
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Case report: Serum-Like Sickness syndrome following ciprofloxacin intake in a 74-year-old-male
A Mouratoglou*; K Karda Makis; L Mouros; O Alexandra; C Valihas; C Touitou
2nd Department of Internal Medicine, Georgios Geminates Hospital of Athens, Greece.
*Corresponding Author : A Mouratoglou
2nd Department of Internal Medicine, Georgios Geminates Hospital of Athens, Greece.
Email: alexandra211764@gmail.com
Received : Mar 16, 2025
Accepted : Apr 07, 2025
Published : Apr 14, 2025
Archived : www.jcimcr.org
Copyright : © Mouratoglou A (2025).
Abstract
Serum-Like Sickness Syndrome (SLS) is a rare hypersensitivity reaction characterized by-immune-mediated systemic symptoms resembling serum sickness. Serum sickness-like reactions are generally less severe than classic serum sickness and can include arthralgias, lymphadenopathy, and urticaria rash, with or without fever. This case report is about a 74-year-old male who developed SLS after ciprofloxacin administration, providing insights into diagnostic criteria, clinical course, and management of this disease. The clinical presentation of this case provided a thorough differential evaluation of other possible conditions such as sepsis, Drug-Induced Hypersensitivity Syndrome (DIHS) and hypocomplementemia urticarial vasculitis. His history of allergic reactions to penicillin-based antibiotics and immunological abnormalities underscores the importance of recognizing predisposing factors for SLS.
Keywords: Serum-Like Sickness syndrome; Hypersensitivity reaction; Serum sickness.
Citation: Mouratoglou A, Karda Makis K, Mouros L, Alexandra O, Valihas C, et al. Case report: Serum-Like Sickness syndrome following ciprofloxacin intake in a 74-year-old-male. J Clin Images Med Case Rep. 2025; 6(4): 3551.
Introduction
Serum-Like Sickness Syndrome (SLS) is a hypersensitivity reaction distinguished by fever, rash, and systemic involvement without the presence of immune complex deposition, as seen in classical serum sickness. There are rare cases of serum-like sickness reported in literature, where is commonly associated with antibiotics [1], particularly beta-lactams and fluoroquinolones as well as monoclonal antibodies [2], anti-seizures medication and in some cases with hepatitis B or vaccines [3]. Given its overlapping symptoms with other hypersensitivity syndromes, a detailed clinical and laboratory evaluation is required for diagnosis.
Case presentation
A 74-year-old male was admitted to the Internal Medicine Department with a pruritic, and targetoid rash distributed over the torso and lower limbs and arthralgias mainly in his knees. Symptoms were developed after ciprofloxacin intake for a urinary tract infection. The patient reported similar symptoms during a prior episode that he reported as an allergic shock reaction to penicillin-based antibiotics. Past medical history included arterial hypertension, paroxysmal atrial fibrillation, benign prostatic hyperplasia, gastroesophageal reflux disease and a history of chronic spontaneous urticaria, diagnosed based on skin biopsy during a previous hospitalization. Findings of the biopsy were mild perivascular lymphocytic infiltrate with sporadic eosinophils, normal epidermis, negative direct immunofluorescence for IgA, IgG, IgM, C1q, C3, C4/fibrogen, while there was no evidence of vasculitis, fibrinoid necrosis, or nuclear debris. Other useful key-findings during his previous reported hospitalization were the presence of symmetrical arthritis in radiocarpal joints and mediastinal lymphadenopathy without other pulmonary diseases, reported by a chest CT-scan. At the time presented in our unit, the rash was pruritic but not painful, and during his hospital charge, he exhibited systemic symptoms that included hypotension and high fever (>38OC), requiring intensive management. Laboratory results are reported below.
Table 1: Laboratory results.
| Category | Parameter | Result | Normal Values |
|---|---|---|---|
| Hematology | Hgb | 15.9 g/dL | 13.5–17.5 g/dL (male);12–15.5 g/dL(female) |
| WBC | 15.43× 10³/μL | 4.5–11 × 10³/μL | |
| NEU | 14.52× 10³/μL | 2–7 × 10³/μL | |
| LYM | 0.55× 10³/μL | 1–3 × 10³/μL | |
| PLT | 130 × 10³/μL | 150–450 × 10³/μL | |
| Inflammatory Markers | CRP | 35 mg/L | < 5 mg/L |
| Arterial BloodGas | Lactate | 3.29 mmol/L | 0.5–2.2 mmol/L |
| Coagulation Profile | INR | 1.1 | 0.8–1.2 |
| PT | 12.8sec | 11–13.5 sec | |
| aPTT | 27 sec | 25–35 sec | |
| Renal Function | Creatinine | 1.2 mg/dL | 0.7–1.3 mg/dL(male);0.6–1.1 mg/dL(female) |
| Urea | 50 mg/dL | 7–20 mg/dL | |
| Immunoglobulins | IgG | 6.760 g/L (low) | 7–16 g/L |
| IgM | 0.635 g/L | 0.4–2.3 g/L | |
| IgE | 135 IU/mL | 0–100 IU/mL | |
| Complement System | C3 | 0.630 g/L (low) | 0.9–1.8 g/L |
| C4 | 0.089 g/L (low) | 0.1–0.4 g/L | |
| Procalcitonin (PCT) | 18.21 μg/L | 0.1-0.5 μg/L |
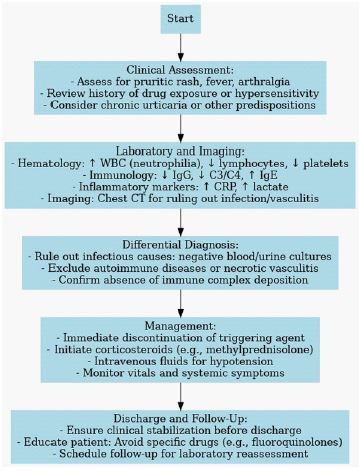
Based on clinical symptoms a chest CT was conducted, and no specific findings were reported; ground-glass opacifications, bilateral pleural effusion with consolidation, and nonspecific mediastinal lymphadenopathy (<1 cm). During the hospital stay, treatment required intravenous inotropic agents and the use of methylprednisolone. At the beginning of treatment, septic shock was included to differential diagnosis, as inflammatory markers as PCT and WBC were considerably above the normal value, so broad spectrum antibiotics were started. While an infectious case was finally excluded by negative blood and urine cultures, antibiotics were discontinued, and the patient was treated with only the intravenous cortisone and fluids. He was discarded with improved clinical picture. Diagnosis was compatible with SLS based on the evaluation of his current symptoms, past medical history, laboratory findings and exclusion of infectious/autoimmune diseases or necrotic angiitis. Herein we present with an algorithm of the evaluation and management that was performed.
