
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 6
Is silver sufficient? An infectious organism presenting as an abdominal mass
Aneal S Dayal1*; John J Farrell2
1College of Medicine, University of Illinois Peoria, One Illini Drive, Peoria, IL 61605, USA.
2Department of Microbiology, St Francis Medical Center, 1224 N Berkeley Ave, Peoria, IL 61603, USA.
*Corresponding Author : Aneal S Dayal
College of Medicine, University of Illinois Peoria, One Illini Drive, Peoria, IL 61605, USA.
Tel: 630 881 1768;
Email: adayal4@uic.edu
Received : Mar 10, 2025
Accepted : Apr 01, 2025
Published : Apr 08, 2025
Archived : www.jcimcr.org
Copyright : © Dayal AS (2025).
Citation: Dayal AS, Farrell JJ. Is silver sufficient? An infectious organism presenting as an abdominal mass. J Clin Images Med Case Rep. 2025; 6(4): 3543.
Description
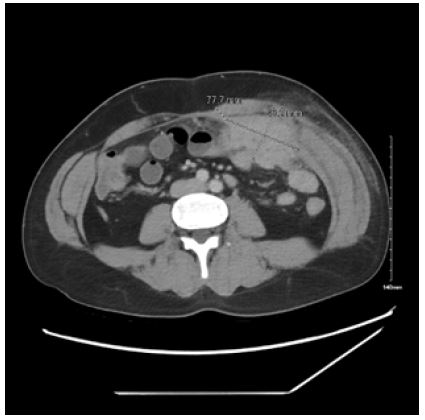
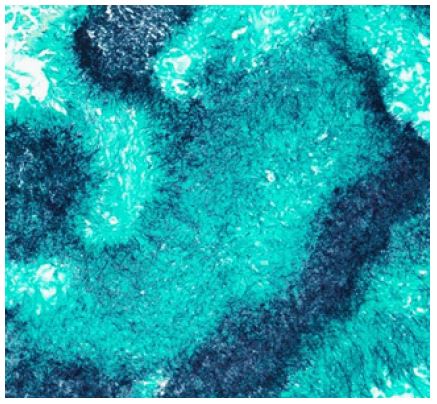
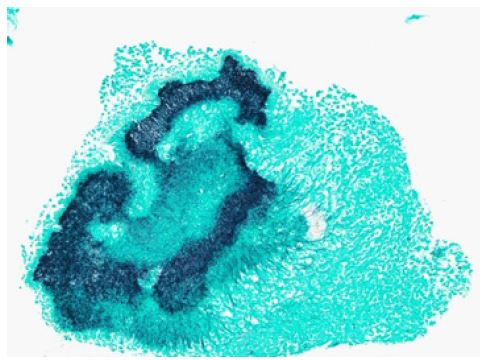
A 37-year-old man presented with complaints of increasing abdominal pain for six months accompanied by chills, nausea, constipation, and an unintended 15-pound weight loss. He was hemodynamically stable with labs only significant for a hemoglobin of 10.4 g/dL and chromogranin A of 118 ng/milk computed tomography of the abdomen and pelvis revealed a hyperdense mass measuring 4.6 x 7.8 x 6.1 centimeters surrounding a lobule of fat in the left anterior momentum of the peritoneum abutting the anterior abdominal wall. Portions of this hyperdense material infiltrated into the abdominal wall musculature with associated soft tissue stranding and distal transverse colonic and left upper abdominal small bowel wall thickening (Figure 1). Percutaneous ultrasound guided core biopsy revealed severe acute and chronic inflammation with necrosis and filamentous branching bacterial organisms consistent with Actinomyces spp. on silver stain (Figures 2 and 3).
Discussion
Abdominal actinomycosis is very rare and represents a challenge in diagnosis as it is often misinterpreted as a malignancy on initial presentation [1]. Involvement of the gastrointestinal tract represents a smaller proportion of actinomycosis cases [1,2]. Despite its rarity, abdominal actinomycosis should be considered in the differential diagnosis when patients present with abdominal pain and associated mass that penetrates through tissue planes.
Declarations
Conflict of interest/competing interests: The authors of this article do not have any conflict of interest with the publication of this manuscript or any institution or product mentioned in this manuscript and/or is essential to the outcome of the study presented. The authors also do not have any conflict of interest with products that compete with those mentioned in this manuscript.
None of the authors had any financial relationship within the last three years with a biotechnology manufacturer, a pharmaceutical company, or other commercial entity that has any interest in the subject matter, materials, or process (es) discussed in the manuscript.
Statements from authors: The manuscript has been read and approved by all the authors, and the requirements for authorship have been met. Each author believes that the manuscript represents honest work.
This study does not contain identifying information about the patients. Informed consent was obtained from the patient for case publication.
References
- Garner JP, Macdonald M, Kumar PK. Abdominal actinomycosis. International Journal of Surgery. 2007; 5(6): 441-448. doi:https://doi.org/10.1016/j.ijsu.2006.06.009
- Vasilescu AM, Târcoveanu E, Lupascu C, Blaj M, Lupascu Ursulescu C, Bradea C. Abdominopelvic Actinomycosis—The Diagnostic and Therapeutic Challenge of the Most Misdiagnosed Disease. Life. 2022; 12(3): 447. doi:https://doi.org/10.3390/life12030447