
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Cerebral radionecrosis in brain tumors: Dexamethasone vs. Bevacizumab: A case report
Dos Santos AAA¹; Da Silva L1; Da Silva M1; Araujo B1; Kojima T1; Santos D1; Martini C²; Delcole G²; Ribeiro I²; Rotta R³*
1Undergraduate Student of Biomedical Sciences, FMU – Metropolitan University, São Paulo, Brazil.
2Neurosurgery Resident, Santa Paula Hospital/DASA, São Paulo, Brazil.
3Head of Neurosurgery Residency Program, Santa Paula Hospital/DASA, São Paulo, Brazil.
*Corresponding Author : Medeiros Roger Thomaz Rotta
Head of Neurosurgery Residency Program, Santa Paula Hospital/DASA, São Paulo, Brazil.
Email: roger.rotta@hotmail.com
Received : Mar 15, 2025
Accepted : Apr 04, 2025
Published : Apr 11, 2025
Archived : www.jcimcr.org
Copyright : © Rotta R (2025).
Abstract
Radionecrosis is a frequent and severe complication of radiotherapy in brain tumors, often mimicking disease progression on imaging. Advanced magnetic resonance techniques such as spectroscopy and perfusion imaging can assist in distinguishing true progression from pseudoprogression. Standard treatment includes corticosteroids, although adverse effects from prolonged use are common. Surgical intervention may be required in severe cases. Recently, bevacizumab has emerged as a promising alternative, offering radiological improvement with fewer side effects. Nevertheless, clinical benefits remain inconsistent, underlining the need for comparative meta-analyses to guide therapeutic decision-making.
Citation: Dos Santos AAA, Da Silva L, Da Silva M, Araujo B, Rotta R, et al. Cerebral radionecrosis in brain tumors: Dexamethasone vs. Bevacizumab: A case report. J Clin Images Med Case Rep. 2025; 6(4): 3550
Introduction
Cerebral radionecrosis (RN) is a late-onset and potentially debilitating consequence of radiation therapy, particularly in patients with high-grade gliomas and cerebral metastases. As Mangesius et al. (2022) emphasize, differentiating RN from tumor progression remains a key clinical challenge, given the similarity in radiological features [1]. Conventional MRI often lacks sufficient specificity, resulting in potential misdiagnosis and inappropriate management strategies.Radiation doses between 46-50 Gy are effective in low-grade gliomas, while 60 Gy remains the standard for high-grade gliomas. Notably, radionecrosis may develop even below these thresholds, reinforcing the importance of identifying risk factors such as total dose, fraction size, and treatment duration. Chemotherapy has also been associated with increased RN risk, even when adjusted for biological effective dose.
Accurate distinction between recurrence and radionecrosis is critical. Raimbault et al. (2014) emphasize the implications for patient prognosis and therapy [2]. Diagnosis is particularly complex in MRI findings post-therapy, where new contrast-enhancing lesions require meticulous differential assessment.Multimodal imaging—combining diffusion, perfusion, and MR spectroscopy—provides superior diagnostic accuracy. Spectroscopy, in particular, allows metabolic characterization of lesions, distinguishing necrotic tissue from active tumor. However, despite encouraging results, standardized protocols are lacking, and further longitudinal studies are required.Treatment typically includes corticosteroids and, in severe cases, surgical resection. More recently, agents like bevacizumab and hyperbaric oxygen therapy have been considered. Bevacizumab, an anti-VEGF monoclonal antibody, has demonstrated radiologic efficacy and reduced cerebral edema, as observed in our case with disease control for over two years post-surgery.
