
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Capsule endoscopy: A breakthrough in diagnosing metastatic melanoma
Nicholas Vanigli1*; Nikolas Dussias1; Paolo Gionchetti1,2; Fernando Rizzello1,2; Carlo Calabrese1,2
1IBD Unit, IRCCS Azienda Ospedaliero-Universitaria di Bologna, Italy.
2Department of Medical and Surgical and Sciences, University of Bologna, Bologna, Italy.
*Corresponding Author : Nicholas Vanigli
IBD Unit, IRCCS Azienda Ospedaliero-Universitaria di Bologna, Italy.
Email: nicholas.vanigli@studio.unibo.it
Received : Mar 07, 2025
Accepted : Mar 28, 2025
Published : Apr 04, 2025
Archived : www.jcimcr.org
Copyright : © Vanigli N (2025).
Abstract
Metastatic melanoma of the gastrointestinal tract is rare and often diagnosed late due to nonspecific symptoms. This report describes the case of a 66-year-old male with a history of cutaneous melanoma who presented with anemia and a positive fecal occult blood test. Conventional endoscopic evaluation yielded no significant findings, whereas video capsule endoscopy identified a small bowel lesion subsequently confirmed as metastatic melanoma. The patient underwent laparoscopic resection and initiated immunotherapy. This case highlights the potential role of VCE in early detection of small bowel melanoma metastases, emphasizing its relevance in improving diagnostic accuracy and guiding clinical management.
Keywords: Capsule endoscopy; Obscure gastrointestinal bleeding; Melanoma; Small bowel metastasis.
Abbreviations: MM: Metastatic Melanoma; VCE: Capsule Endoscopy; SBMM: Small Bowel Metastatic Melanoma; MRI: Magnetic Resonance; PET: Positron Emission Tomography; CT: Computed Tomography.
Citation: Vanigli N, Dussias N, Gionchetti P, Rizzello F, Calabrese C. Capsule endoscopy: A breakthrough in diagnosing metastatic melanoma. J Clin Images Med Case Rep. 2025; 6(4): 3540.
Introduction
Melanoma is the most serious form of skin cancer worldwide. It accounts for 1-3% of all tumors and has an unusual predilection to metastasize to the gastrointestinal tract. [1] The incidence of malignant melanoma has been increasing in white populations, and in cases of Metastatic Melanoma (MM), the prognosis is very poor. The diagnosis of MM to the gastrointestinal tract is usually difficult due to nonspecific symptoms and the lack of endoscopic investigations of the small bowel. [2] Early detection of small bowel melanoma remains a challenge for both radiologists and clinicians. Small bowel Video Capsule Endoscopy (VCE) is a minimally invasive method for the intraluminal visualization of the entire small bowel. VCE can be a useful tool for detecting small bowel tumors, both primary and metastatic. We report a case of small bowel metastatic melanoma (SBMM) detected through VCE. [3].
Case report
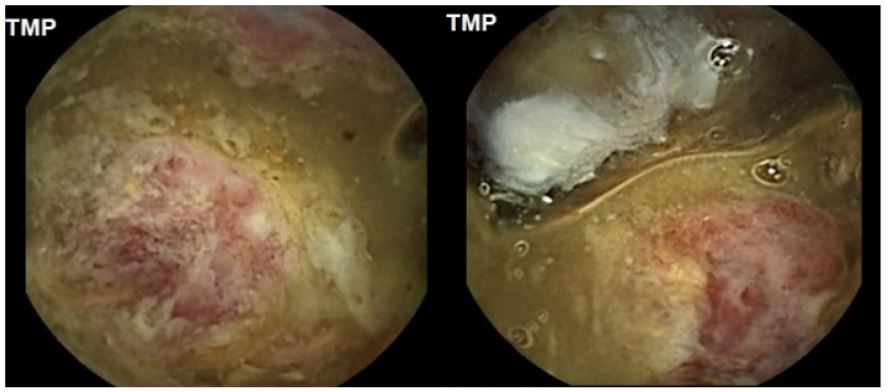
A 66-year-old male with a history of type 2 diabetes mellitus, hypertension, and prior resection of a cutaneous nodular melanoma on his right arm in 2017 (stage II, pT3bN0M0), presented to our clinic with iron-deficiency anemia and positive fecal occult blood. Due to his history of melanoma and anemia, an extensive workup was performed, including esophagogastroduodenoscopy and colonoscopy, both of which were normal, except for the presence of two small sessile polyps. Given his prior negative workup, a VCE was performed, revealing a large edematous and ulcerated area with disruption of the pit pattern in the second tertile (5 hours and 3 minutes from the pylorus) (Figure 1).
