
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 6
Nasal and laryngeal telangiectasia in a 65-year-old patient with Osler-Weber-Rendu disease: Clinical image
Karima Ouardi*; Aiman Fettouhi; Bouchaib Hemmaoui; Fouad Benariba; Noureddine Errami
Department of Otorhinolaryngology – Head and Neck Surgery, Mohammed V Military Hospital, Rabat, Morocco.
*Corresponding Author : Karima Ouardi
Department of Otorhinolaryngology – Head and Neck Surgery, Mohammed V Military Hospital, Rabat, Morocco.
Email: k.ouardi15@gmail.com
Received : Mar 24, 2025
Accepted : Apr 11, 2025
Published : Apr 18, 2025
Archived : www.jcimcr.org
Copyright : © Ouardi K (2025).
Keywords: Hereditary Hemorrhagic Telangiectasia (HHT); Refractory epistaxis; Telangiectasia; Arteriovenous malformations.
Citation: Ouardi K, Fettouhi A, Hemmaoui B, Benariba F, Errami N. Nasal and laryngeal telangiectasia in a 65-year-old patient with Osler-Weber-Rendu disease: Clinical image. J Clin Images Med Case Rep. 2025; 6(4): 3559.
Description
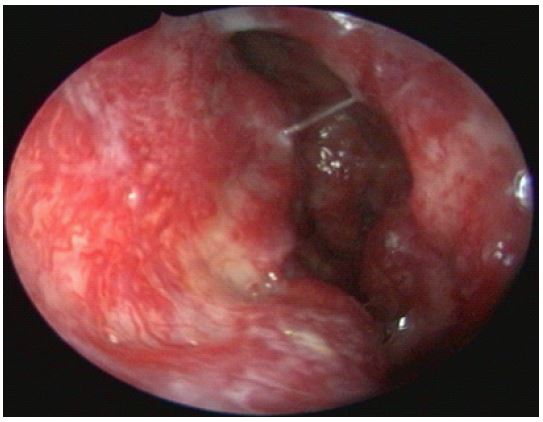
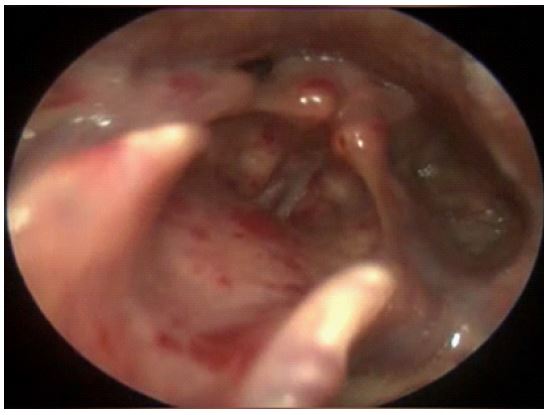
Osler-Weber-Rendu disease, also known as hereditary hemorrhagic telangiectasia, is a rare autosomal dominant hereditary vascular disease, Phenotypic variation is extreme ranging from asymptomatic to severely symptomatic, from cases with no or few mucocutaneous lesions to those with diffuse cutaneous telangiectasia of 2-3 mm diameter that are found on the skin and mucosal surfaces, particularly the face, lips, mouth, and nasopharynx. The mucosal lesions usually blanch on pressure and are highly vulnerable to spontaneous rupture and cause bleeding. Visceral vascular dilation causes arteriovenous shunts can occur in various organs, such as the central nervous system, lungs, liver, and spine. Hence the severity of the disease. Refractory Epistaxis from nasal mucosal telangiectasia, being the most common presentation of this disease that is seen in 32-85%, may lead to chronic anemia [1]. It represents a handicap inevitably impairing quality of life and social life [2]. Otolaryngologists are often the first to be consulted for recurrent epistaxis and should not overlook this condition. The diagnosis is made based on the Curaçao criteria that includes epistaxis, telangiectasia, visceral lesions, and family history. The diagnosis is confirmed by the presence of at least three of these manifestations. We present the case of a 65-year-old patient with a history of refractory epistaxis since childhood and a family history of epistaxis in a first-degree relative. ENT Clinical examination revealed telangiectasias of the nasal mucosa (Figure 1) and laryngeal mucosa (Figure 2). Systemic screening identified multiple angiodysplasias in the stomach, duodenum, and lungs. Management of epistaxis in HHT patients should follow the SFORL guidelines, which recommend initial referral to a specialized center for initial visceral work-up, genetic confirmation and annual follow-up. First-line treatment for acute epistaxis in Rendu-Osler Weber disease is bidigital compression after nasal cleansing. In case of failure, resorbable packing should be associated with systematic antibiotic prophylaxis. Embolization is reserved to cases of resistance to local treatment with fall in red blood-cell count. Non-resorbable packing and chemical or electric cauterization are not recommended. Nasal mucosa telangiectasia can be treated by sclerosing agent injection, hemostatic gel, and laser or radiofrequency ablation. When local treatment fails to provide adequate control of epistaxis, systemic tranexamic acid (Exacyl®) is recommended if there are no cardiovascular contraindications. Systemic administration of bevacizumab (Avastin®) has proved effective, but is reserved to reference centers [3].
References
- Babin E, Borsik M, Braccard S, et al. [Treatments of hereditary hemorrhagic telangiectasia of the nasal mucosa]. Rev Laryngol Otol Rhinol. 2005; 126(1): 43-8.
- Shovlin CL. Hereditary hemorrhagic telangiectasia: Pathophysiology, diagnosis, and treatment. 2010; 24(6): 203-19.
- L Robard, J Michel, et al. Guidelines of the French Society of Otorhinolaryngology (SFORL) (short version). Specific treatment of epistaxis in Rendu-Osler-Weber disease. European Annals of Otorhinolaryngology, Head and Neck Diseases. 2017; 134(1): 37-41.