Case report
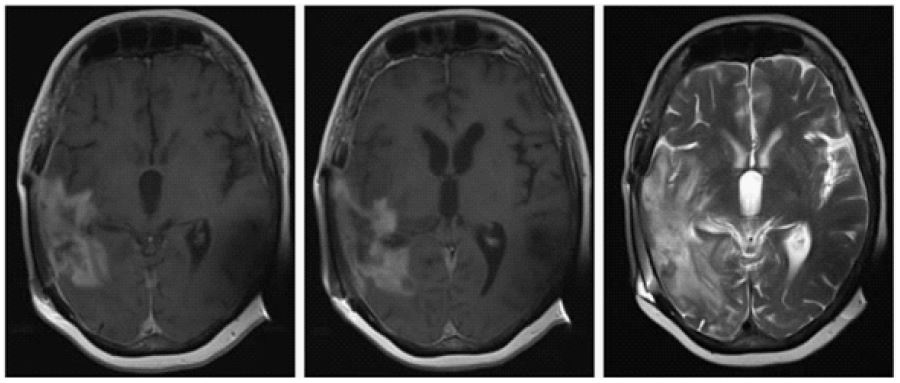
A 56-year-old female presented with behavioral changes and facial paresis on December 29, 2022. CT scan revealed a mass lesion with midline shift and hemorrhage, suggestive of high-grade glioma. Nodular lesions in the left lateral ventricle were noted. She underwent gross total resection in January 2023 of a 4.9 cm malignant neoplasm located in the right angular and supramarginal gyri, extending into the opercular cortex. Adjuvant treatment included 60 Gy radiotherapy over 30 fractions plus temozolomide, completed in April 2023. Maintenance temozolomide began in May but was suspended in October due to suspected progression. A second resection in October 2023 revealed viable tumor (20%) and extensive treatment-induced changes, including radionecrosis (80%). Postoperatively, the patient developed CSF leakage, infection, and required ventriculoperitoneal shunting (Figure 1).

Discussion
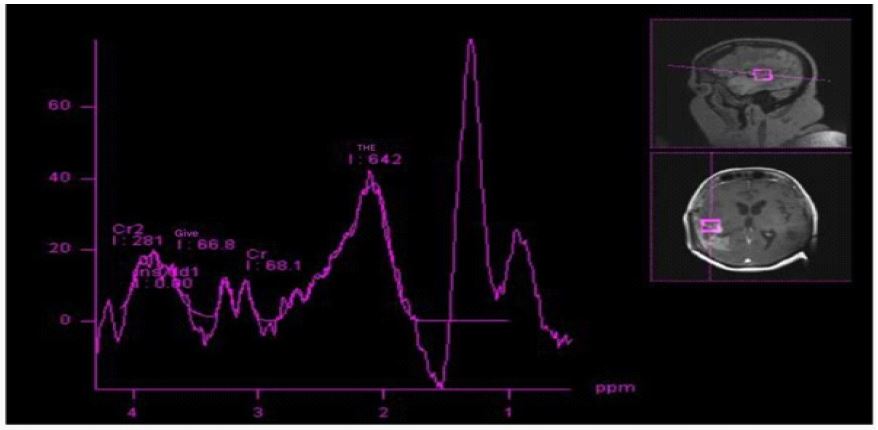
RN remains a difficult diagnosis due to overlapping radiologic and clinical features with tumor progression. In our patient, this differentiation was crucial to guide treatment. The lesion demonstrated features of both recurrent glioblastoma and radiation-induced injury. Pathology confirmed RN in the majority of the resected tissue (Figure 2). Advanced MR techniques were key to guiding further management. Multiparametric MRI—including diffusion, perfusion, and spectroscopy—helped differentiate necrotic from neoplastic processes. Spectroscopy revealed metabolic patterns compatible with non-neoplasticchanges.
RN typically presents 6–12 months post-radiotherapy but may occur years later, particularly with stereotactic radiosurgery (SRS) and reirradiation. Clinical symptoms vary by lesion location and may include headache, seizures, paresis, or speech disturbances.An institutional diagnostic algorithm should include MR spectroscopy, dynamic FET-PET, and in selected cases, biopsy or resection (Figure 3). Such structured approaches can standardize care and facilitate interdisciplinary decision-making.
Bevacizumab has emerged as a potential therapy for RN, with reported radiologic benefit. However, adverse events such as ischemic strokes and corneal ulcers have been observed. As in our case, bevacizumab reduced lesion size and edema but did not significantly alter the clinical course.
