
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Menstrual irregularities (amenorrhea) caused by isotretinoin
Syed M Aftab Alam Shah; Gao Lihua; Lu Jianyu*
Department of Dermatology, Xiangya Third Hospital, Medical School of Central South University, Changsha, Hunan Province, P.R. China.
*Corresponding Author : Lu Jianyu
Department of Dermatology, Xiangya Third Hospital, Medical School of Central South University, Changsha, Hunan Province, P.R. China.
Tel: 008613975130008;
Email: xiaoyun3@csu.edu.cn &
228319004@csu.edu.cn
Received : Mar 24, 2025
Accepted : Apr 11, 2025
Published : Apr 18, 2025
Archived : www.jcimcr.org
Copyright : © Jianyu L (2025).
Abstract
Isotretinoin, a systemic retinoid, is mainly indicated in very severe acne vulgaris unresponsive to other therapies, for example, topical therapy or antibiotics. Being a synthetic derivative of vitamin A, isotretinoin inhibits the activity of sebaceous glands, normalizes the keratinization process in the follicles, and also has an anti-inflammatory effect, thereby proving efficient in acne management. Although efficacious, isotretinoin is associated with a wide array of possible side effects, which include dryness of the skin, mucosal irritation, and psychiatric disturbances. Among its less well-known but important side effects is its effect on menstrual cycles, manifesting as menstrual cycle irregularities, delayed cycles, amenorrhea, or menorrhagia. This case report details a female patient who was taking isotretinoin for acne vulgaris and developed menstrual irregularities in the form of delayed cycles and amenorrhea. Hormonal investigations, such as serum estradiol and progesterone levels, corroborated the strong temporal relationship between isotretinoin treatment and the development of these disturbances. Discontinuation of isotretinoin resulted in the restoration of her menstrual cycle within 2 months. The case highlights the need for physicians to monitor the menstrual status of patients on isotretinoin treatment, with a view to active management of this understated side effect. Clinicians may maximize patient care and enhance overall therapeutic results by incorporating menstrual monitoring into treatment regimens.
Citation: Shah SMAA, Lihua G, Jianyu L. Menstrual irregularities (amenorrhea) caused by isotretinoin. J Clin Images Med Case Rep. 2025; 6(4): 3560.
Introduction
Isotretinoin is a potent oral retinoid used mainly in the management of severe acne vulgaris, especially when other forms of treatment, like antibiotics or topical medications, have failed [1]. Isotretinoin inhibits sebum secretion, normalizes keratinization of the follicle, and has an anti-inflammatory effect to bring about marked relief in the severity of acne [2]. Although efficacious, isotretinoin is associated with a wide array of well-documented side effects, such as dryness of the skin, mucosal irritation, and teratogenicity [3]. A less frequent but important side effect is the disturbance of hormonal balance, which may manifest as menstrual irregularities in female patients [4]. The irregularities may manifest as delayed cycles, amenorrhea, and menorrhagia, though these are usually underreported and not discussed in routine practice. Although the effect of isotretinoin on menstruation is not a commonly discussed topic in the literature, there is now sufficient evidence to warrant closer endocrine monitoring during therapy. Here, we report a female patient who experienced menstrual disruption during isotretinoin treatment, highlighting the value of proactive monitoring and further awareness of this side effect that continues to be underemphasized in dermatologic practice. This case highlighted the necessity of increased vigilance and multi-faceted management approaches in female patients on isotretinoin therapy.
