
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Successful multimodal management of pediatric chest wall Ewing’s sarcoma: A case report and comprehensive review of treatment strategies
Gurpreet Kaur Chawla1; Vishakha Maheshwari2; Vaibhav Sharma2*
1Department of Internal Medicine, Himalayan Institute of Medical Sciences, Dehradun, India.
2Center for Advanced Heart Failure and Heart Transplant, University of Texas Health Science Center, Houston, USA.
*Corresponding Author : Vaibhav Sharma
Center for Advanced Heart Failure and Heart Transplant, University of Texas Health Science Center, Houston, USA.
Tel no: +13142160550;
Email: vsharma3090@gmail.com
Received : Mar 13, 2025
Accepted : Apr 03, 2025
Published : Apr 10, 2025
Archived : www.jcimcr.org
Copyright : © Vaibhav S (2025).
Abstract
Ewing’s sarcoma is a very virulent malignant neoplasm composed of round cells with a high frequency in pediatric and young adult age groups. The present article elucidates a case report of a 12-year-old female patient with Ewing’s sarcoma of the chest wall, presenting the clinical presentation, diagnostic workup, radiographic features, and a detailed review of literature regarding management practices and prognostic factors of this uncommon malignancy. Chest wall involvement is fraught with serious diagnostic and therapeutic difficulties owing to the complicated anatomical structures and the need for a multidisciplinary therapeutic approach. Early diagnosis and appropriate therapeutic measures are important for the enhancement of prognosis in the case of this virulent tumor.
Citation: Chawla GK, Maheshwari V, Vaibhav S. Successful multimodal management of pediatric chest wall ewing’s sarcoma: A case report and comprehensive review of treatment strategies. J Clin Images Med Case Rep. 2025; 6(4): 3548.
Introduction
Ewing’s sarcoma is classified in a category of neoplasms called the Ewing’s Sarcoma Family of Tumors (ESFT), which comprises classic Ewing’s sarcoma, Peripheral Primitive Neuroectodermal Tumor (PPNET), and Askin tumor. These neoplasms are defined by the presence of small round blue cells and cytogenetic abnormalities [1,2], namely the t(11;22) (q24; q12) translocation that leads to the formation of the EWS-FLI1 fusion gene in approximately 85% of cases [3]. Ewing’s sarcoma is most commonly seen in pediatric age groups and young adults, with the highest incidence in 10- to 20-year-old patients. The condition accounts for approximately 3% of all malignancies in children [4]. The most common anatomical sites involved are the pelvis, femur, and rib cage [5]. Ewing’s sarcoma in the chest wall, also known as Askin tumor when it is in the thoracopulmonary area, is a condition with unique challenges due to its location and its aggressive nature [6].
Case presentation
A 12-year-old female patient presented with a three-month history of progressive swelling on the right chest. She complained of no chest pain, cough, or shortness of breath. On examination, the swelling was clear in shape, on the lower right side of her chest, and firm in consistency.
Diagnostic imaging
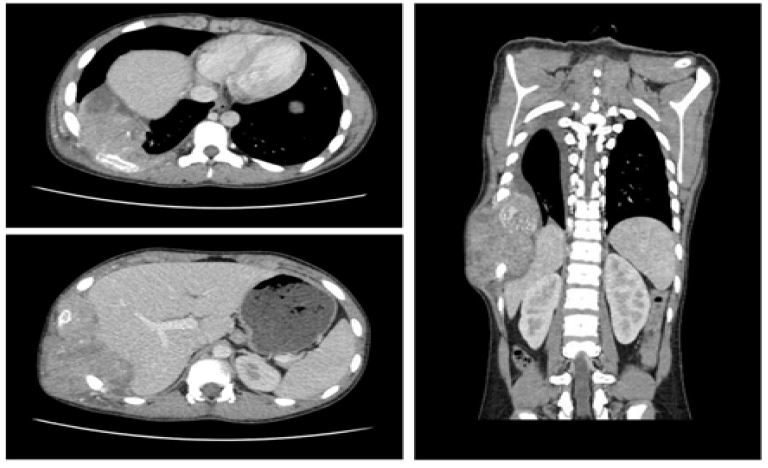
There was a poorly defined margin with lytic bone lesions on initial chest radiograph involving the lateral border of the right 9th rib with a corresponding soft tissue lesion. The remainder of the radiograph was otherwise within normal limits (Figure 1). Contrast-enhanced chest CT showed a large, ill-defined heterogeneously enhancing lytic mass filling the right hemithorax with peripheral necrosis measuring about 12 × 9 × 5 cm (craniocaudal by anteroposterior by transverse). Hypodense regions indicative of necrosis was noted within the lesion, which extended to the right lateral chest wall with cortical erosion and destruction of the right 9th rib. The lesion was invading into the lateral chest wall muscles and subcutaneous tissue. It was also found to be pushing the left hemidiaphragm downwards with scalloping of the liver surface. While focally ill-defined fat planes were observed, there was no hepatic invasion. The lesion invaded the parietal and visceral pleura as well (Figure 2a-2c). On the basis of the history, physical, and imaging results, the patient was hospitalized and a Positron Emission Tomography (PET) scan was performed. It revealed a large soft tissue mass occupying the right hemithorax and extending into the lateral chest wall and the overlying ribs, consistent with Ewing sarcoma. No other FDG-avid disease was present elsewhere in the body, suggesting localized disease [7,8].
