
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
An atypical presentation of non-specific interstitial pneumonitis
Munazza Asad1*; Samreen Fatima2; Saniya Sabzwari3
1Lecturer, Department of Family Medicine, Aga Khan University, Karachi, Pakistan.
2Resident-IV, Department of Family Medicine, Aga Khan University, Karachi, Pakistan.
*Corresponding Author : Munazza Asad
Lecturer, Department of Family Medicine, Aga Khan University, Karachi, Pakistan.
Email: munazza.asad@aku.edu
Received : Mar 11, 2025
Accepted : Mar 31, 2025
Published : Apr 07, 2025
Archived : www.jcimcr.org
Copyright : © Asad M (2025).
Citation: Asad M, Fatima S, Sabzwari S. An atypical presentation of non-specific interstitial pneumonitis. J Clin Images Med Case Rep. 2025; 6(4): 3542.
Introduction
Epigastric pain can occur from various underlying conditions. Typical diagnoses to consider include peptic ulcer disease, functional dyspepsia, H. pylori gastritis, cholecystitis, and pancreatitis. However, in some cases, the origin of symptoms may be unrelated, e.g. cardiopulmonary issues. It is essential to explore alternative diagnoses if patients do not respond to usual treatments. Here, we describe a case of Non-Specific Interstitial Pneumonia (NSIP) where abdominal pain was the sole presenting symptom, with no accompanying respiratory complaints reported by the patient.
Chest imaging
Her HRCT was reported as patchy abnormal mosaic attenuation areas predominantly involving the bilateral lower lobes, right middle lobe and left lingular segment, along with lower segments of the bilateral upper lobes. These areas were associated with fine fibrotic changes and secondary traction bronchiectasis. Her HRCT can be found in Figure 1.
Background
Non-Specific Interstitial Pneumonia (NSIP) is a form of chronic interstitial pneumonia [1].
Prevalence of NSIP in Asia and LMIC (Lower Middle-Income Countries) is not well documented. The increasing recognition and reporting of ILDs (Interstitial Lung Diseases) in these regions suggest that the prevalence of NSIP may be significant [3,4]. A study conducted among ILD patients in Karachi, Pakistan revealed different sub-types in which IPF was 38% and NSIP was 15% [5]. Another study cited similar rates of NSIP prevalence [6]. NSIP is characterized by interstitial fibrosis, usually involves bilateral lungs with a predisposition for lower lobes [7]. It can be idiopathic; however, it can also be seen in association with HIV, connective tissue diseases and drugs/toxins [8,9]. NSIP, in comparison with other ILDs, has a better prognosis [10]. There is no association with smoking, unlike IPF. It typically has a female predominance and presents in patients aged 40-50 years old, with progressive dyspnea, cough, fever and weight loss, progression of symptoms may be variable [9,11]. Gastrointestinal symptoms are not typically the primary manifestations of Non specific Interstitial Pneumonia (NSIP). However, they can occur, particularly in cases where NSIP is associated with systemic autoimmune or connective tissue diseases. Upper gastro-intestinal symptoms like heartburn, reflux, belching and abdominal or epigastric pain have been reported in several studies [12]. One such study revealed that regurgitation and reflux was present in almost 40% of the patients [13]. Another study concluded high prevalence of gastro esophageal reflux disease which did not respond to standard PPI dose, among patients with ILD [14]. Many studies have reported abdominal pain, dyspepsia, and GERD as common symptoms in patients with ILD [15]. However, gastrointestinal symptoms as the primary presenting complaint are atypical and were not found during literature review on Google Scholar and PubMed. Therefore, our case highlights the importance of keeping other systemic differentials in mind while investigating upper gastrointestinal symptoms that are persistent and non-responsive to standard therapy.
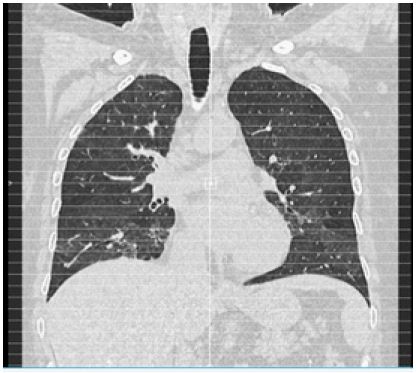
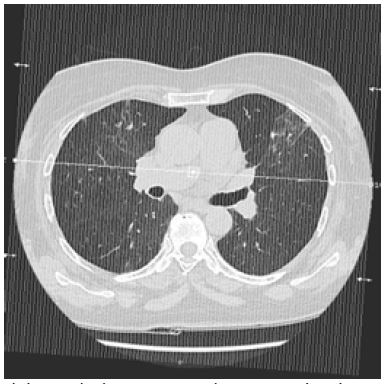
Table 1: American thoracic society classification of interstitial lung disease [2]
| Classification | Types |
|---|---|
| Exposure related | Hypersensitivity pneumonitis, pneumoconiosis |
| CTD*-related | Rheumatoid arthritis, systemic sclerosis, polymyositis, dermatomyositis, systemic lupus erythematosus, mixed connective tissue disease |
| Idiopathic | IPF*, NSIP*, RB-ILD*, DIP*, COP*, AIP* |
| Other | Vasculitis, diffuse alveolar hemorrhage, Langerhans cell histiocytosis, eosinophilic pneumonia, neurofibromatosis, lymphangioleiomyomatosis |
*AIP: Acute Interstitial Pneumonia; *COP: Cryptogenic Organizing Pneumonia; *CTD: Connective Tissue; *DIP: Desquamative Interstitial Pneumonia; *IPF: Idiopathic Pulmonary Fibrosis; *NSIP: Non-Specific Interstitial Pneumonia; *RB-ILD: Respiratory Bronchiolitis associated Interstitial Lung Disease.