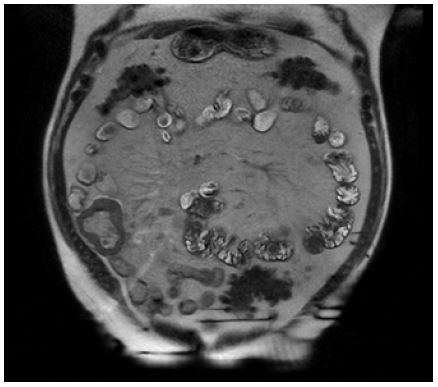
As part of the diagnostic evaluation, Magnetic Resonance (MRI) enterography showed a dilated portion of the distal ileum measuring 58 x 4 x 62 mm, without evidence of obstruction or significant upstream bowel dilation. The scan also revealed diffuse and irregular thickening of the visceral wall (approximately 12 mm) with contrast enhancement and marked signal restriction on diffusion. Several mesenteric lymph nodes were noted (Figure 2).
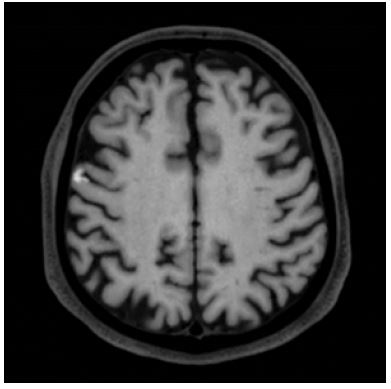
After multidisciplinary evaluation, the patient underwent an elective videolaparoscopic resection, including the pathological-appearing loop, with the creation of an extracorporeal side-to-side ileo-ileal anastomosis using a mechanical stapler through a service minilaparotomy. Histological examination of the mass revealed an intestinal localization of epithelioid melanoma, infiltrating the full thickness of the intestinal wall, with focal extension into perivisceral fat. The neoplasm is immunoreactive to SOX-10, Prame, S-100, and vimentin, and negative for CKAE1-AE3 and CD45. Finally, the patient underwent a PET scan and brain MRI, which revealed a small hemorrhagic lesion of 7 mm with minimal satellite edema in the cortical area of the right frontal third convolution, characterized by moderate enhancement after administration of contrast agent (Figure 3).
Based on brain MRI findings and evaluation by neurosurgeons and radiotherapists, stereotactic radiotherapy using CyberKnife was chosen for the single brain lesion. Additionally, first-line chemotherapy with nivolumab (1 mg/kg) and ipilimumab (3 mg/kg) was scheduled through the oncology service.
Discussion
Here we discuss a case of SBMM diagnosed by VCE.
MM represents an advanced stage of melanoma that generally carries a poor prognosis. According to the American Cancer Society, the current five-year survival rate for MM is estimated to be 32%. [4] Additionally, although around 60% of patients who die from melanoma present with gastrointestinal metastases, only 1.5-4.4% of gastrointestinal tract metastases are detected before death. [5] Therefore, it is essential that bowel metastases are recognized as early as possible. [5] Gastrointestinal metastases often present insidiously with nonspecific complaints such as intermittent abdominal pain, anemia, bleeding, obstruction, hematemesis, melena, anemia, fatigue, weight loss, or the presence of a palpable abdominal mass. Consequently, the diagnosis is not straightforward and often takes time; in fact, the interval between the diagnosis of primary melanoma and the identification of bowel metastases can vary from 2 to 180 months. [6] Currently, there are no standardized protocols for the diagnosis of SBMM and regular radiographic screening for intestinal metastases is not recommended for patients with primary cutaneous melanoma or for those with MM who do not exhibit gastrointestinal symptoms. Diagnosis typically relies on endoscopic examinations and various imaging techniques, including abdominal ultrasound, barium studies, MRI enterography, CT, and PET-CT, which are the most commonly used. [5] Transabdominal ultrasound and conventional barium enteroclysis are first-line tests for patients with vague abdominal symptoms; however, when used alone, they are not sufficient to confirm the diagnosis of SBMM. Cross-sectional imaging with CT has a sensitivity of 60-70% for detecting SBMM, with improved detection rates achieved through CT enteroclysis. [5] Whole-body PET imaging with fluorodeoxyglucose has higher sensitivity and specificity than CT for detecting gastrointestinal metastases in melanoma patients. However, neither CT nor PET-CT can detect all lesions, and conventional endoscopic studies identify only 10-20% of