
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Bone marrow amyloidosis masquerading as visceral leishmaniasis: An enigma of a big spleen disease
Sujata Raychaudhuri; Aparna Singh2; Tathagata Chatterjee3*; Dipti Sidam3; Mukta Pujani3
1Professor, Pathology, ESIC Medical College and Hospital, Basaidarapur, New Delhi, India.
2Assistant Professor, Pathology, ESIC Medical College and Hospital, Faridabad, India.
3Professor, Pathology, ESIC Medical College and Hospital, Faridabad, India.
*Corresponding Author : Tathagata Chatterjee
Professor, Pathology, ESIC Medical College and Hospital, Faridabad, India.
Email: ctathagat@hotmail.com
Received : Mar 07, 2025
Accepted : Mar 28, 2025
Published : Apr 04, 2025
Archived : www.jcimcr.org
Copyright : © Chatterjee T (2025).
Abstract
Background: Massive splenomegaly can be caused by various infectious, inflammatory and systemic disorders but is a rare occurrence due to underlying amyloidosis. Amyloidosis is due to the defective or unusual folding of amyloid proteins and is characterized by abnormal deposition of anomalous proteins.
Case report: A 53-year-old man presented with complains of fever on and off for the past nine months with massive hepatosplenomegaly, generalized weakness, anorexia, nausea and vomiting. There was progressive increase in urea and creatinine and episodic increase in SGOT and SGPT. On CECT abdomen, multiple well defined hepatic lesions were seen showing discontinuous, nodular and peripheral enhancement along with splenomegaly. A complete blood count with peripheral smear, serial liver and kidney function tests, serology and blood cultures were done including rk39 for kala-azar which was negative. Giemsa-stained bone marrow smears revealed extensive homogenous aggregates of bluish staining material with reduced marrow cellularity. A diagnosis of bone marrow amyloidosis with an increase in lymphohistiocytic activity was rendered. The bone marrow biopsy showed extensive extracellular eosinophilic amorphous deposits which were Congo red positive and retained the stain after reduction with KMNO4 favoring AL type amyloidosis. The IHC stains were positive for CD138, CD38 and showed kappa restriction .M spike was noted in Serum electrophoresis . Kidney biopsy revealed amyloid deposits with apple green birefringence on polarized microscopy which confirmed the diagnosis.
Conclusion: This rare case gave an insight to rule out amyloidosis in patients not responding to the usual treatment for massive hepatosplenomegaly.
Keywords: Hepatosplenomegaly; Bone marrow aspiration; AL type amyloidosis.
Citation: Raychaudhuri S, Singh A, Chatterjee T, Sidam D, Pujani M. Bone marrow amyloidosis masquerading as visceral leishmaniasis: An enigma of a big spleen disease. J Clin Images Med Case Rep. 2025; 6(4): 3539.
Introduction
Amyloidosis is a spectrum of protein disorders which are characterized by abnormal deposition of anomalous proteins. Due to the defective or unusual folding of amyloid protein it is also referred to as protein folding and conformational disorders [1]. These abnormal protein deposits form similar eosinophilic clusters, and stains positive with Congo red dye and demonstrate apple-green birefringence under polarized microscope due to the characteristic β-pleated sheet structure of these molecules [2]. The systemic amyloidosis can have varied etiology which may range from primary immunocyte dyscrasias to several chronic inflammatory condition. It may also be the result of mutation in the non-amyloid protein or may arise from genetic defect of the amyloid protein itself [3]. The type of amyloidosis is essential to know the etiology of amyloidosis to treat the underlying systemic condition. There are 36 different fibrillary proteins which are amyloidogenic in nature [4]. The various types of amyloidosis are AL type associated immunocyte or plasma cell dyscrasia, serum amyloid A protein associated with chronic inflammation (AA types), hereditary or sporadic mutations in different genes encoding for soluble proteins, such as transthyretin amyloidosis (ATTR), fibrinogen amyloidosis (AFib), apolipoprotein A1 amyloidosis (AApo A1), gelsolin amyloidosis (AGel), cystatin C amyloidosis (ACys), and lysozyme amyloidosis (ALys) [5]. Of these, AL type is the most prevalent followed by ATTR [6].
Massive splenomegaly can be caused by various kinds of infectious diseases, infiltrative disorders, pooling of blood and hepatic disorders. The case is presented to unravel the cause of a hepatosplenomegaly with history of prolonged illness in an elderly man not responding to treatment.
