
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Myocarditis due to eosinophilic granulomatosis with polyangiitis: Case report and literature review
Jean Carlos Souza Machado dos Santos1#; Rodrigo Mont’ Alverne Guimarães1#; Luma Maria Tavares de Sousa2*; Suellen Bergamim Tavares1; Ricardo Paulo de Sousa Rocha1; Jefferson Luís Vieira1,2
1Hospital de Messejana Dr. Carlos Alberto Studart, Fortaleza, CE, Brazil.
2Federal University of Ceará, Fortaleza, CE, Brazil.
#Co-first Authors.
*Corresponding Author : Luma Maria Tavares de Sousa
Federal University of Ceará, Fortaleza, CE, Brazil.
Email: lumamtavaress@gmail.com
Received : Mar 17, 2025
Accepted : Apr 08, 2025
Published : Apr 15, 2025
Archived : www.jcimcr.org
Copyright : © Tavares de Sousa LM (2025).
Abstract
Eosinophilic Granulomatosis with Polyangiitis (EGPA) is a rare systemic vasculitis, with cardiac involvement being one of its most severe and life-threatening complications. Early diagnosis is essential to preventing the progression of myocardial damage and reducing mortality risk through the timely initiation of targeted therapy. Cardiac Magnetic Resonance (CMR) plays a crucial role in the non-invasive characterization of myocardial tissue, enabling the early detection of cardiac involvement in EGPA. Here, we present the case of a young patient with a history of late-onset asthma, rhinitis, polyarthralgia, mononeuritis, and myocarditis secondary to EGPA, emphasizing the diagnostic approach, therapeutic management, and clinical follow-up.
Citation: Machado dos Santos JCS, Alverne Guimarães RM, Tavares de Sousa LM, Bergamim Tavares S, Sousa Rocha RPD, et al. Myocarditis due to eosinophilic granulomatosis with polyangiitis: Case report and literature review. J Clin Images Med Case Rep. 2025; 6(4): 3553.
Introduction
Eosinophilic myocarditis is a rare condition characterized by myocardial inflammation due to eosinophil infiltration. Several etiological factors can trigger this condition, including myeloproliferative diseases, parasitic infections, medications, and immune-mediated diseases such as EGPA [1]. While EGPA typically has a favorable prognosis, cardiac involvement is associated with a significantly higher mortality rate [2]. Early warning signs include dyspnea, palpitations, chest pain, syncope, arrhythmia, and unexplained heart failure, which can progress to cardiogenic shock or sudden death. The definitive diagnosis is usually made through endomyocardial biopsy (EMB) [3]. However, CMR offers a valuable non-invasive alternative, enabling the identification of key structural changes associated with myocarditis [4].
Case report
A 34-year-old female from Rio Branco, Acre, located in the Northern region of Brazil, presented to the hospital with progressive exertional dyspnea, paroxysmal nocturnal dyspnea, orthopnea, and flu-like prodromal symptoms. The initial physical examination revealed tachypnea, crackles at the lung bases, an irregular heart rhythm, and bilateral lower limb edema. She was initially diagnosed with COVID-19 pneumonia complicated by acute Heart Failure (HF) and was admitted to the ICU with acute pulmonary edema.
Initial laboratory results showed an elevated troponin level (rising from 37 to 71 ng/L) and a pro-BNP level of 5,900 pg/mL. The initial echocardiogram demonstrated diffuse hypokinesis, a left ventricular ejection fraction (LVEF) of 43%, and severe mitral regurgitation. The patient showed significant improvement after treatment with vasodilators and diuretics in the ICU. During hospitalization, her heart failure therapy was optimized with a quadruple regimen consisting of sacubitril/valsartan, spironolactone, bisoprolol, and dapagliflozin.
Despite these interventions, two weeks later, the patient was readmitted due to decompensated heart failure, reporting the onset of new symptoms during the interim between hospitalizations, including fever, vomiting, abdominal pain, arthralgia, and paresthesia in the extremities. A repeat echocardiogram showed further deterioration in ventricular function, with an LVEF of 32%.