Case presentation
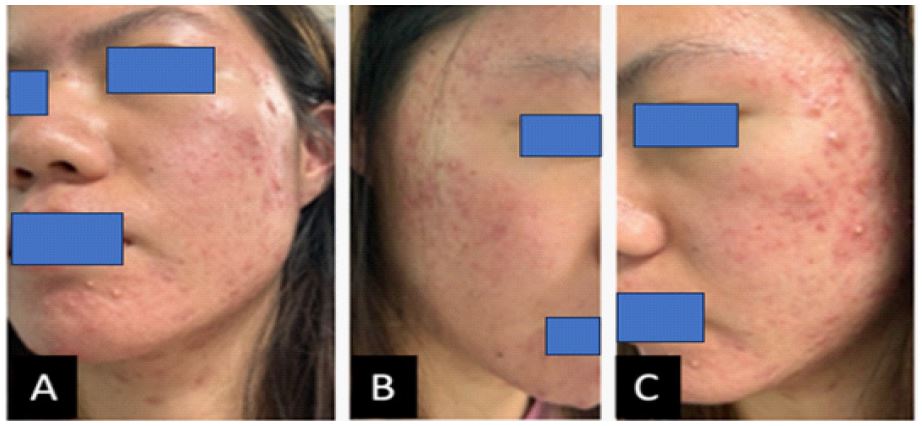
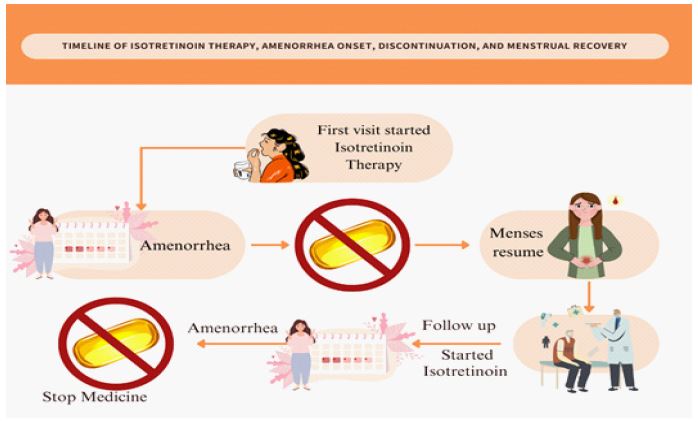
Ms. A, a 21-year-old female patient with a history of resistant acne vulgaris, was unresponsive to regular topical therapy and oral antibiotics. She was properly investigated and started on isotretinoin therapy in the form of 10 mg twice daily for two months (Figure 1). Her menstrual cycles were regular prior to initiating isotretinoin, and she did not have a history of any significant menstrual disturbances or underlying endocrine disease. A month following the start of isotretinoin treatment, the patient had, for the first time in her life, developed menstrual cycle irregularity in the form of amenorrhea. Otherwise, the patient was asymptomatic at presentation, without any physical or psychological complaints of significance. She also lacked any signs of systemic involvement, weight, appetite, or mood changes. Endocrine investigations to assess any endocrine cause of amenorrhea were completed according to the presentation. Investigations revealed normal progesterone and estradiol, and a negative pregnancy test ruled out pregnancy as a potential etiology. Further investigations to exclude other etiologies of menstrual abnormality, including complete blood count and thyroid function tests, were all within normal limits. Based on the chronological relationship between the start of isotretinoin and the development of amenorrhea and the lack of any other discernible cause, a relationship between isotretinoin treatment and menstrual disturbance was considered. In the absence of an alternative evident cause for the symptom, isotretinoin treatment was continued and the patient’s menstrual function and overall health closely monitored. At the end of the two-month course of isotretinoin, the drug was discontinued. Three weeks after drug withdrawal, the patient’s menstrual cycle had returned to normal, and amenorrhea did not recur (Figure 2). Her acne also improved, and she experienced a cumulative reduction in acne lesions, her primary concerns at the time of therapy initiation. No impact on her long-term menstrual status was observed in the months subsequent to drug withdrawal. This report describes the side effects of menstrual irregularities, including amenorrhea, as isotretinoin therapy complications. These side effects are rare and perhaps underreported in the literature, yet this case shows how crucial it is to monitor menstrual status throughout isotretinoin therapy, particularly in women with regular menses. Normalization of amenorrhea after stopping isotretinoin shows that the effects would be most likely to be dose-dependent and reversible, and this is why practitioners should remember this side effect and treat it accordingly when it is present.
