
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Giant cell tumor of the talus: An uncommon location for a common tumor, a rare case report
Mohit Kumar*; Rajesh Lalchandani; Lokesh Pratap Singh; Rahul Sonkaria; Sanchit Jain
ESIC Hospital and PGIMSR, Basaidarapur, New Delhi 110015, India.
*Corresponding Author : Mohit Kumar
ESIC Hospital and PGIMSR, Basaidarapur, New Delhi 110015, India.
Received : Mar 16, 2025
Accepted : Apr 07, 2025
Published : Apr 14, 2025
Archived : www.jcimcr.org
Copyright : © Mohit K (2025).
Abstract
Giant Cell Tumours are benign, aggressive tumours typically found in the metaphysis of long bones, most commonly at the distal femur and proximal tibia. These most commonly affect long bones. We describe a rare occurrence of GCT in the talus bone of a young female, highlighting the clinical presentation, diagnostic process, treatment modalities, and outcomes, in this case report. The report also emphasizes the importance of early detection and appropriate management to prevent complications, including pathological fractures & joint dysfunction.
Citation: Mohit K, Lalchandani R, Pratap Singh L, Sonkaria R, Jain S. Giant cell tumor of the talus: An uncommon location for a common tumor, a rare case report. J Clin Images Med Case Rep. 2025; 6(4): 3552.
Introduction
Giant cell tumor is a benign bone neoplasm of mesenchymal origin, identified by multinucleated giant cells [1]. GCT is a locally aggressive tumor of bone composed of proliferation of mononuclear cells with scattered macrophages. It occurs between 20 to 40 years, with a 56% predominance in females. However, giant cell tumors of the talus are rare and account for a small percentage of all cases. The talus, being a weight-bearing bone, poses a unique challenge in terms of treatment due to its importance in foot mechanics. The talus is an uncommon site for ABCs. Involvement of the RANK pathway is believed to contribute to the pathogenesis of GCT.
Case presentation
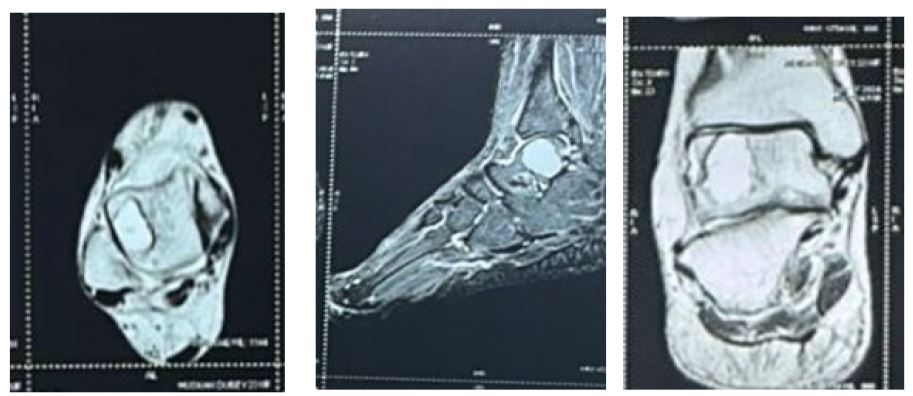
A 23-year-old female presented with complain of right ankle pain for the past five months which was insidious in onset, gradually progressive, non-radiating, localized to the anterolateral aspect of the right ankle. The pain was dull in character, persistent, and aggravated by weight-bearing activities & relieved on medications & rest. There was no history of trauma or any other similar incidence in the past. On examination of the foot, there was no visible or palpable swelling with no skin changes, normal local temperature, and tenderness to deep palpation was noted on the dorsal aspect of the ankle. The distal neurovascular integrity was intact. Ankle Radiographs showed a well-defined expansile lytic lesion in the talus bone. Further imaging studies were performed to confirm the diagnosis.