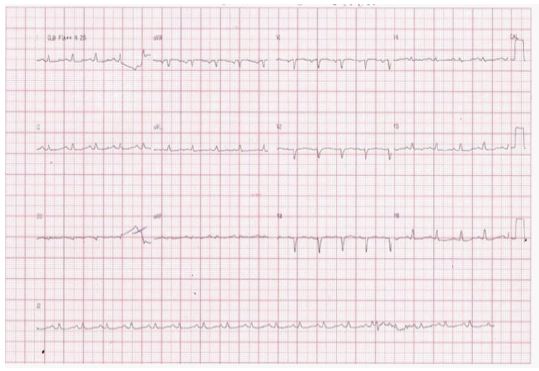
The patient was referred to an advanced heart failure center, where she was admitted with a respiratory rate of 23 breaths per minute, a heart rate of 150 bpm, diminished breath sounds at the lung bases, and lower limb edema. The initial electrocardiogram showed low-amplitude QRS complexes and slow R-wave progression in the precordial leads (Figure 1). Chest radiography revealed costophrenic angle blurring and pulmonary congestion (Figure 2). Echocardiography demonstrated worsening systolic function, with an LVEF of 29% and moderate pericardial effusion. Laboratory findings showed marked eosinophilia (27 × 10⁹/L; normal range: 3–10 × 10⁹/L), an elevated C-reactive protein (CRP) level of 49 mg/L, and an NT-proBNP level of 2,230 pg/mL.
The patient’s medical history revealed significant findings, including intermittent skin eruptions that worsened in December, during the period between hospitalizations (Figures 3 to 5), and breast implant placement four months before symptom onset. Additionally, she had a history of late-onset asthma, rhinitis, sinusopathy, inflammatory arthralgia, asthenia, lower limb paresthesia, and shoulder pain radiating to the hands, with a biceps tendon rupture identified on ultrasound. There was no history of heart disease or conventional cardiovascular risk factors.
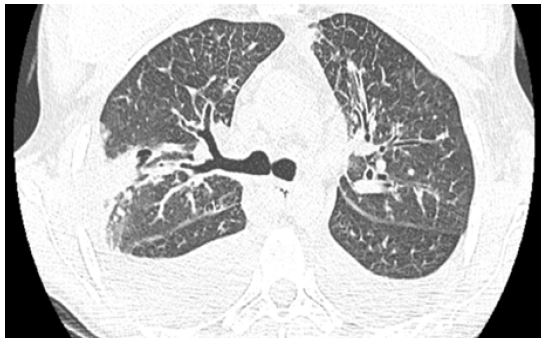
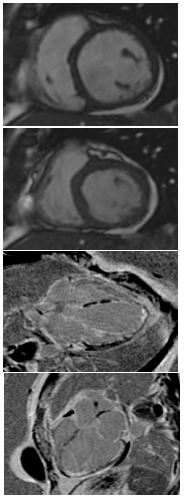
Chest computed tomography (Figures 6 and 7) revealed pulmonary congestion, bilateral pleural effusion, and pericardial effusion, with no evidence of pulmonary embolism. Cardiac Magnetic Resonance Imaging (CMR) was performed using a PHILIPS 1.5T scanner with a clinically optimized protocol to minimize scan time due to the patient’s condition. The protocol included pre-contrast cine sequences (cine b-SSFP) and Late Gadolinium Enhancement (LGE) sequences.
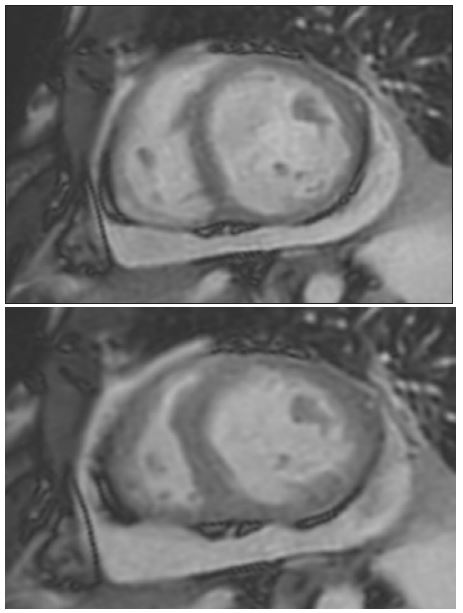
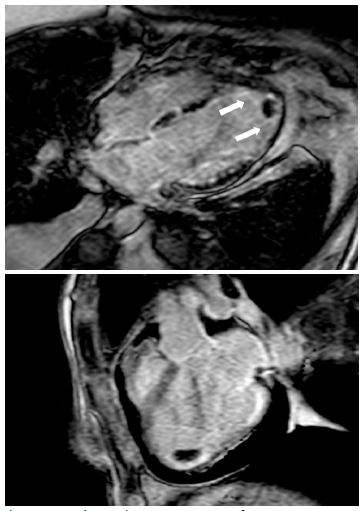
The study showed normal ventricular volumes (right ventricular end-diastolic volume index [RVEDVI] = 82 mL/m²; left ventricular end-diastolic volume index [LVEDVI] = 90 mL/m²), preserved right ventricular systolic function (RVEF = 58%), and moderate left ventricular systolic dysfunction (LVEF = 35%) due to akinesia of all apical segments and hypokinesia of the remaining myocardial segments. Using the phase-sensitive inversion recovery (PSIR) LGE technique, with inversion time adjusted to optimize healthy myocardium nulling and image acquisition approximately six minutes after contrast administration, diffuse subendocardial hyperintensity was observed, consistent with myocardial fibrosis. Additionally, moderate pericardial and bilateral pleural effusions were noted, along with the presence of a 1.4 × 1.8 cm apical thrombus in the left ventricle (Figures 8 to 12). Coronary CT angiography showed no coronary lesions or anomalies.
