity or effects of therapeutic interventions. While colloidladen macrophages are associated with benign conditions like residual thyroid tissue or post-surgical changes, their presence in lymph nodes post- FTC surgery is rarely documented [2]. We describe a patient with FTC who underwent total thyroidectomy followed by radioactive iodine therapy. After normalization of thyroid function tests despite withdrawal of levothyroxine, new nodules were found in the thyroid bed. An FNA was performed and showed atypia of undetermined significance (AUS). The resection revealed lymph nodes containing macrophages with cytoplasmic colloid-like material that tested positive for thyroglobulin. This finding was unusual and adds under- standing of the possible histologic findings in patients with surgically resected lymph nodes and may contribute to their appropriate FTC management. To our knowledge, this is the first report of colloid-laden macrophages within lymph nodes after thyroidectomy for FTC [3,4].
Case presentation
A 67-year-old female with thyroid nodules underwent a total thyroidectomy; a 4 cm nodule was diagnosed as minimally invasive follicular thyroid carcinoma (FTC). After surgery, she was treated with radioactive iodine and levothyroxine. After levothyroxine withdrawal, her thyroid function tests normalized. Eleven months after the initial thyroidectomy, new nodules were detected in the thyroid bed. An anterior neck and thyroid bed ultrasound revealed two nodules 1.9 cm and 1.8 cm, in the right and left thyroid bed, respectively.
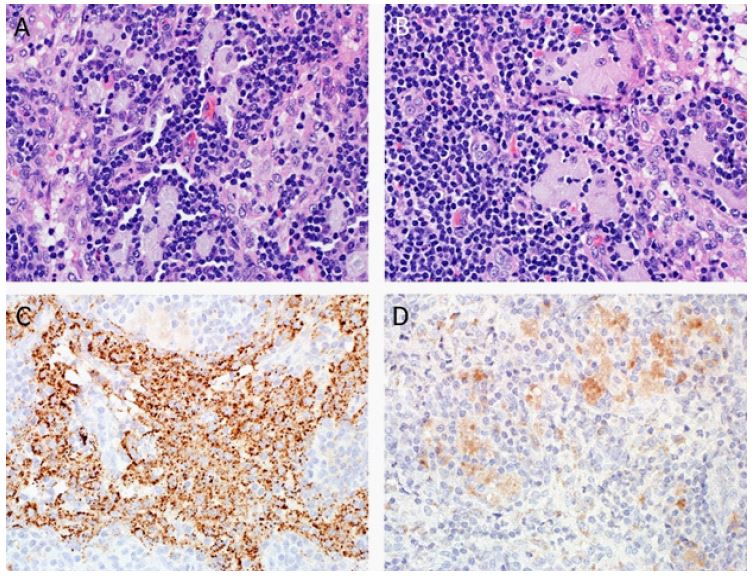
An FNA was performed; this material showed follicular cells with nuclear overlapping and scant colloid. This FNA cytology specimen was interpreted as atypia of undetermined significance. This finding led to a second surgical intervention. During the second surgery, the right thyroid nodule was resected. The pathology report revealed a hypercellular enlarged parathyroid gland and benign multinodular thyroid tissue. Additionally, seven right paratracheal lymph nodes were examined. While these lymph nodes were free of malignancy, they contained unusual cells that required further investigation. The lymph nodes showed sinusoidal epithelioid cells with a cytoplasmic colloid-like content. These cells were negative for mucicarmine, PAS, and PAS with diastase stains. On immunohistochemical stains, these cells were positive for CD68 and thyroglobulin; and they were negative for TTF-1, CDX-2, p63, and cytokeratins AE1/AE3 (Figure 1). These results indicated that these sinusoidal cells were benign histiocytes with phagocytized thyroid colloid consistent with colloid-laden macrophages/histiocytes. There was no evidence of residual malignancy in the lymph nodes. The incidental finding of colloid-laden macrophages/histiocytes in the lymph nodes provided a valuable insight into the spectrum of post-surgical tissue changes and did not impact the patient’s overall treatment plan or prognosis.
