
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Unusual presentation of acute appendicitis
Rozan Marjiyeh-Awwad1,2*
1Rambam Health Care Campus, Haifa, Israel.
2University Hospital Düsseldorf, Düsseldorf, Germany.
*Corresponding Author : Rozan Marjiyeh-Awwad
Rambam Health Care Campus, Haifa, Israel.
Email: r_marjiyeh@rambam.health.gov.il
Received : Mar 13, 2025
Accepted : Apr 03, 2025
Published : Apr 10, 2025
Archived : www.jcimcr.org
Copyright : © Marjiyeh-Awwad R (2025).
Citation: Marjiyeh-Awwad R. Unusual presentation of acute appendicitis. J Clin Images Med Case Rep. 2025; 6(4): 3547.
Introduction
As a surgeon, we all believe that nowadays acute appendicitis is the most common and frequent surgical diagnosis during a surgical shift in the ER. Some patients present with sudden pain appearance, others with a nausea, vomiting and wandering pain. Some but present after suffering few days without paying attention for developing an acute abdomen presenting with peri appendicular abscess or even free intraperitoneal perforation of the appendix. Patients with unusual presentation, or atypical symptoms need a high level of suspicion for the diagnosis. Even after years of diagnosing and treating patients with acute appendicitis, the atypical presentation leads to misdiagnosing or even unsuitable intervention. Recognizing such cases and being aware of the unusual presentation can bring in benefits of rapid diagnosing and ensures better outcomes. Recurrent cases were published that described unusual presentation of appendicitis, some discussed incarcerated femoral hernia included appendicitis [1], others described tuberculosis of appendix as first diagnosis for tuberculosis in young patient [2] which appears only in 0.1%-2% of appendectomies. In the cases where appendicitis leads to soft tissue infection which fistulated through the posterior abdominal wall it caused a conflict by unusual presentation with differential diagnosis of necrotizing fasciitis. For another example, appendicitis can present as soft tissue infection of the abdominal wall, flank, thigh and perineum, the most serious complication of which being necrotizing fasciitis [4]. In these complicated cases the cost the patient paid due to late diagnosis and intervention could be such high as from long term VAC-use until reoperation debridement and even ileostomy as it will be shown in our case presentation. In some reports a case of unexpected perforation due to foreign body was described [5]. even typically presented appendicitis may be complicated and misdiagnosed by reactive arthritis [6]. Herein we report a case of a young patient with mental retardation, which in our opinion was one of the factors that lead to unusual presentation of her illness, in this case with medical background of mental retardation and groin pain, leads to first diagnosis of groin abscess, which was treated operatively but partially, incomplete treatment lead to septic shock and emergent laparotomy, showing multiple intraabdominal pus collections due to perforated appendix without intraperitoneal free air.
Case history
Investigation: We present a 31-year- old female, presented to the ER due to mass and pain in her right groin. Her medical history describes a mental retardation, clinically dysmorphic.
In the ER she was stable hemodynamically, with tachycardia up to 120 b/m. In her physical examination a mass was palpable in the inguinal ligament which extends to her right flank, it had a Fluctuation and induration with noticeable local tenderness. She denied abdominal pain, nausea, vomiting or any other gastrointestinal symptoms. No fever, no chills. No abdominal trauma history.
Labor tests show completed blood account with increased white blood cells of 31,000x103/μL, Blood Chemistry with creatinine of 1.09 gr/dL, hyponatremia 122 mmol/L:
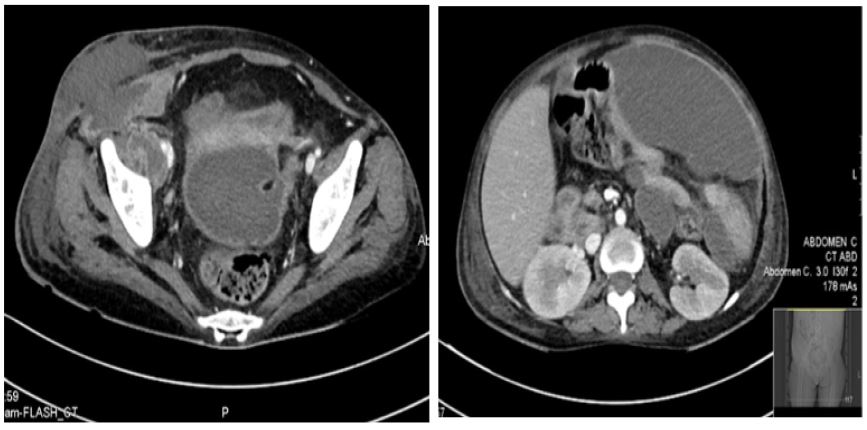
Diagnosis: Due to the mentioned parameters a CT scan was performed to rule out necrotizing fasciitis.
It showed multiple intraabdominal fluid collection. Measured as simple fluid (Figure 1). Multiple pockets of liquid in the Peritoneal space, the largest one is seen in the upper abdomen and partially scanned, measured about 16 x 6.5 cm. Additional pockets attached to the small intestine, anterior rectum, anterior of the right iliac bone and adjacent to the neck. The pockets contain a simple fluid (Figures 2 and 3). It seems that most of them are connected to each other. In the pelvis on the right is another liquid pocket that is adjacent to the abdominal wall that breaks it and continues into the subcutaneous skin, in this position the liquid is measured as a composite liquid, around which the turbidity of fat and subcutaneous edema.
This structure is suitable for an infectious process. There is no obvious exception to the subcutaneous fluid. the appendix could not be clearly identified.