Conclusion
Abdominal pain can be a distressing symptom for many patients. When conventional treatments fail to provide relief, it is essential to broaden the differential diagnosis to include potential causes specially related to the lungs and heart. This holistic approach can lead to more accurate diagnoses and effective treatment plans.
Ethical consideration: Informed written consent was taken from the patient. Ethical approval was obtained from Aga khan university hospital with ERC number 2024-10468-32377. For this case report the electronic information was used from database, reviewing the investigations and discharge summaries via mypatient@aku application using patient’s medical record number. Patient’s name and medical record number and all other identifiers were removed to maintain patient’s confidentiality.
References
- Vancheri A SC, Agati S, Poletti V. Interstitial lung abnormalities evolving to histologically proven nonspecific interstitial pneumonia. Rare and Interstitial Lung Diseases: Elsevier. 2025; 33-44.
- Buzan MT, Pop CM. State of the art in the diagnosis and management of interstitial lung disease. Clujul Med. 2015; 88(2): 116-23.
- Anjum H, Ahmad H, Rehman M, Gul H. Prevalence of ild subtypes on the basis of hrct at a tertiary care hospital. PJR. 2020; 29(4).
- Zubairi ABS, Ansarie M, Mahmud T, Ashraf S, Rao NA, et al. National Registry of Interstitial Lung Disease from Pakistan. Cureus. 2021; 13(4): 14684.
- Jafri S, Ahmed N, Saifullah N, Musheer M. Epidemiology and Clinico-radiological features of Interstitial Lung Diseases. Pak J Med Sci. 2020; 36(3): 365-70.
- Sarwar Zubairi AB, Hassan M, Shahzad T, Sarwar S, Abbas A, et al. Spectrum of interstitial lung disease from a tertiary care hospital in Karachi. JPMA The Journal of the Pakistan Medical Association. 2017; 67(7): 1065
- Hino T, Lee KS, Han J, Hata A, Ishigami K, et al. Spectrum of Pulmonary Fibrosis from Interstitial Lung Abnormality to Usual Interstitial Pneumonia: Importance of Identification and Quantification of Traction Bronchiectasis in Patient Management. Korean J Radiol. 2021; 22(5): 811-28.
- Vancheri A, Sorino C, Agati S, Poletti V. Interstitial lung abnormalities evolving to histologically proven nonspecific interstitial pneumonia. Rare and Interstitial Lung Diseases: Elsevier; 2025; 33-44.
- Belloli EA, Beckford R, Hadley R, Flaherty KR. Idiopathic non-specific interstitial pneumonia. Respirology. 2016; 21(2): 259-68.
- Lee J, Kim YH, Kang JY, Jegal Y, Park SY. Korean Guidelines for Diagnosis and Management of Interstitial Lung Diseases: Part 3. Idiopathic Nonspecific Interstitial Pneumonia. Tuberc Respir Dis (Seoul). 2019; 82(4): 277-84.
- Cottin V, Hirani NA, Hotchkin DL, Nambiar AM, Ogura T, et al. Presentation, diagnosis and clinical course of the spectrum of progressive-fibrosing interstitial lung diseases. Eur Respir Rev. 2018; 27(150).
- Ruaro B, Pozzan R, Confalonieri P, Tavano S, Hughes M, et al. Gastroesophageal Reflux Disease in Idiopathic Pulmonary Fibrosis: Viewer or Actor? To Treat or Not to Treat? Pharmaceuticals. 2022; 15(8): 1033.
- Carvajalino S, Reigada C, Johnson MJ, Dzingina M, Bajwah S. Symptom prevalence of patients with fibrotic interstitial lung disease: A systematic literature review. BMC Pulm Med. 2018; 18(1): 78.
- Raghu G, Freudenberger TD, Yang S, Curtis JR, Spada C, et al. High prevalence of abnormal acid gastro-oesophageal reflux in idiopathic pulmonary fibrosis. Eur Respir J. 2006; 27(1): 136-42.
- Allaix ME, Fisichella PM, Noth I, Mendez BM, Patti MG. The pulmonary side of reflux disease: From heartburn to lung fibrosis. J Gastrointest Surg. 2013; 17(8): 1526-35.