Discussion
This case adds a new histologic finding associated with the follow up of follicular thyroid carcinoma (FTC) and explains how unexpected findings can arise in post-surgical evaluations. The discovery of colloid-laden macrophages in the lymph nodes of a patient with FTC is unusual and is not widely documented in the literature. Typically, FTC metastasizes hematogenously, favoring distant sites such as the lungs or bones, rather than spreading via lymphatics [5]. The presence of colloid material in lymph nodes post-thyroidectomy could be perplexing, especially when considering that such findings are generally associated with benign thyroid conditions [6]. Firstly, it might be explained as a consequence of surgery, during the initial thyroidectomy, that might have led to disruption of the thyroid follicles allowing colloid material to leak and their secondary phagocytosis and transport by macrophages. This is consistent with prior observations that surgical trauma can alter the microenvironment and lead to unusual histopathological findings [7]. Also, radioactive iodine therapy may cause thyroid follicular cells destruction, tissue remodeling and subsequent release of colloid, its phagocytosis and transport via lymphatics to lymph nodes. However, the exact mechanism remains speculative and warrants further investigation. The presence of colloid-laden macrophages in lymph nodes might be misinterpreted as metastatic disease, particularly in cases where recurrence is a concern. This scenario emphasizes the importance of ancillary testing with immunohistochemical evaluation. In this patient, the positive staining for CD68 and thyroglobulin, along with negative staining for epithelial markers such as AE1/3, was key to distinguishing these cells from malignant ones [8]. This ancillary testing prevented unnecessary concern and ensured that the patient’s treatment plan remained appropriate and focused on true disease management. To our knowledge, this is the first reported case of colloid-laden macrophages in lymph nodes post-FTC surgery. While the finding did not alter the patient’s prognosis or overall management, it contributes valuable information to the growing body of literature on post-operative changes in FTC. Understanding these benign histological changes is crucial for clinicians to avoid misdiagnosis and over-treatment. Further case reports and studies are needed to determine if this phenomenon has any broader implications for prognosis or future treatment strategies in FTC management [9]. This case presents a unique and rare occurrence of colloid-laden macrophages in lymph nodes following follicular thyroid carcinoma (FTC) surgery. The appearance of these macrophages raises important considerations in the post- surgical evaluation of FTC patients, as these findings can potentially be mistaken for metastatic disease or recurrent malignancy. This case serves as a reminder that unexpected findings, while initially concerning, can sometimes be benign and should be approached with a balanced perspective. By sharing these observations, we hope to provide additional context and reassurance for clinicians who may encounter similar cases in their practice. The role of macrophages in the tumor microenvironment of thyroid cancers is complex and has gained increasing attention in recent years. Tumor-associated macrophages (TAMs) are a major component of the immune cell infiltration in thyroid cancers and can influence disease progression and therapeutic outcomes. TAMs typically exhibit a spectrum of activation states, ranging from the anti-tumorigenic M1 phenotype to the pro-tumorigenic M2 phenotype. In most thyroid cancers, including FTC, TAMs predominantly display the M2 phenotype, which is associated with tumor progression, angiogenesis, and immunosuppression [10]. In this case, the presence of colloid-laden macrophages might be attributed to post-surgical tissue remodeling, radioactive iodine therapy, or inflammatory processes, rather than an indication of disease metastasis or recurrence, as FTC does not usually metastasize to lymph nodes. Studies have shown that macrophages can phagocytose colloid material released from disrupted thyroid follicles, leading to their accumulation in lymph nodes [11]. This phenomenon may be attributed to the body’s response to surgical trauma or radioactive iodine therapy, both of which can alter the thyroid tissue environment and lead to unexpected histopathological findings. The clinical challenge lies in differentiating these histiocytes from malignant cells in the lymph nodes. In this context, immunohistochemical staining plays a useful role, as seen in this patient’s case, where staining for thyroglobulin and CD68 confirmed the benign nature of the cells. The use of appropriate ancillary studies is crucial for ensuring accurate diagnosis and avoiding unnecessary therapeutic interventions [12]. This report, to our knowledge, is among the first to describe colloid-laden macrophages in lymph nodes following FTC surgery. It highlights the importance of recognizing this phenomenon to prevent over-diagnosis and over-treatment. Further research is warranted to explore whether the presence of colloid-laden macrophages has any prognostic implications or specific association with treatment modalities like radioactive iodine therapy [10]. Overall, this case serves as a reminder of the complex interactions between tumor biology and the immune system in thyroid cancer, and the necessity for a nuanced approach to post-surgical lymph node evaluation to optimize patient care and outcomes.
References
- Hedinger C, Williams ED, & Sobin LH. Follicular Thyroid Carcinoma. In Histological Typing of Thyroid Tumours. 1988; 33-36.
- Zhang J, & Liu Y. Thyroglobulin as a Marker for Thyroid Cancer: Utility and Limitations. Endocrine Practice. 2014; 20(1): 65-72.
- Ramos J, & Trejo B. Residual Thyroid Tissue and Its Implications in Post-Surgical Monitoring. Thyroid. 27(8); 1041-1048.
- Morris LF, Yang W. Post-Surgical Thyroglobulin Elevation: Clinical Relevance and Management. Journal of Clinical Endocrinology & Metabolism. 2016; 101(7): 2552-2560.
- Smith J, Brown A, Thompson R. Hematogenous metastasis patterns in follicular thyroid carcinoma: A review of the literature. Thyroid Cancer Journal. 2019; 12(4): 178-184.
- Johnson M, Harris L. Understanding benign lymph node changes following thyroid surgery: A focus on colloid-laden macrophages. Endocrine Pathology. 2020; 31(2): 125-132.
- Green D, Miller C, Park H. Surgical influences on thyroid microenvironment: The potential impact on post-operative findings. Surgical Oncology Reviews. 2018; 5(3): 215-223.
- Jones P, White A, Robinson T. Immunohistochemical markers in thyroid pathology: Diagnostic and prognostic implications. Diagnostic Pathology. 2017; 12(1): 58.
- Hernandez E, Lopez G, Patel K. Post-surgical changes in thyroid cancer patients: Case reports and literature review. Journal of Thyroid Research. 2021; 16(2): 101-109.
- Liu Q, Zhang H, Sun W. Roles and new insights of macrophages in the tumor microenvironment of thyroid cancer. Frontiers in Pharmacology. 2022; 13: 875384.
- Wei S, LiVolsi VA, Baloch ZW. Pathology of thyroglossal duct: An institutional experience. Endocrine Pathology. 2015; 26: 75-79.
- Chou J, Walters A, Hage R, et al. Thyroglossal duct cysts: Anatomy, embryology, and treatment. Surgical Radiology Anatomy. 2013; 35: 875-881.