Case report
A 53 year old male presented with episodic fever since 9 months and received treatment for typhoid. However, he complained of persistent generalized weakness, headache and anorexia. Clinically, he presented with hypertension and on physical examination there was massive hepatosplenomegaly and on CECT abdomen, liver was more than 26 cm and spleen were more than 14 cm in size. There was evidence of renal failure in the last 6 months and ultrasound revealed reduction in the size of the kidneys. There was a progressive rise in serum creatinine and urea with episodic increase in serum potassium and serum SGOT and SGPT. Serum Urea was 143 mg/dl and Creatinine was 5.55 mg/dl. Albumin and globulin values were 3.95 g/dl and 5.05 g/dl respectively. Total Serum protein was 9 g/dl, but lipid values were normal. Also, there were complaints of itching all over the body and increased frequency of urination and urge to pass stools along with inability to eat well and early satiety. The lab tests revealed an elevated total serum Bilirubin of 1.64 mg/dl along with SGOT and SGPT values of 49 mg/dl and 78 mg/dl respectively, but the viral markers were negative. The hemoglobin was 15.5 g/dl, TLC-19570 with 84% neutrophils and PCV was 46.3%. No hemiparasites were seen. Based on clinical features of massive hepatosplenomegaly, fever and wasting an infiltrative or infective etiology was suggested. To rule out the infectious causes, complete blood tests, blood culture and rk39 antigen detection by ELISA for leishmaniasis, anti-HbsAg, anti-HCV and anti-HIV antibodies were advised. However, none of these tests were positive. Bone marrow aspiration revealed extensive bluish deposits on Giemsa stain and bone marrow biopsy showed eosinophilic material which confirmed the diagnosis of amyloidosis using Congo red stain and apple green birefringence.
Discussion
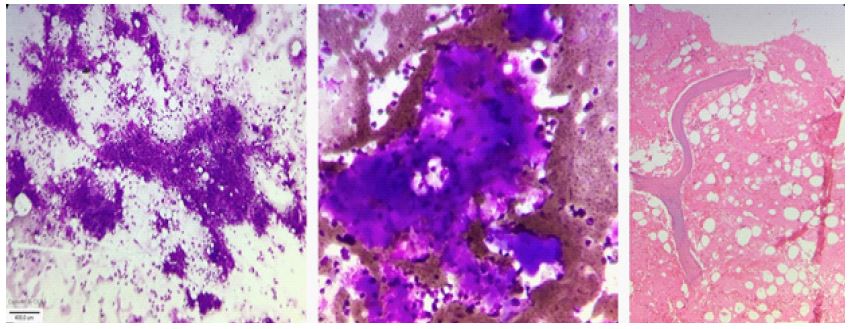
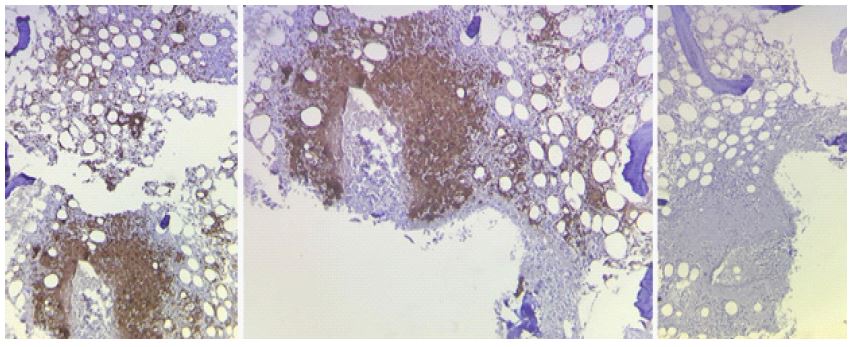
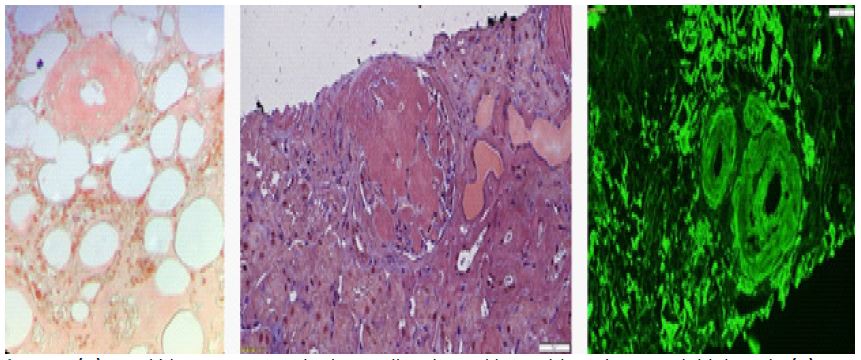
Renal amyloidosis is one of the most important causes of progressive renal failure and massive proteinuria in the elderly [1]. It can be the dominant manifestation in various forms of systemic amyloidosis [7]. Several types of amyloidosis are present with different clinical manifestations. In the present case the patient presented with episodic fever and increased frequency of urination and passage of stools reflecting repeated infections, itching all over the body due to rise in bilirubin, secondary deranged liver functions associated with hepatomegaly and early satiety and inability to eat due to fullness in the left hypochondrium associated with splenomegaly. Enlargement of spleen with fever, features of infection and cachexia aroused the clinical suspicion of leishmaniasis and all investigations including CBC with PS, BMA and bone marrow biopsy along with biochemical and serological tests were undertaken. Bone marrow aspirate revealed extensive deposits of bluish staining amorphous material on Giemsa-stained smears and a diagnosis of bone marrow amyloidosis was given (Figures 1a and 1b). Bone marrow biopsy also revealed abundant extensive extracellular eosinophilic deposits (Figure 1c). When Congo red staining was done on bone marrow biopsy, it appeared pink on light microscopy in the areas of amorphous deposits. This pale pink stain was retained after KMNO4 reduction proving that the amyloid was AL type. Serum electrophoresis showed an M spike confirming the plasma cell dyscrasias as the underlying cause. On Immunohistochemistry, the lymphoid cells showed focal positive expression for CD38 and CD138, were Kappa restricted and Lambda negative (Figures 2a, 2b, 2c). There was focal aberrant expression of CD56 and CD20 was negative. It is not always necessary to biopsy the different deeper systemic sites like kidney or heart as bone marrow or pad of fat is easily accessible and amyloid is easily detected [8]. However, Kidney biopsy was advised in the present case. Positive staining with Congo red was noted both in the bone marrow biopsy (Figure 3a) and in the glomeruli and interstitium. Amyloid deposits were noted in H&E section and appeared pink on light microscopy (Figure 3b) and these deposits gave an apple green birefringence on polarized microscopy (Figure 3c). All other investigations were normal with no evidence of Leishmaniasis on serology or on bone marrow aspiration and biopsy.