Treatment
The management of GCT involves a range of options, including curettage, bone grafting, sclerotherapy, and, in rare cases, resection of the affected bone. The aim is primarily to alleviate symptoms and prevent complications, such as fractures or joint dysfunction. In our patient, the decision was made to proceed with curettage and bone grafting. Extended Curettage is a widely used technique for managing GCT, as it allows for the removal of the lesion and preserves the surrounding bone structure. After curettage, the cavity was filled with an autologous bone graft from the iliac crest, which maintains the structural integrity of the talus & promotes healing. Post-operatively, the ankle was immobilized in a non-weight bearing below knee cast for 12 weeks.
Outcome and Follow-up
Histopathological study showed fibrocollagenous tissue comprising of large number of non-neoplastic osteoclastic like giant cell along with mononuclear cells, features suggestive of GCT. After 3 months Rehabilitation protocol focused on restoring range of motion, was started. The patient reported significant improvement in pain. Follow-up imaging at 6 months revealed satisfactory healing of the talus with complete resolution of the cystic lesion. The bone graft had integrated well with the surrounding bone & there was no recurrence.
Discussion
The favored sites of presentation are the vertebrae, flat bones, and metaphysis of long bones [3]. The talus is an unusual site for GCT. They typically affect individuals in the second or third decade of life, with a slight female predilection. Although GCT are most commonly located in the long bones, such as the femur, tibia, and humerus, their occurrence in the talus is exceedingly rare. Clinical manifestations of GCT vary depending on the location, size, and aggressiveness of the lesion. In most cases, patients present with localized pain, swelling, and, in some cases, pathologic fractures. The ankle joint, as in our case, is relatively uncommon for GCT, making the diagnosis particularly challenging. Imaging is essential for the diagnosis of GCT. Radiographs typically reveal a lytic, expansile lesion with well-defined borders. MRI is the gold standard for evaluating the lesion’s internal structure, demonstrating the classic multilocular cystic appearance, fluid- filled spaces, and septations. CT scans may be used for further evaluation, especially in cases with significant bony destruction or when surgical planning is needed. The differential diagnosis for an expansile lesion in the talus includes other benign lesions such as giant cell tumor, osteoblastoma, chondroblastoma, and fibrous dysplasia, as well as malignant lesions like metastatic bone disease. A biopsy may be required for definitive diagnosis, though imaging findings and clinical presentation are often sufficient for a presumptive diagnosis. Many authors have described excellent results with intralesional extended curettage and bone grafting for lytic lesions that were well localized within the talus [5-7].
Conclusion
GCT in the talus are extremely rare and due to their similarity to other bone lesions & uncommon location can present diagnostic challenges. Through appropriate imaging, Early diagnosis is crucial for accurate identification and treatment planning. Extended Curettage and bone grafting remain effective treatment options for GCT, and with timely intervention, favorable outcomes can be achieved. This case emphasizes the importance of considering GCT in the differential diagnosis of bone lesions in the talus, particularly in young patients presenting with unexplained ankle pain.
References
- Turcotte RE. Giant cell tumour of bone. Orthoepy Clin North Am. 2006; 37(1): 35-51. doi: 10.1016/j.ocl.2005.08.005.
- Purohit S, Pardi Wala DN. Imaging of giant cell tumour of bone. Indian J Ortho. 2007; 41(2): 91-96. doi: 10.4103/0019-5413.32037.
- Luna AR, Fernandez-Saddi H, Garcia AV, Reina Cde J, Martin JV. Aneurysmal bone cyst in children involving infrequent locations. Report on two cases. Chirr Organic Mov. 2004; 89: 347-52.
- Dhillon MS, Singh B, Gill SS, Walker R, Nagi ON. Management of giant cell tumor of the tarsal bones: A report of nine cases and a review of the literature. Foot Ankle. 1993; 14: 265-72. doi: 10.1177/107110079301400506.
- Bapat MR, Narlawar RS, Pimple MK, Bhosale PB. Giant cell tumour of talar body. J Postgrad Med. 2000; 46: 110-1.