Initial treatment: We drained initially a Large abscess up to 8 x 10 cm in lower right abdomen, which spread in depth to the muscles of the abdominal wall and sides toward the pelvis in parallel to the upper in the right abdomen, about 5 cm from a middle-axillary line, a height of the upper border, a mid-axillar line and an inguinal canal at a lower boundary, without the involvement of an inguinal canal, cellulite around. Necrotic skin tissue was removed, about 250 ml of pus was suctioned. A massive drainage of the wound was performed and antibiotic treatment was continued.
Postoperative care: In the first three postoperative day – she was stable but tachycardic until 113 b/p; without fever. In the 4th postoperative day, she became dyspneic; with desaturation in room air, oxygen was supplied. Labor: White blood cell counts of 28x103/μL HB 8.8 (after one packed cell due to Hemoglobin levels of 6.7 gr/dL) hyponatremia 122 creatinine 1.09. In the next day-abdominal distension, clinical impression of elevated intraabdominal pressure. We completed an abdominal CT scan: Intraabdominal Fluid collection with no noticeable difference, the largest one in the left upper quadrant.
Due to the sac-like fluid collection in the absence of abdominal symptoms, a differential diagnosis included Pseudomyxoma peritonei, with absence of abdominal symptoms and after a multidisciplinary team discussion we decided to drain on easily accessible fluid collection. Simultaneously with respiratory deterioration, we performed a US-guided punctation of the fluid – pus with offensive smell. See picture below. She was transformed directly to operating room for exploratory laparotomy. In the operation a huge amount-about 3-4 liters of pus was suctioned by entering the intraperitoneal space. Till end the operation approximately 5 liter of pus in the different fluid pockets.in addition we perform an appendectomy due to edematous gangrenous appendix. One single enterotomy was repaired primary. She was admitted to the ICU. Few days after the last surgery, a second investigative laparotomy was performed for a second look - during which no further foci of infection appeared, the bowel still appeared to be edemas, intraperitoneal lavage was performed, the appendectomy was examined without leakage marks, the small and large bowel looks viable and healthyAbdomen was closed with vicarly mesh. About three days later, due to worsening of sepsis, an abdominal CT scan was done: a suspicion of leakage from terminal ileum. Therefore, a recurring laparotomy was decided during which it appeared to have leaked from the enterotomy area - because the bowel looked quite ill and edemas, a resection of a small bowel sectio, ileostomy was performed with mucus fistula of the ascending colon.
Ten days later a high amount of bile seen through the Jackson pratt. We decided to take her again to the operating room. In order to find out the leakage source we inject blue contrast through the ileostomy, it was extravasated through the proximal part of the ileostomy. We performed a new ileostomy, and closed the abdomen after intraperitoneal lavage.
Discharge: Through the next two months in the ICU, she was extubated and transferred to rehabilitation center. One year later she admitted electively and underwent successfully an ileostomy closure.
Pathology: Appendix with severe peritonitis and area of phlegmonous transmural inflammation. Other resection small bowel part was unremarkable.


Discussion
Acute appendicitis is seen nowadays as a typical surgical emergency. The medical development has succeeded in reducing hospitalization- and treatment time due to faster diagnosing and relatively easy interventional treatment. But yet it constitutes one of the most challenging diagnoses specially in patient with communication disability. The presented case shows the range of differential diagnosis specially when the patient presents with unusual symptoms even if an acceptable imaging was performed. The atypical presentation of acute appendicitis varieties depends on the unusual morphological characters, whereas some cases showed unusual anatomical presentation, which lead to missing the diagnoses, while other presents with unusual symptoms development, leasing in some cases to larger differential diagnosis and requires a good clinical and radiological judgement before intervention to prevent exacerbation or worsening of the current status. In our case presentation the challenge was at first understanding the clinical symptoms of the patient to match it to an acute surgical problem or a longstanding oncological status. The challenge was in interpretation of the imaging in relation to the clinical presentation in a communication disabled patient, making the imaging looks relative more suitable to the development of oncological disease, while the patient underwent a “silent sepsis” until sudden respiratory and cardiogenic failure occur. Our message in this case is to show the difficulties a surgeon can confront when anamneses lacks and to deliver the summary of the importance of completion of radiological clearance but not on cost of acute deterioration of the patient. On the other hand, we should know that even the simplest surgical condition can present in such a complicated form that experienced surgeon could have difficulties in recognizing the given condition.
References
- Akopian G, Alexander M. De Garengeot Hernia: Appendicitis within a Femoral Hernia. 2005; 71(6): 526-527.
- Constantinescu C, Vayalumkal J, Fisher D. An unusual case of appendicitis. CMAJ. 2014; 186(16): 1241-1243. doi: 10.1503/cmaj.131126
- J Bryan, J Ashcroft, VE Hudson, KY Wong. Unusual presentation of appendicitis as soft tissue infection of the thigh. Journal of Surgical Case Reports. 2021; 1: rjaa505.
- Kumar D, Cortés-Penfield NW, El-Haddad H, Musher DM. Bowel perforation resulting in necrotizing soft-tissue infection of the abdomen, flank, and lower extremities. Surg Infect (Larchmt) 2018; 19: 467-72.
- Tustumi F. Unusual cause of appendicitis. A case report of acute appendicitis caused by needle ingestion. Int J Surg Case Rep. 2020; 72: 499-502.
- Mackie SL, Keat A. An unusual complication of appendicitis. Annals of the Rheumatic Diseases. 2004; 63: 1526.