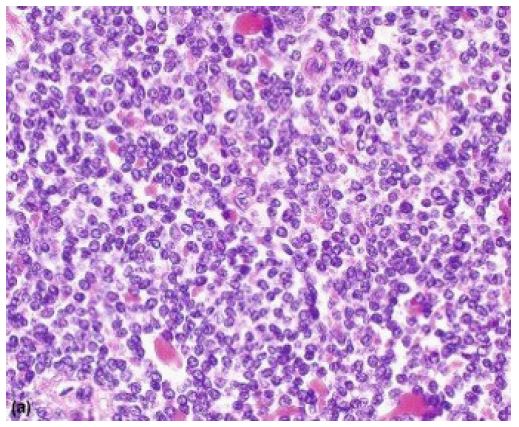
Histopathological diagnosis: A CT-guided biopsy was performed under sedation, and five fragments of soft tissue measuring in aggregate 0.7 × 0.5 × 0.2 cm were submitted for histopathological examination. Microscopic analysis revealed sheets of small round blue cells with high nuclear-to-cytoplasmic ratio, fine chromatin, and inconspicuous nucleoli (Figure 3). Immunohistochemistry demonstrated positive staining for synaptophysin, CD99 (MIC2), and FLI-1. The PAS and PASD stains highlighted the cytoplasmic glycogen [12,13]. CKAE1/3, chromogranin, desmin, S100, MYOD1, Myogenin, CD45, and TdT were all negative. These findings were consistent with Ewing sarcoma.
Molecular analysis of the tumor tissue was positive for t(11;22) (q24; q12) EWS/FLI-1/ERG fusion transcript, confirming the diagnosis of Ewing sarcoma of the chest wall with localized disease [9].
Management: A multidisciplinary approach involving pediatric oncologists, radiation oncologists, thoracic surgeons, and an orthopedic surgeon was adopted. Initially, the patient was scheduled for bilateral bone marrow aspirate and biopsy, along with the placement of a central line (Polykite). However, these procedures could not be performed because of complications related to anesthesia. Instead, central venous access was achieved using a Peripherally Inserted Central Catheter (PICC) to allow for chemotherapy administration after obtaining a baseline echocardiogram.
Systemic therapy: The patient began induction chemotherapy as the first step in treatment, with the goal of managing micro metastatic disease and shrinking the tumor before local therapy. An interval-compressed regimen that alternated Vincristine-Doxorubicin-Cyclophosphamide (VDC) with Isocyanide-Etoposide (IE) was given at 2-week intervals for a total of 6 cycles. A follow-up CT scan of the chest, performed after the second cycle of chemotherapy, revealed a significant reduction (about 50%) in the size of the enhancing pleural mass in the right hemithorax, with the mass effect on the nearby cardio mediastinal structures resolved. The mass, which previously measured 12 × 9 × 5 cm (CC×AP×TR), decreased to 6 × 5.4 × 3.1 cm in its maximum dimensions, indicating a favorable response to systemic therapy.
Surgical intervention: After completing six cycles of induction chemotherapy, local control was achieved through surgical resection. The surgery involved removing part of the 10th rib and performing a wedge resection of the right lower lobe. During the procedure, two previously undetected pulmonary nodules in the right middle lobe were also found and excised. A segmental lung resection was carried out on the adhered right lower lobe, along with a pleurectomy performed en bloc with the entire specimen. The surgery went smoothly without any complications, and histopathological analysis confirmed negative margins (R0 resection) [10].
Radiation therapy: Even though an R0 resection was achieved along with a complete pathological response, adjuvant radiotherapy was advised because of the initially large tumor size, the suspected pleural involvement that had not been sampled, and the location of the primary tumor on the chest wall. Radiation therapy was initiated two weeks post-surgery after ensuring proper healing of the chest wall incision. The radiation treatment plan included whole lung irradiation with a total of 15 Gy given in 10 fractions, followed by a boost to the surgical bed, bringing the total dose to 33 Gy at 1.8 Gy per fraction.
Adjuvant chemotherapy: Following recovery from surgery and completion of radiation therapy, the patient continued with the planned chemotherapy regimen for a total of 43 weeks (14 cycles of chemotherapy).
