
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Lower limb plegia following subarachnoid hemorrhage
Francisco Ortuño-Andériz F¹,²*; Manuela Jorquera-Moya³; Elena Valdés-Franci¹; Laura Castrillo-Cortecedo¹
1Department of Intensive Care Medicine, Hospital Clínico San Carlos, Madrid, Spain.
2Professor of Medicine, Complutense University of Madrid, Spain.
3Neuroradiology Unit, Department of Radiology, Hospital Clínico San Carlos, Madrid, Spain.
*Corresponding Author : Ortuño-Andériz F
Department of Intensive Care Medicine, Hospital Clínico San Carlos, Madrid, Spain.
Email: portunoa@yahoo.es
Received : Mar 24, 2025
Accepted : Apr 10, 2025
Published : Apr 17, 2025
Archived : www.jcimcr.org
Copyright : © Ortuño-Andériz F (2025).
Abstract
Lower limb plegia following Subarachnoid Hemorrhage (SAH) is an extremely rare entity with an unknown pathophysiology. A literature review revealed only one previously reported case similar to ours, where the clinical presentation was attributed to the migration of subarachnoid blood into the thecal sac, exerting a local effect that resulted in an acute spinal syndrome. The condition resolved spontaneously within a few weeks.
Keywords: Subarachnoid hemorrhage; Plegia; Lower limbs; Thecal sac; Spinal syndrome.
Citation: Ortuño-Andris F, Jorquera-Moya M, Valdés-Fruncí E, Castrillo-Cortecedo L. Lower limb plegia following subarachnoid hemorrhage. J Clin Images Med Case Rep. 2025; 6(4): 3558.
Introduction
We present an exceptional case, scarcely described in the literature, of lower limb paraplegia following a Subarachnoid Hemorrhage (SAH) in a 37-year-old professional flamenco dancer with no relevant medical history.
Case presentation
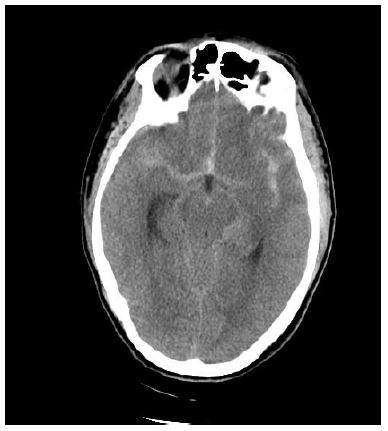
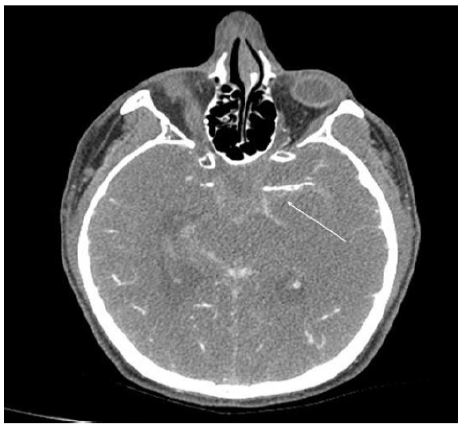
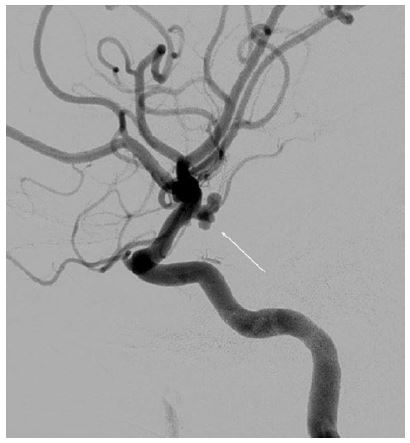
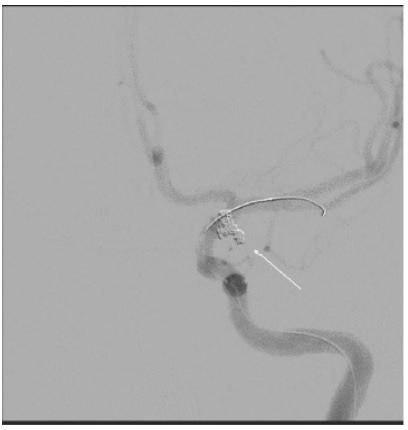
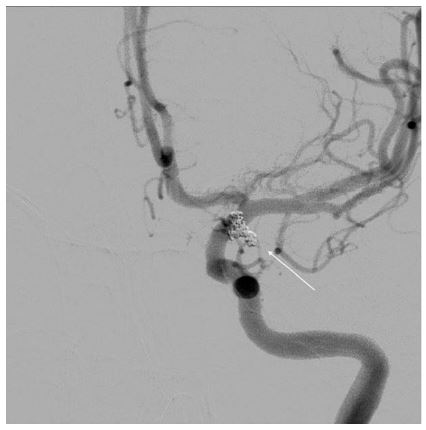
The patient was brought to the hospital intubated and on mechanical ventilation due to a decreased level of consciousness (Glasgow Coma Score of 3) following a generalized tonic-clonic seizure. An emergency cranial computed tomography (CT) scan revealed a Fisher grade IV, Hunt and Hess grade IV SAH with an intraventricular component (blood in the occipital horn of the left lateral ventricle) (Figure 1). A 3.4 mm aneurysm with a 1.7-mm neck was identified in the left choroidal artery, adjacent to the ipsilateral carotid and middle cerebral arteries (Figure 2). An external ventricular drainage catheter was placed, and the patient underwent cerebral angiography with coil embolization of the aneurysm, achieving excellent results (Figures 3-5). The initial clinical course was favorable, with no further seizures or intracranial hypertension, allowing for extubation on day 5. The patient remained conscious and oriented (GCS 15) but developed progressive lower limb paresis, eventually evolving into plegia. Neurological examination revealed abolished deep tendon reflexes, an indifferent plantar reflex, no clonus, and preserved perineal sensitivity. A transcranial Doppler ultrasound showed no evidence of elevated velocities, ruling out cerebral vasospasm. Electromyography (EMG) demonstrated the absence of voluntary activity in the lower limb muscles, with motor unit potentials within normal limits in response to nociceptive stimuli. Sensory and motor conduction velocities were normal, with intact potentials in the femoral and posterior tibial nerves.
