
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 6
Prediction of matrix metalloproteinase–7 to heart failure with preserved ejection fraction in uremic patients
Xinrui Wang1; Xiaomeng Li2; Dongjuan Zhang3; Lu Ma2; Yang Yang3*
1Clinical laboratory, Centre for Disease Prevention and Control of Chang’an District, Shijiazhuang, China.
2Doppler Ultrasonic Department, Beidaihe Rehabilitation and Recuperation Center of the Chinese People’s Liberation Army, Qinhuangdao, China.
3Hemodialysis Centre, 981th Hospital of Chinese People’s Liberation Army, Chengde, China.
*Corresponding Author : Yang Yang
Hemodialysis Centre, 981th Hospital of Chinese People’s Liberation Army, Chengde, China.
Tel: 018830453253; Email: yybjzy@163.com
Received : Mar 07, 2025
Accepted : Mar 31, 2025
Published : Apr 07, 2025
Archived : www.jcimcr.org
Copyright : © Yang Y (2025).
Keywords: Chronic kidney disease; Heart failure; Cardiac remodeling.
Citation: Xinrui W, Xiaomeng L, Dongjuan Z, Lu M, Yang Y. Prediction of matrix metalloproteinase–7 to heart failure with preserved ejection fraction in uremic patients. J Clin Images Med Case Rep. 2025; 6(4): 3541.
Description
Heart Failure (HF) in patients with chronic kidney disease (CKD) has an incidence ranging from 17% to 21% and includes HF with a preserved or reduced ejection fraction (HFpEF and HFrEF, respectively). Although extensive clinical and basic research has shed light on HFrEF, little is known about HFpEF [1]. This is likely due to the multifactorial character of HFpEF and a lack of knowledge of its pathophysiology in the CKD population. Many animal studies showed that 5/6-nephrectomy-operated rodents developed obvious Cardiac Remodeling (CR) and signs of HFpEF at 8 weeks postoperatively. The development of HFpEF is associated with progressive microvascular inflammation along with LV hypertrophy, cardiac remodeling (CR) and diastolic dysfunction [2,3]. We have reported that MMP7 plays a key role in the development of CR in uremic mice, through a mechanism that includes the activation of cardiac macrophages [4]. Thus, we designed a retrospective study in a cohort of Hemodialysis (HD) patients to investigate whether MMP7 is a biomarker that predicts the risk of HFpEF [5]. It was a single-center, retrospective, observational study from January to March of 2012. Incident HF was determined over the 4.5-year follow up, until December 2017. A consensus regarding a diagnosis of definite HF was reached by the nephrologists in accordance with the modified Framingham criteria. In 2019, the Heart Failure Working Group (HFA) of the ESC presented a new diagnostic algorithm with HFA-PEFF score to diagnosis HFpEF [6]. We calculated the HFA-PEFF score for every patient based on available data and a score over 5 would imply HFpEF. The Left Ventricular Ejection Fraction (LVEF) was calculated according to the modified Simpson method and HFrEF were defined as LVEF <40%. Measurements were taken using standard parasternal and apical views using a LOGIQ E9 ultrasound unit (GE Healthcare, Chicago, IL) equipped with M5S-D phased array transducers (1.6-4.2 MHz). LVEF was calculated using the modified biplane Simpson method. Cardiac diastolic function was evaluated using pulsed-wave Doppler imaging to calculate the ratio between peak E-wave and A-wave velocities (E/A). Lateral and septal early diastolic mitral annulus velocities (e’ lateral and e’ septal) were determined and the mean velocity (e’ mean) was derived. The LV filling index (E/e’ mean) was calculated from the collected parameters. Fasting blood samples were obtained under standardized conditions before HD. MMP7 kits were purchased from LifeSpan BioSciences (cat. no.: LS-F159; Seattle, WA), collagen type 1 kits from My BioSource (MBS164973; San Diego, CA), platelet factor-4 (PF4) kits from Biorbyt (orb562142; Cambridge, UK), and galectin 3 (GAL3) from LifeSpan BioSciences (LS-F442). The plasma N-terminal proB-type natriuretic peptide (NT-proBNP) concentration was determined using electrochemical luminescence immunoassay. Platelet-derived micro particles (PMPs) in the peripheral blood were detected via fluorescence-activated cell sorting using