lesions. [7] VCE is a recent technique that allows for the investigation of segments of the intestine that cannot be examined with conventional endoscopy. VCE integrates cross-sectional imaging and, according to recent studies, has better diagnostic validity for identifying the presence and extent of SBMM compared to CT. In particular, Prakoso et al. demonstrated that VCE is superior to PET-CT scanning with 18F-fluorodeoxyglucose in identifying small intestinal involvement in patients with MM. [8] The same author showed that VCE can reveal new lesions undetected by other imaging modalities, suggesting that the combination of PET-CT and VCE may be the optimal approach for evaluating patients with gastrointestinal symptoms. [8,9] In addition, Aerts et al [10] demonstrated that VCE and PET-CT had comparable results in the diagnosis of SBMM; VCE was more sensitive in identifying luminal lesions, while PET-CT was more effective for mesenteric lesions. This finding reinforces the complementary nature of the two methods. Finally, the definitive diagnosis is confirmed by histological examination using immunohistochemical stains such as S-100 and HMB-45, which play a crucial role in confirming MM. [5] SBMM typically presents as multiple polypoid masses in the submucosal region. These can be both pigmented and amelanotic, with the latter being as common as the pigmented forms. Thus, the absence of pigmentation does not exclude the diagnosis. [5-11] Ulcerations and/or active bleeding may also be observed. Unlike our case, SBMMs rarely present as a solitary mass. In conclusion, the diagnosis of SBMM remains a significant challenge, highlighting the need for standardized protocols regarding the appropriate use of imaging and endoscopic investigations. VCE may play a future role as a screening tool for SBMM in patients with stage melanoma, especially those presenting with gastrointestinal symptoms.
References
- D Blecker, S Abraham, EE Furth, ML Kochman. Melanoma in the gastrointestinal tract, Am. J. Gastroenterol. 1999; 94(12): 3427-3433. doi: 10.1111/J.1572-0241.1999.01604.X.
- M Arnold et al. Global Burden of Cutaneous Melanoma in 2020 and Projections to 2040, JAMA Dermatology. 2022; 158(5): 495. doi: 10.1001/JAMADERMATOL.2022.0160.
- DY Cheung, JS Kim, KN Shim, MG Choi. The Usefulness of Capsule Endoscopy for Small Bowel Tumors,Clin. Endosc. 2016; 49(1): 21-25. doi: 10.5946/CE.2016.49.1.21.
- S Sundararajan, AM Thida, S Yadlapati, SKR Mukkamalla, S Koya. Metastatic Melanoma, StatPearls. 2024.
- M Lens, V Bataille, Z Krivokapic. Melanoma of the small intestine, Lancet. Oncol. 2009; 10(5): 516-521. doi: 10.1016/S1470-2045(09)70036-1.
- D Kohoutova, D Worku, H Aziz, J Teare, J Weir, J Larkin. Malignant Melanoma of the Gastrointestinal Tract: Symptoms, Diagnosis, and Current Treatment Options, Cells. 2021; 10(2): 1-10. doi: 10.3390/CELLS10020327.
- S Fernández Noël, et al. Capsule endoscopy diagnosis of gastrointestinal melanoma, Rev. Esp. enfermedades Dig. 2023; 115(12): 750-751. doi: 10.17235/REED.2023.9803/2023.
- E Prakoso, M Fulham, JF Thompson, WS Selby. Capsule endoscopy versus positron emission tomography for detection of small-bowel metastatic melanoma: A pilot study, Gastrointest. Endosc. 2011; 73(4): 750-756. doi: 10.1016/J.GIE.2010.11.028.
- E Prakoso, WS Selby. Capsule endoscopy in patients with malignant melanoma, Am. J. Gastroenterol. 2007; 102(6): doi: 10.1111/J.1572-0241.2007.01115.X.
- MA Aerts, F Mana, B Neyns, D De Looze, C Reenaers, et al. Small bowel metastases from melanoma : Does videocapsule provide additional information after FDG positron emission tomography ?”.
- E Prakoso, WS Selby. Polypoid and non-pigmented small-bowel melanoma in capsule endoscopy is common, Endoscopy. 2010; 42(11): 979. doi: 10.1055/S-0030-1255879/ID/5/BIB.