The absence of voluntary activity, with improved muscle recruitment upon nociceptive stimulation, suggested a central etiology, ruling out generalized or focal neuropathy in the lower limbs. A brain Magnetic Resonance Imaging (MRI) scan was unremarkable. However, a spinal MRI revealed a hematocrit level within the thecal sac in the lumbar region extending dorsally (Figure 6). With conservative management, the patient experienced a spontaneous recovery of lower limb mobility, and the flaccid paraplegia resolved within weeks, allowing for a return to professional activities within a few months.

Discussion/conclusion
Paraplegia following SAH is an extremely rare complication. A literature review identified only one case similar to ours [1]. Spinal arachnoiditis following SAH has been reported to cause paresis or plegia of the lower limbs, although its incidence is estimated at less than 1% [2,3]. These cases typically present with low back pain followed by varying degrees of lower limb paresis, persisting for months or even years. One proposed mechanism involves hemolysis of subarachnoid blood leading to leptomeningeal irritation, subsequently causing arachnoiditis and potentially progressing to syringomyelia [4]. However, such cases typically have a chronic and prolonged course, in contrast to the rapid onset and resolution observed in our patient. A previous report described spinal migration of blood following SAH due to a ruptured vertebral artery [5]. In that case, the initial presentation included lumbar pain and lower limb weakness, differing from our case, in which paraplegia was triggered by an SAH of aneurysmal origin. In our case, the presence of blood in the thecal sac resulted from its migration from the cerebral subarachnoid space. The only previously reported similar case also presented with acute onset and rapid progression of symptoms. In that instance, the condition resolved following lumbar puncture to evacuate the blood, suggesting that decompression of the thecal sac played a crucial role in recovery [1]. Furthermore, clinical improvement coincided with radiological resolution, and neither cerebral nor spinal arterial vasospasm was identified as a contributing factor. The absence of cauda equina syndrome in our case suggests a lesion above L1, without significant lower radicular compression. The flaccid plegia and areflexia initially pointed to lower motor neuron involvement or an acute phase of central cord injury. EMG findings indicated absent voluntary muscle activity with preserved motor and sensory potentials in the femoral and tibial nerves, along with muscle recruitment in response to nociceptive stimuli. Thus, the initial flaccid plegia with areflexia, along with preserved perineal sensation, supports the hypothesis of an acute spinal cord injury localized to the dorsal or upper lumbar region, without complete cord involvement. The subsequent full recovery suggests the absence of a structural myelopathy.
The precise pathophysiology remains uncertain, but several hypotheses can be considered:
1. Undetected vasospasm of small spinal arteries, not visible on MRI.
2. Toxic and inflammatory effects of subarachnoid blood at the local level.
3. Increased cerebrospinal fluid pressure at the spinal level, leading to perfusion deficits due to mechanical compression. This last hypothesis is supported by a previously reported case similar to ours, in which relief of thecal sac pressure resulted in rapid clinical resolution [1].
In our case, no lumbar puncture was performed to drain subarachnoid blood, but we postulate that clinical improvement coincided with blood reabsorption. Unfortunately, the patient was lost to follow-up, and no subsequent MRI was obtained to confirm this hypothesis.
References
- Yi-Chun C, Chung-Hsih L, Wen-Hsien C, Yuang-Seng T. Acute Paraplegia After Aneurysmal SAH: A Case Report of a Rare Complication and Review of the Literature. World Neurosurg. 2016; 88: 695-9.
- Kok AJ, Verhagen WI, Bartels RM, van Dijk R, Prick MJ. Spinal arachnoiditis following subarachnoid haemorrhage: report of two cases and review of the literature. Acta Neurochir (Wien) 2000; 142: 795-9.
- Van Heerden J, McAuliffe W. Spinal arachnoiditis as a consequence of aneurysm-related subarachnoid haemorrhage. J Med Imaging Radiat Oncol. 2013; 57: 61-4.
- Nakanishi K et al. Spinal syringomyelia following subarachnoid hemorrhage. J Clin Neurosci. 2012; 19: 594-7.
- Ovalı GY et al. Symptomatic spinal migration of SAH due to ruptured intradural vertebral artery aneurysm. J Neuroimaging 2015; 25: 668-70.