Discussion
SLS is a hypersensitivity reaction that differs from classical serum sickness regarding to its pathophysiology and clinical presentation. Unlike classical serum sickness, which is an example of the Gell and Coombs “type III” or immune complex-mediated hypersensitivity disease [4], SLS lacks this hallmark feature. The presence of low complement levels (C3 and C4) and hypogammaglobulinemia suggests a predisposition to immune dysregulation, which may contribute to the development of SLS. As seen here, the patient’s history of penicillin allergy further showcases the increased susceptibility to immune-mediated hypersensitivity reactions, so allergic predisposition often represents a key factor in these cases. The diagnosis of SLS is established based on the following key criteria. Usually, an exposure to a causative agent like certain drugs or biological agents, such as antibiotics can trigger a SLS reaction. Clinical presentation includes systemic symptoms like fever, arthralgia, or more specific skin manifestations. Rash is the most common presenting feature and can take various forms, including urticarial (most common), targetoid, palpable purpura, morbilliform eruptions, papules, or maculopapular lesions. Fever is usually uncommon, intermittent and can resolve on its own, starting at 5 to 10 days after oral administration of the culprit drug. Arthralgias are a characteristic, but usually inconsistent feature of serum sickness [5]. Commonly are involved metacarpophalangeal joints, knees, wrists, ankles and shoulders. Less common symptoms are facial or peripheral edema, nonspecific headache and blurred vision, splenomegaly, peripheral neuropathy, nephropathy, vasculitis, anterior uveitis [6]. Lymphadenopathy, as seen in this patient, represents a less common manifestation. Laboratory testing includes Complete Blood Count (CBC), Erythrocyte Sedimentation Rate (ESR), C-Reactive Protein (CRP), urinalysis, and serum chemistries. These are essential for identifying systemic inflammation and ruling out other conditions. Infectious diseases, particularly hepatitis B, must be ruled out through appropriate serological testing. The measurement of C3 and C4 complement levels is valuable, as low levels are often observed in SLS. The exclusion of vasculitis and immune complex deposition is critical and can be confirmed through skin biopsy and immunofluorescence. In this patient, the presence of a targetoid rash, systemic hypotension, and the exclusion of vasculitis through biopsy findings align with the diagnosis of SLS. Drug-Induced Hypersensitivity Syndrome (DIHS) is a part of differential diagnosis, but absence of eosinophilia and multiorgan dysfunction excludes this diagnosis.
Conclusion
This case highlights the need for prompt recognition and management of serum-like syndrome, particularly in patients with prior allergic reactions and immunological abnormalities. Diagnostic confirmation relies on the exclusion of immune complex-mediated processes. Early discontinuation of the offending agent and corticosteroid therapy are critical for favorable outcomes. Further research is necessary to understand the factors that may contribute to a better understating of this condition and possible new therapeutic strategies.
References
- Yorulmaz A, Akın F, Sert A, Ağır MA, Yılmaz R, et al. Demographic and clinical characteristics of patients with serum sickness-like reaction. Clin Rheumatol. 2018; 37(5): 1389-94.
- Knowles SR, Uetrecht J, Shear NH. Idiosyncratic drug reactions: the reactive metabolite syndromes. Lancet Lond Engl. 2000; 356(9241): 1587-91.
- Apisarnthanarak A, Uyeki TM, Miller ER, Mundy LM. Serum sickness-like reaction associated with inactivated influenza vaccination among Thai health care personnel: Risk factors and outcomes. Clin Infect Dis Off Publ Infect Dis Soc Am. 2009; 49(1): 18-22.
- Lawley TJ, Bielory L, Gascon P, Yancey KB, Young NS, et al. A prospective clinical and immunologic analysis of patients with serum sickness. N Engl J Med. 1984; 311(22): 1407-13.
- Zhang Z, Xiang Y, Wang B, Chen H, Cai X, et al. Intestinal mucosal permeability of children with cefaclor-associated serum sickness-like reactions. Eur J Pediatr. 2013; 172(4): 537-43.
- Sène D, Ghillani-Dalbin P, Amoura Z, Musset L, Cacoub P. Rituximab may form a complex with IgMkappa mixed cryoglobulin and induce severe systemic reactions in patients with hepatitis C virus-induced vasculitis. Arthritis Rheum. 2009; 60(12): 3848-55.