The case is discussed due to its rarity. It is unusual for bone marrow amyloidosis to present as a big spleen disease in the elderly. To our knowledge, there are only a few case reports in the literature with splenomegaly as the first symptom for bone marrow amyloidosis. The presence of amyloid deposits on the bone marrow aspirate itself helped clinch the prompt diagnosis and rule out other causes of big spleen disease in an elderly patient. The frequency of AL type and non-AL type amyloid can be based on proteomics typing of bone marrow [8].
Timely diagnosis helped in the treatment for AL amyloidosis which could be offered at the earliest in the form of Daratumumab, Cyclophosphamide, Bortezomib and dexamethasone.
Conclusion
The first sign of AL amyloidosis can be splenomegaly, and an early timely diagnosis can be obtained by proper bone marrow studies along with radiology paired with special stains, Immunohistochemistry and protein electrophoresis. Treatment with Bortezomib and dexamethasone in the case of AL amyloidosis can be life saving.
References
- Herrera GA, Teng J, Turbat-Herrera EA. Renal amyloidosis: current views on pathogenesis and impact on diagnosis. ContribNephrol. 2011;169:232-246. doi: 10.1159/000314795. Epub 2011 Jan 20. PMID: 21252523.
- Hawkins PN. Amyloidosis. Blood Rev. 1988 Dec; 2(4):270–80. https://doi.org/10.1016/0268-960x(88) 90016-1 PMID: 3061533
- M. M. Picken, “Amyloidosis-where are we now and where are we heading?” Archives of Pathology & Laboratory Medicine. 2010; 131(4): 545–551.
- Sipe, J. D., Benson, M. D., Buxbaum, J. N., Ikeda, S. ichi, Merlini, G., Saraiva, M. J. M., & Westermark, P. Amyloid fibril proteins and amyloidosis: chemical identification and clinical classification International Society of Amyloidosis 2016 Nomenclature Guidelines. Amyloid. 2016; 23(4): 209-213. https://doi.org/10.1080/13506129.2016.1257986
- Barreca A, Bottasso E, Veneziano F, Giarin M, Nocifora A, Martinetti N, Attanasio A, Biancone L, Benevolo G, Roccatello D, Cassoni P, Papotti MG; Amyloidosis Group of the “Rete InterregionalePiemonte e Valle d’Aosta per le Malattie Rare”. Immunohistochemical typing of amyloid in fixed paraffin-embedded samples by an automatic procedure: Comparison with immunofluorescence data on fresh-frozen tissue. PLoS One. 2021; 16(8): e0256306. doi: 10.1371/journal.pone.0256306. PMID: 34428239; PMCID: PMC8384180.
- Dasari S, Theis JD, Vrana JA, et al. Amyloid typing by mass spectrometry in clinical practice: a comprehensive review of 16,175 samples. Mayo Clin Proc. 2020; 95(9): 1852–1864.
- L. M. Lool. An investigation of the protein components of amyloid using immunoperoxidase and permanganate methods on tissue sections. Pathology. 1986; 19(1): 137–140.
- Chiu A, Dasari S, Kurtin PJ, Theis JD, Vrana JA, Dispenzieri A, Rech KL, Dao LN, Howard MT, Grogan M, McPhail ED. Bone marrow amyloid: a comprehensive analysis of 1,469 samples, including amyloid type, clinical features, and morphologic distribution. Amyloid. 2022; 29(3): 156-164. doi: 10.1080/13506129.2022.2031963. Epub 2022 Feb 9. PMID: 35135386.