The investigation of eosinophilic myocarditis was extended with a bone marrow aspirate and biopsy, which revealed reactive eosinophilia, and an Electromyography (EMG), which confirmed asymmetric involvement of sensory and motor fibers in the lower limbs and the right upper limb, consistent with mononeuritis multiplex.
The combination of eosinophilia, late-onset asthma, predominantly eosinophilic extravascular inflammation, and mononeuritis multiplex led to a diagnosis of eosinophilic granulomatosis with polyangiitis (EGPA) [5]. Immunosuppressive therapy was initiated, including prednisone (1 mg/kg/day for three months, followed by a tapering regimen until the sixth month) and rituximab (1,000 mg, with a two-week interval between doses), in collaboration with the local rheumatology service.
The patient demonstrated complete symptom remission within seven days, accompanied by normalization of inflammatory biomarkers. Given the significant clinical improvement following the initiation of immunosuppressive therapy and the CMR findings suggestive of eosinophilic myocarditis, an endomyocardial biopsy was deemed unnecessary. A follow-up CMR conducted six months after symptom onset showed normal cardiac chamber dimensions, preserved right ventricular systolic function (RVEF = 56%), and partial improvement in left ventricular systolic function, with mild dysfunction and an LVEF of 49%. The pleural effusion and apical thrombus resolved after three months of treatment with apixaban 5 mg BID, and there was a substantial reduction in pericardial effusion. The patient is currently under follow-up in her home state and has had no recurrence of symptoms, receiving optimized therapy including sacubitril/valsartan 200 mg BID, spironolactone 25 mg, bisoprolol 10 mg, and dapagliflozin 10 mg.





Discussion
Eosinophilic Granulomatosis with Polyangiitis (EGPA), formerly known as Churg-Strauss syndrome, is a rare systemic vasculitis that primarily affects small and medium-sized vessels, characterized by eosinophilia and eosinophilic infiltration in various tissues. It is classified as one of the vasculitides associated with Anti-Neutrophil Cytoplasmic Antibodies (ANCA) [6], and commonly involves the skin and lungs, presenting with symptoms such as asthma, sinusitis, transient pulmonary infiltrates, and peripheral neuropathy. In the case presented, the patient progressively developed these manifestations; however, EGPA’s multisystemic nature can also involve other organs, including the heart [7]. Interestingly, there was a temporal association between the patient’s breast implant surgery and the onset of symptoms, which occurred four months post-procedure. Although there are isolated reports in the literature of patients with silicone implants developing EGPA, these studies are largely observational or case reports, limiting the ability to establish a definitive causal relationship. It is recognized that, in some instances, silicone implants may trigger a chronic immune or inflammatory response.
However, it is important to note that the majority of patients with breast implants do not develop autoimmune conditions or vasculitis [8].