Outcome and follow-up: The CT chest and PET scan performed at the end of treatment confirmed complete remission. At the time of this report, the patient had maintained remission for more than one year without evidence of relapse. The patient continues to be regularly followed with imaging evaluations every 3 months.

Discussion
Ewing’s sarcoma of the chest wall represents a rare and challenging clinical entity that requires prompt diagnosis and a multidisciplinary approach to management.
Our case illustrates several important aspects of this disease, including:
Clinical presentation and diagnosis: The clinical presentation of chest wall Ewing’s sarcoma often lacks specificity, with the most common symptoms being localized pain, swelling, and occasionally respiratory, symptoms depending on the extent of intrathoracic involvement. Our patient presented a progressively enlarging mass on the chest wall without any accompanying symptoms, which underscores the need to consider malignancy when evaluating chest wall masses in children, even when there are no general symptoms present [11,12]. The diagnostic approach to suspected chest wall Ewing’s sarcoma typically involves a combination of imaging studies and histopathological examination. Initial radiographic assessments usually show lytic bone lesions along with soft tissue masses. CT and MRI scans offer detailed insights into the local extent of the disease [13], while PET-CT is useful for identifying distant metastases and evaluating treatment response [13]. A histopathological diagnosis is made through biopsy, where the hallmark finding is the presence of small round blue cells. Immunohistochemical markers, especially CD99 and FLI-1, assist in differentiating Ewing’s sarcoma from other small round blue cell tumors. Molecular confirmation of the EWS-FLI1 fusion gene or other EWSR1 rearrangements is essential for a definitive diagnosis [13-15].
Therapeutic approach: The management of Ewing’s sarcoma involves a multidisciplinary approach involving systemic chemotherapy, local control measures (surgery and/or radiation therapy), and in some cases, high-dose chemotherapy with stem cell rescue [14].
Systemic therapy: Systemic chemotherapy is essential in treating Ewing’s sarcoma, targeting both visible tumors and possible micrometastases. The standard treatment regimens usually consist of a mix of vincristine, doxorubicin, cyclophosphamide, ifosfamide, and etoposide. The interval-compressed VDC/IE regimen utilized for our patient has demonstrated better outcomes than the traditional 3-week intervals in multiple studies [16]. The response to induction chemotherapy offers valuable prognostic insights and informs decisions regarding subsequent local therapies [16]. Our patient showed a notable decrease in tumor size after only two cycles, suggesting that the tumor is sensitive to chemotherapy.
Local control: Local control of chest wall Ewing’s sarcoma can be accomplished through surgery, radiation therapy, or a combination of both. The choice of the best approach is influenced by several factors, such as the tumor’s location and size, the response to induction chemotherapy, the possibility of obtaining negative margins, and the expected functional and cosmetic results [17]. Surgical resection with negative margins is associated with improved local control rates and is preferred when feasible [17,18]. Our patient underwent successful resection of the primary tumor and involved structures with negative margins, which is a favorable prognostic factor.
Radiation therapy: Radiation therapy plays a crucial role in managing local control for Ewing’s sarcoma, especially in situations where there are positive or close margins, inadequate response to induction chemotherapy, or when surgical intervention could lead to considerable functional or cosmetic issues [19]. In our case, even though we achieved negative margins, radiation therapy was given because of the tumor’s initial large size and its location, aligning with current guidelines for high-risk characteristics.
Prognostic factors and outcomes: Several prognostic factors have been identified in Ewing’s sarcoma, such as tumor size and location, the presence of metastatic disease at diagnosis, the response to induction chemotherapy, and the achievement of local control [20]. In our patient, favorable prognostic factors included localized disease, a strong response to induction chemotherapy, and complete surgical resection with negative margins.
The overall 5-year survival rate for localized Ewing’s sarcoma has seen significant improvement over the years, with current estimates between 65% and 75% [13]. However, patients diagnosed with metastatic disease still face challenging outcomes, with 5-year survival rates around 20-30% [5].
Conclusion
This case highlights the effective multidisciplinary approach taken to manage a pediatric patient with chest wall Ewing’s sarcoma, leading to a complete response and lasting remission. Early diagnosis, timely initiation of multimodal therapy, and diligent monitoring are crucial for achieving the best outcomes in this aggressive malignancy [5]. Managing chest wall Ewing’s sarcoma requires a customized strategy that considers the specific anatomical challenges and the necessity for effective local control while reducing long-term complications. Ongoing advancements in molecular diagnostics, targeted therapies, and improvements in local control methods are anticipated to enhance outcomes for patients facing this challenging disease.
Declarations
Funding: The authors received no funding for this article.
Conflict of interest statement: The authors declare no conflicts of interest relevant to this article.
Fundings: Nil.
Disclosures: Nil.