a BD FACSCalibur™ flow cytometer (Franklin Lakes, NJ). This retrospective study was based on a chart review of 450 patients, 383 of whom had been followed up for at least 4.5 years.7 HF was diagnosed in 16.7% of these patients (7.3% HFpEF and 9.4% HFrEF) during 4.5 years of HD (Figure 1A). The populations of patients combined diabetes and receiving aspirin (Figure 1B), HF biomarkers (NT-proBNP and GAL-3), platelet-activating parameters (PMPs and PF4), CR biomarkers (MMP7 and sCol-1, Figure 1C) differed significantly between patients with HFrEF and HFpEF. However, the cardiac function parameters (LVEF, E/A and E/e’) were similar at baseline between patients with HFrEF and HFpEF (Figure 1D). The baseline MMP7 level was an independent variable that predicted all cases of HF in HD patients (Figure 1E). The multivariate linear regression analysis for HF subtypes revealed that an elevated baseline MMP7 level was not associated with the incidence of HFrEF (adjusted odds ratio [OR]: 1.094, 95% CI: 0.852–1.238) but it was a strong predictive factor (adjusted OR: 1.282, 95% CI: 1.117–1.450) for HFpEF in HD patients when adjusted for age, sex, smoking habit, blood pressure, anti-platelet treatment, statin prescriptions, diabetes complications, and HD duration, frequency, and adequacy. The incidences of HFrEF (Figure 1F) and HFpEF (Figure 1G) were compared among groups differing in their MMP7 levels: >0–5.0, 5.1–10.0, 10.1–20.0, 20.1–35.0, and >35. Data on the dynamic echocardiographic changes during the 4.5 years of HD were available for all 383 patients and were used to evaluate the ability of MMP7 levels to predict a decline in cardiac function in HD patients. Systolic and diastolic dysfunction were assessed based on the changes in LVEF and E/A, respectively. After adjustments were made for age, sex, smoking habit, blood pressure, anti-platelet treatment, statin prescriptions, diabetes complications, and HD duration, frequency, and adequacy, the MMP7 level remained an independent variable for predicting declines in both LVEF and E/A; but the R-squared value of the predictive model associating MMP7 with LVEF decline was much lower than the values obtained for models with other variables, including PF4, PMPs, GAL3, NT-proBNP, or sCol-1. The opposite was the case for the models analyzing the ability to predict an E/A decline (Figures 1H, 1I). Collagen I is the primary substrate of MMP7 and its soluble hydrolyzed fragments can be detected in the circulation. We tested the combined ability of MMP7 and sCol-1 to predict cardiac function decline in HD patients. The results showed that the combination of MMP7 and sCol-1 was a more sensitive predictor of significant E/A decline than MMP7 alone. However, this same combination failed to predict changes in LEVF (Figures 1J, 1K). Emerging studies suggest that adverse CR involving ECM turnover results in high morbidity and mortality in patients with HF, and that MMPs play an important role in the process because of their ability to degrade ECM components. Soslow et al. showed that MMP7 levels are inversely correlated with LVEF in patients with Duchenne muscular dystrophy. Zile et al. found that, in patients with LV hypertrophy, those with elevated MMP7 levels exhibited an increase in LV structural remodeling [8]. We recently reported that PF4 and other platelet-derived particles significantly upregulate MMP7 expression by cardiac macrophages in uremic mice, resulting in the hydrolysis of cardiac collagen and the progression of CR during uremia.5 In the present study, HD patients with a broader range of MMP7 levels exhibited a more marked decline in E/A, a primary parameter for evaluating diastolic dysfunction, and were at a notably higher risk of HFpEF [9]. This study had several limitations. First, it was retrospective study and all serum specimens for enzyme-linked immunosorbent assay detection had been previously obtained. Second, the sample size was small, such that our conclusions remain to be confirmed in a larger, more comprehensive population.
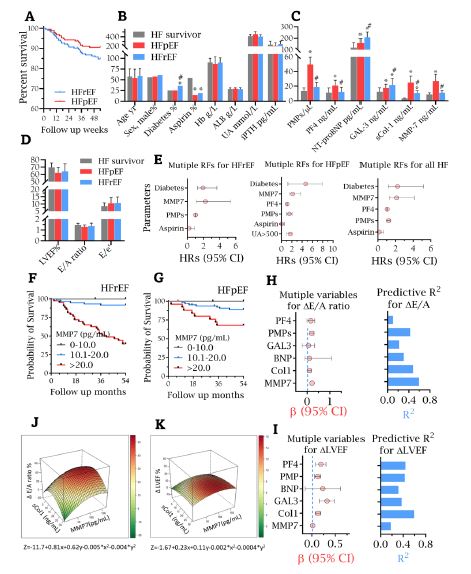
(A) The incidences of HFpEF, and HFrEF in HD patients during the 4.5 years of follow-up.