The natural history of EGPA is described in three phases, which are not always clearly delineated. The first phase, or prodromal phase, is characterized by atopy, allergic rhinitis, and asthma, as occurred approximately four years prior to the patient’s cardiac involvement. The second phase, eosinophilic, involves peripheral eosinophilia and tissue infiltration, emerging during the first episode of acute heart failure. Finally, the vasculitic phase involves inflammation and potentially life-threatening involvement of multiple organs [9]. Cardiac involvement is reported in 16% to 92% of EGPA cases and is associated with high rates of morbidity and mortality. This involvement can affect any structure of the heart, manifesting as myocarditis, heart failure, pericarditis, arrhythmias, and even valvular disease. In this case, the patient developed myocarditis complicated by acute heart failure, underscoring the importance of early diagnosis and appropriate management to prevent severe complications such as mural thrombus formation and deterioration of ventricular function.
Early diagnosis of EGPA is crucial for initiating immunosuppressive therapy, but it can be challenging as manifestations typically present in isolation, and ANCA positivity occurs in only 40%-60% of patients [10]. The diagnostic criteria established by the American College of Rheumatology (ACR) include eosinophilia ≥1 × 109/L, airway obstruction, presence of nasal polyps, ANCA positivity, eosinophilic extravascular inflammation, hematuria, and motor neuropathy [11], as observed in this patient.
EGPA has two variants: the ANCA-positive form, characterized by vasculitis of small and medium vessels, and the ANCA-negative form, associated with greater cardiac involvement and eosinophilic infiltration in the affected organs, as seen in the reported case. The eosinophilic myocarditis of EGPA develops in three stages. The first stage, lasting about five to six weeks, involves subendocardial eosinophilic infiltration, which can range from asymptomatic to fulminant myocarditis. In the second stage, lasting approximately ten months, thrombus formation occurs in the apical and trabecular regions, as well as thickening of the heart valves and subvalvular apparatus. The third stage, or fibrotic phase, is marked by subendocardial fibrosis, with complications such as restrictive physiology, valvular regurgitation, and heart failure, as observed with the presence of myocardial fibrosis in this patient.
The Endomyocardial Biopsy (EMB) is considered the definitive method for diagnosing eosinophilic myocarditis. However, its sensitivity is relatively low, estimated at around 50%, and its routine use is limited due to the risk of severe complications, such as cardiac tamponade, as well as concerns related to cost and availability [12,13]. Therefore, Cardiac Magnetic Resonance (CMR) has been recommended by the International Consensus Group of Cardiovascular Magnetic Resonance as the primary diagnostic method, in conjunction with clinical evidence [14].
Cardiac Magnetic Resonance (CMR) is considered the gold standard for evaluating cardiomyopathies, as it allows for detailed tissue characterization, as well as assessment of cardiac function and anatomy. Studies show that CMR can detect cardiac abnormalities in patients with EGPA, even in the absence of symptoms. T1 and T2 mapping techniques, which are promising for detecting diffuse fibrosis and inflammation, can identify early cardiac involvement even in the absence of late gadolinium enhancement, making them highly relevant for the precise monitoring of cardiac involvement in patients with ANCA-associated vasculitis.
In this case, the introduction of immunosuppressive therapy with prednisone and rituximab led to a rapid remission of symptoms and normalization of inflammatory markers. Rituximab, a monoclonal anti-CD20 antibody, specifically targets B cells, which play a central role in the pathogenesis of ANCA-associated vasculitis. Studies suggest that rituximab is not inferior to cyclophosphamide in inducing remission in severe ANCA vasculitis and may even show superiority in cases of recurrent disease [15]. Furthermore, the potential for cyclophosphamide to induce infertility, especially in patients of reproductive age, strengthened the choice of rituximab as a safer alternative in this case [16,17].
The follow-up CMR revealed significant improvement in ventricular function, resolution of pleural and pericardial effusions, and disappearance of the apical thrombus, underscoring the importance of appropriate treatment in functional recovery and reduction of complications.
Conclusion
Eosinophilic myocarditis due to EGPA, although rare, should be considered in the differential diagnosis of acute heart failure. Cardiac Magnetic Resonance (CMR), with its non-invasive nature and high sensitivity, can provide an early diagnosis and help prevent complications associated with Endomyocardial Biopsy (EMB), enabling effective therapeutic management that can potentially modify the clinical course.
References
- FOZING, Thierry, ZOURI, Nayef, TOST Axel, et al. Management of a Patient with Eosinophilic Myocarditis and Normal Peripheral Eosinophil Count. Circulation: Heart Failure, [SL]. Ovid Technologies (Wolters Kluwer Health). 2014; 7(4): 692-694. http://dx.doi.org/10.1161/circheartfailure.114.001130.