References
- Khoury JD. Ewing sarcoma family of tumors. Advances in anatomic pathology. 2005; 12(4): 212-20.
- Maheshwari AV, Cheng EY. Ewing sarcoma family of tumors. JAAOS-Journal of the American Academy of Orthopaedic Surgeons. 2010; 18(2): 94-107.
- Giovannini M, Biegel JA, Serra M, Wang JY, Wei YH, et al. EWS-erg and EWS-Fli1 fusion transcripts in Ewing’s sarcoma and primitive neuroectodermal tumors with variant translocations. The Journal of clinical investigation. 1994; 94(2): 489-96.
- Larsson SE, Lorentzon R. The incidence of malignant primary bone tumours in relation to age, sex and site: A study of osteogenic sarcoma, chondrosarcoma and Ewing’s sarcoma diagnosed in Sweden from 1958 to 1968. The Journal of Bone & Joint Surgery British Volume. 1974; 56(3): 534-40.
- Grünewald TG, Cidre-Aranaz F, Surdez D, Tomazou EM, de Álava E, et al. Ewing sarcoma. Nature reviews Disease primers. 2018; 4(1): 5.
- Christiansen S, Semik M, Dockhorn-Dworniczak B, Rötker J, Thomas M, et al. Diagnosis, treatment and outcome of patients with Askin-tumors. The Thoracic and Cardiovascular Surgeon. 2000; 48(05): 311-5.
- Eubank WB, Mankoff DA, Schmiedl UP, Winter 3rd TC, Fisher ER, et al. Imaging of oncologic patients: benefit of combined CT and FDG PET in the diagnosis of malignancy. AJR. American journal of roentgenology. 1998; 171(4): 1103-10.
- Agress Jr H, Cooper BZ. Detection of clinically unexpected malignant and premalignant tumors with whole-body FDG PET: histopathologic comparison. Radiology. 2004; 230(2): 417-22.
- Urano F, Umezawa A, Yabe H, Hong W, Yoshida K, et al. Molecular analysis of Ewing’s sarcoma: another fusion gene, EWS‐E1AF, available for diagnosis. Japanese journal of cancer research. 1998; 89(7): 703-11.
- Pan HY, Morani A, Wang WL, Hess KR, Paulino AC, et al. Prognostic factors and patterns of relapse in Ewing sarcoma patients treated with chemotherapy and r0 resection. International Journal of Radiation Oncology* Biology* Physics. 2015; 92(2): 349-57.
- Widhe B, Widhe T. Initial symptoms and clinical features in osteosarcoma and Ewing sarcoma. JBJS. 2000; 82(5): 667.
- Balamuth NJ, Womer RB. Ewing’s sarcoma. The lancet oncology. 2010; 11(2): 184-92.
- Iwamoto Y. Diagnosis and treatment of Ewing’s sarcoma. Japanese journal of clinical oncology. 2007; 37(2): 79-89.
- Zöllner SK, Amatruda JF, Bauer S, Collaud S, de Álava E, et al. Ewing sarcoma-diagnosis, treatment, clinical challenges and future perspectives. Journal of clinical medicine. 2021; 10(8): 1685.
- Hu-Lieskovan S, Zhang J, Wu L, Shimada H, Schofield DE, et al. EWS-FLI1 fusion protein up-regulates critical genes in neural crest development and is responsible for the observed phenotype of Ewing’s family of tumors. Cancer research. 2005; 65(11): 4633-44.
- Pretz JL, Barysauskas CM, George S, Hornick JL, Raut CP, et al. Localized adult Ewing sarcoma: Favorable outcomes with alternating vincristine, doxorubicin, cyclophosphamide, and ifosfamide, etoposide (VDC/IE) based multimodality therapy. The Oncologist. 2017; 22(10): 1265-70.
- Bedetti B, Wiebe K, Ranft A, Aebert H, Schmidt J, et al. Local control in Ewing sarcoma of the chest wall: results of the EURO-EWING 99 trial. Annals of surgical oncology. 2015; 22: 2853-9.
- Shamberger RC, LaQuaglia MP, Gebhardt MC, Neff JR, Tarbell NJ, et al. Ewing sarcoma/primitive neuroectodermal tumor of the chest wall: impact of initial versus delayed resection on tumor margins, survival, and use of radiation therapy. Annals of surgery. 2003; 238(4): 563-8.
- Donaldson SS, Torrey M, Link MP, Glicksman A, Gilula L, et al. A multidisciplinary study investigating radiotherapy in Ewing’s sarcoma: End results of POG# 8346. International Journal of Radiation Oncology* Biology* Physics. 1998; 42(1): 125-35.
- Lee J, Hoang BH, Ziogas A, Zell JA. Analysis of prognostic factors in Ewing sarcoma using a population‐based cancer registry. Cancer. 2010; 116(8): 1964-73.