(B) The demographic and baseline clinical and experimental characteristics. (B) HF biomarkers, platelet-activating parameters and cardiac remodeling biomarkers at baseline.
(D) The echocardiographic parameters at baseline. * and # indicate significant difference compared with HF survivors and patients with HFpEF, respectively.
(E) Risk factor analysis for all HF cases, HFpEF, and HFrEF in HD patients. Multivariate logistic regression models were used to analyze the risk factors for all HF cases, HFpEF, and HFrEF in HD patients. In the multivariate analysis, the Hazard Ratios (HRs) and 95% confidence intervals (CIs) of the candidate HF variables were adjusted by age, sex, presence of a smoking habit, past cardiovascular disease events, diabetes, body mass index, blood pressure, HD parameters (duration, frequency, and adequacy), and medication.
(F,G) The cumulative incidences of HFrEF and HFpEF were compared among patients with increased MMP7 levels.
(H,I) Multivariate linear regression coefficients (β) of candidate variables (left graph) as a function of the decline (Δ) in E/A and LVEF after adjustments for age, sex, smoking habit, past cardiovascular disease events, diabetes, body mass index, blood pressure, HD parameters, and medication. The corresponding coefficient of determination (R2) of each predictive model is shown in a histogram in the right graph.
(J,K) Combining MMP7 and soluble collagen I fragment (sCol-1) levels better predict cardiac dysfunction. Bivariate quadratic surface fitting. The multinomial approximation function is f (x, y) = a + bx + cy + dx2 + ey2, where x and y represent MMP7 and sCol-1, respectively. ΔE/A = (E/A Baseline – E/A Endpoint)×100% / E/A Baseline. ΔLVEF = (LVEF Baseline – LVEF Endpoint)×100% / LVEF Baseline.
Declarations
Declarations of interest: none.
Author contributions: Yang Yang and Lu Ma designed the study; Xinrui Wang and Xiaomeng Li carried out experiments; Dongjuan Zhang analyzed the data; Yang Yang made the figures; Yang Yang drafted the paper; all authors approved the final version of the manuscript.
Funding: The present work was supported by the 13th Five-Year Key Plan for the Military Medical Scientific Research Project to Yang Yang (CBJ14L016).
References
- Kottgen A, Russell SD, Loehr LR, et al. Reduced kidney function as a risk factor for incident heart failure: the Atherosclerosis Risk In Communities (ARIC) study. Journal of the American Society of Nephrology : JASN. 2007; 18: 1307-15.
- Primessnig U, Schönleitner P, Höll A, et al. Novel pathomechanisms of cardiomyocyte dysfunction in a model of heart failure with preserved ejection fraction. European journal of heart failure. 2016; 18: 987-97.
- Winterberg PD, Jiang R, Maxwell JT, Wang B, Wagner MB. Myocardial dysfunction occurs prior to changes in ventricular geometry in mice with Chronic Kidney Disease (CKD). Physiological reports. 2016; 4.
- Paulus WJ, Tschöpe C. A novel paradigm for heart failure with preserved ejection fraction: comorbidities drive myocardial dysfunction and remodeling through coronary microvascular endothelial inflammation. Journal of the American College of Cardiology. 2013; 62: 263-71.
- Yang Y, Ma L, Wang C, et al. Matrix metalloproteinase-7 in platelet-activated macrophages accounts for cardiac remodeling in uremic mice. Basic research in cardiology. 2020; 115: 30.
- Pieske B, Tschöpe C, de Boer RA, et al. How to diagnose heart failure with preserved ejection fraction: the HFA-PEFF diagnostic algorithm: a consensus recommendation from the Heart Failure Association (HFA) of the European Society of Cardiology (ESC). European heart journal. 2019; 40: 3297-317.
- Yang Y, Wang C, Jin L, et al. Effectiveness of and risk associated with aspirin therapy in hemodialysis patients with a background of antiplatelet factor 4/heparin complex antibody detection. Thrombosis research. 2015; 136: 61-8.
- Soslow JH, Xu M, Slaughter JC, et al. The Role of Matrix Metalloproteinases and Tissue Inhibitors of Metalloproteinases in Duchenne Muscular Dystrophy Cardiomyopathy. Journal of cardiac failure. 2019; 25: 259-67.
- Zile MR, Desantis SM, Baicu CF, et al. Plasma biomarkers that reflect determinants of matrix composition identify the presence of left ventricular hypertrophy and diastolic heart failure. Circulation Heart failure. 2011; 4: 246-56.