- FURUTA S, et al. Update on eosinophilic granulomatosis with polyangiitis. Allergol Int. 2019.
- CAFORIO A, PANKUWEIT S, ARBUSTINI E, BASSO C, GIMENO-BLANES J, et al. European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: A position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart. 2013; 34(33): 2636-48, 2648a-2648d. doi: 10.1093/eurheartj/eht210.
- AGGARWAL HK, JAIN D, KAVERAPPA V, JAIN P, KUMAR A, et al. Síndrome hipereosinofílica idiopática manifestando-se como endocardite de Loeffler grave. Arq Bras Cardiol. 2013; 100(4): e43-e46.
- GRAYSON PC, PONTE C, SUPPIAH R, ROBSON JC, CRAVEN A, et al. DCVAS Study Group. American College of Rheumatology/European Alliance of Associations for Rheumatology Classification Criteria for Eosinophilic Granulomatosis with Polyangiitis. Ann Rheum Dis. 2022; 81(3): 309-314. doi: 10.1136/annrheumdis-2021-221794.
- KOZAK M, GILL E, GREEN LS. The Churg-Strauss syndrome: A case report with angiographically documented coronary involvement and a review of the literature. Chest. 1995; 107: 578-580.
- ROSENBERG M, LORENZ HM, GASSLER N, KATUS HA, FREY N. Rapid progressive eosinophilic cardiomyopathy in a patient with Churg-Strauss syndrome (CSS). Clin Res Cardiol. 2006; 95(5): 289-294. doi:10.1007/s00392-006-0364-06.
- WATAD A, ROSENBERG V, TIOSANO S, et al. Silicone breast implants and the risk of autoimmune/rheumatic disorders: A real-world analysis. Int J Epidemiol. 2018; 47(6): 1846-1854. doi:10.1093/ije/dyy217.
- GHOSH S, BHATTACHARYA M, DHAR S. Churg-Strauss syndrome. Indian J Dermatol. 2011; 56(6): 718-21. doi: 10.4103/0019-5154.91836.
- GHOSH S, BHATTACHARYA M, DHAR S. Churg-Strauss syndrome. Indian J Dermatol. 2011; 56(6): 718-21. doi: 10.4103/0019-5154.91836.
- GRAYSON PC, PONTE C, SUPPIAH R, ROBSON JC, CRAVEN A, et al. DCVAS Study Group. American College of Rheumatology/European Alliance of Associations for Rheumatology Classification Criteria for Eosinophilic Granulomatosis with Polyangiitis. Ann Rheum Dis. 2022; 81(3): 309-314. doi: 10.1136/annrheumdis-2021-221794.
- MONTERA MW, MARCONDES-BRAGA FG, SIMÕES MV, et al. Brazilian Society of Cardiology Guideline on Myocarditis - 2022. Arq Bras Cardiol. 2022; 119(1): 143-211. doi:10.36660/abc.20220412.
- REZAIZADEH H, SANCHEZ-ROSS M, KALUSKI E, KLAPHOLZ M, HAIDER B, et al. Acute eosinophilic myocarditis: diagnosis and treatment. Acute Card Care. 2010; 12(1): 31-6. doi:10.3109/17482940903578998.
- FRIEDRICH MG, SECHTEM U, SCHULZ-MENGER J, et al. Cardiovascular magnetic resonance in myocarditis: A JACC White Paper. J Am Coll Cardiol. 2009; 53(17): 1475-87. doi:10.1016/j.jacc.2009.02.007.
- STONE JH, MERKEL PA, SPIERA R, et al. Rituximab versus cyclophosphamide for ANCA-associated vasculitis. N Engl J Med. 2010; 363(3): 221-232. doi:10.1056/NEJMoa0909905.
- TEIXEIRA V, MOHAMMAD AJ, JONES RB, SMITH R, JAYNE D. Efficacy and safety of rituximab in the treatment of eosinophilic granulomatosis with polyangiitis. RMD Open. 2019; 5(1): e000905. doi:10.1136/rmdopen-2019-000905.
- MOHAMMAD AJ, HOT A, ARNDT F, et al. Rituximab for the treatment of eosinophilic granulomatosis with polyangiitis (Churg-Strauss). Ann Rheum Dis. 2016; 75(2): 396-401. doi:10.1136/annrheumdis-2014-206095.