Discussion
a retinoid derivative of vitamin A, is perhaps the most effective treatment for severe nodular acne vulgaris that fails to respond to other treatments [5]. Isotretinoin decreases sebum, normalizes keratinization, and has anti-inflammatory properties that act synergistically to render it an effective cure against chronic acne. Yet, although therapeutically useful, isotretinoin is also associated with a myriad of side effects that are dermatologic, gastrointestinal, musculoskeletal, or psychiatric [6]. Among them of particular importance to female patients is the tendency for menstrual irregularity, which has been poorly characterized in the literature. The development of menstrual irregularities with isotretinoin treatment continues to be underappreciated, with important implications for female patients [7]. In the cases presented here, the development of amenorrhea in a patient taking isotretinoin underscored the necessity for more vigilant monitoring of hormonal status while on therapy. Isotretinoin has also been noted to affect the Hypothalamic-Pituitary-Gonadal (HPG) axis that controls reproductive hormones [8]. Although the precise mechanisms through which isotretinoin influences menstrual cycles are unclear, it is theorized that isotretinoin can disrupt the normal activity of the HPG axis, causing interference with the secretion of Gonadotropin-Releasing Hormone (GnRH), thereby influencing the release of Luteinizing Hormone (LH) and follicle This hormonal interference is perhaps accountable for the menstrual irregularities experienced by some patients. Although isotretinoin-related menstrual irregularities are not present in every case and are, in any case, mostly considered to be temporary, they do highlight the necessity for careful monitoring of female patients undergoing treatment. As indicated in the case report, amenorrhea was reversed within three weeks following isotretinoin discontinuation, demonstrating that these disturbances are reversible. Nevertheless, the possible effect of isotretinoin on reproductive function requires more active monitoring of menstrual cycles during treatment, especially in regular cycle women before treatment. Follow-up visits at regular intervals should cover inquiries about menstrual well-being and review of any probable side effects that may affect quality of life. The findings also point to the need for patient education about the possible endocrine actions of isotretinoin. Patients should be informed about the possibility of menstrual disturbances and what they can do if such disturbances occur. Early reporting of any changes can minimize anxiety, enable appropriate management, and prevent delays in adjusting treatment.
Conclusion
Menstrual irregularities are a noteworthy side effect of isotretinoin that warrants clinicians’ attention. The cases presented demonstrate the importance of monitoring menstrual cycles and the need for further research to explore the mechanisms behind these hormonal changes.
Primary takeaway: Clinicians should proactively address menstrual health in female patients receiving isotretinoin to ensure comprehensive care and improve patient outcomes.
Acknowledgments: We want to thank the clinical staff at Xiangya Third Hospital for their support in gathering data and managing patient care.
References
- Ganceviciene R, Zouboulis CC. Isotretinoin: state of the art treatment for acne vulgaris. JDDG: Journal der Deutschen Dermatologischen Gesellschaft. 2010; 8: 47-59.
- Kim HJ, Kim YH. Exploring Acne Treatments: From Pathophysiological Mechanisms to Emerging Therapies. International Journal of Molecular Sciences. 2024; 25(10): 5302.
- Brzezinski P, Borowska K, Chiriac A, Smigielski J. Adverse effects of isotretinoin: A large, retrospective review. Dermatologic therapy. 2017; 30(4): 12483.
- Chelliah P, Glass D. Comprehensive review of reports of menstrual irregularities associated with isotretinoin. International Journal of Women’s Dermatology. 2020; 6(5): 365-7.
- Liu M, Huang YYM, Hsu S, Kass JS. Neurological and neuropsychiatric adverse effects of dermatologic medications. CNS drugs. 2016; 30: 1149-68.
- Alhetheli G, Alhazmi S, Almutairi S, Alharbi S, Alharbi N, et al. The effects of isotretinoin on the menstrual cycle: A cross-sectional study. Clinics and Practice. 2022; 12(6): 908-17.
- Szabo B. Antiandrogenic effect of isotretinoin: is the retina involved in mechanism of action? Medical hypotheses. 2007; 69(6): 1281-3.