Conclusion
Cerebral radionecrosis is a frequent, under-recognized complication of radiotherapy in neuro-oncology. Accurate diagnosis via MR spectroscopy and perfusion is essential to distinguish from tumor progression. Corticosteroids remain standard therapy, although side effects are considerable. Surgical options are reserved for mass effect or life-threatening edema. Bevacizumab offers promise with fewer adverse effects but requires further validation (Figure 4). We advocate for a meta-analysis comparing therapeutic strategies to better define treatment algorithms.
References
- Mangesius J. et al. A multi-disciplinary approach to diagnosis and treatment of radio necrosis in malignant gliomas and cerebral metastases. Cancers. 2022; 14: 6264.
- Raimbault A, et al. Radionecrosis of malignant glioma and cerebral metastasis: A diagnostic challenge in MRI. Diagnostic and Interventional Imaging. 2014; 95: 986-993.
- Martins P, et al. Advances in Radiotherapy for Brain Tumors. International Journal of Cancer. 2021; 148: 1121-1130.
- Garcia L. The Challenges of Radiotherapy: Pseudoprogression and Radionecrosis. Neurosurgery Review. 2022; 39: 5-12.
- Thompson H, et al. The Role of MRI in Diagnosing Brain Tumors. Radiology Today. 2023; 12: 32-38.
- Brown K, et al. Multimodal Imaging Techniques in Tumor Assessment. Clinical Radiology v. 2021; 75: 245-252.
- Wilson S. Multiparametric MRI: A New Standard in Tumor Imaging. Journal of Clinical Oncology. 2022; 40: 1802-1809.
- Wilson S. Multiparametric MRI: A New Standard in Tumor Imaging. Journal of Clinical Oncology. 2022; 40: 1802-1809.
- Mcbane D, et al. Incidence of radionecrosis in glioma patients: a systematic review. Journal of Neuro-Oncology. 2018; 139: 19-27.
- Haber M, et al. Radiation necrosis: Pathophysiology and management. Neurosurgical Focus v. 2014; 36: 1-9.
- Ruben JD, et al. Cerebral radiation necrosis: incidence, outcomes, and risk factors with emphasis on radiation parameters and chemotherapy. International Journal of Radiation Oncology Biology Physics. 2006; 65: 499-508.
- Kerr G, et al. Clinical outcomes of patients with high-grade gliomas treated with radiotherapy. Neuro-Oncology v. 2017; 19: 1382-1392.
- Karuna Muni R, et al. Radiation necrosis in patients with brain tumors: a review of the literature. Current Oncology Reports v. 2017; 19: 1-9.
- Zhuang H, Yuan X, Zheng Y, et al. A study on the evaluation method and recent clinical efficacy of bevacizumab on the treatment of radiation cerebral necrosis. Sci Rep. 2016; 6: 24364.
- Delishaj D, Ursino S, Pasqualetti F, et al. Bevacizumab for the treatment of radiation-induced cerebral necrosis: a systematic review of the literature. J Clin Med Res. 2017; 9: 273-80.
- Chung C, Bryant A, Brown PD. Interventions for the treatment of brain radionecrosis after radiotherapy or radiosurgery. Cochrane Database of Systematic Reviews. 2018; 7: 011492.
- Thompson H, et al. The Role of MRI in Diagnosing Brain Tumors. Radiology Today v. 2023; 12: 32-38.
- White A, et al. MRS in Routine Clinical Practice: Challenges and Future Directions. Neuroradiology Journal v. 2024; 67: 77-84.
- Wilson S. Multiparametric MRI: A New Standard in Tumor Imaging. Journal of Clinical Oncology v. 2022; 40: 1802-1809.
- Bourg V, Frenay M, Cohen M, Lebrun C. Radionecrose e seu tratamento com bevacizumabe: Uma revisão de dados atuais. Oncology Journal. 2011; 58: 233-240.
- Gronier S, Bour V, Frenay M, Cohen M, Mondot L, et al. Bevacizumab para o tratamento da radionecrose cerebral. Revue Neurologique. 2011; 167: 331-336.