
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Review Article - Open Access, Volume 6
Healing beyond the surface: Unraveling the psycho-dermatological link between mental health, hormones, and skin wellness
Alina Jacob2,3; Anita Jacob4; Kevin B Sneed1,5; Yashwant Pathak1,5*
1Taneja College of Pharmacy, University of South Florida, Tampa, Florida, USA.
2University of South Florida, Tampa, Florida, USA.
3Judy Genshaft Honors College, University of South Florida, Tampa, Florida, USA.
4Herbert Wertheim College of Medicine, Florida International University, Miami, Florida, USA.
5Adjunct Professor, Faculty of Pharmacy, Airlangga University, Surabaya, Indonesia.
*Corresponding Author : Yashwant Pathak
Adjunct Professor, Faculty of Pharmacy, Airlangga University, Surabaya, Indonesia.
Email: ypathak1@usf.edu
Received : Mar 19, 2025
Accepted : Apr 16, 2025
Published : Apr 23, 2025
Archived : www.jcimcr.org
Copyright : © Pathak Y (2025).
Abstract
The unique relationship between psychological well-being and dermatological health has been a topic of discussion in recent years. This literature review aims to explore and understand the connection between the mind and the skin, also known as the psych dermatological interface. Stress, anxiety and depression in addition to other mental health conditions have been shown to exacerbate inflammatory dermatological conditions such as psoriasis, eczema, acne and urticaria by dysregulation of neurotransmitter pathways such as the Hypothalamic-Pituitary-Adrenal (HPA) axis that increases cortisol production and promotes chronic inflammation. Neurotransmitters including dopamine, serotonin, epinephrine and cortisol are essential in mood regulation and skin homeostasis. Once the connection between mental health and the presentation of dermatological conditions is understood, there are a variety of psych dermatology treatment approaches. There are holistic, integrative approaches that include both dermatological treatments that may include pharmaceuticals with psychiatric treatments such as cognitive-behavioral therapy that target neuroendocrine and immune pathways. Preventative strategies including stress management, dietary changes, exercise and sleep hygiene have all been shown to control the manifestation of related dermatological symptoms. This review emphasizes the significance of understanding psych dermatological disorders and explores the mental health interventions and lifestyle modifications that play a crucial role in dermatologic care, ultimately improving patient outcomes.
Keywords: Skin disorders; Psycho dermatological challenges; Mental health and skin disorders; Hormones and skin disorders; Skin wellness.
Citation: Pathak Y, Jacob A, Jacob A, B Sneed K. Healing beyond the surface: Unraveling the psycho-dermatological link between mental health, hormones, and skin wellness. J Clin Images Med Case Rep. 2025; 6(4): 3566.
Introduction
The mind-skin connection, also known as psycho-dermatology, explores how mental health and hormonal fluctuations influences dermatological well-being. The interplay between the two disciplines highlights the relationship between mental health and skin conditions such as acne, eczema, and psoriasis. This paper examines how mental health hormones, such cortisol and serotonin, impact skin health, exacerbating skin conditions such as acne, eczema, and psoriasis, and proposes integrative approaches for holistic care.
Importance of mental health in overall well-being
Mental health is a crucial component in one’s overall well-being, affecting how individuals think, feel, and act. This, hence, influences one’s ability to handle stress, relate to others emotionally, and make physically and mentally healthy choices [1]. With increasing evidence by published studies by the National Institutes of Health (NIH), they highlight that adults that possess mental health concerns are at higher risk for behavioral and emotional problems. Mental disorders that are most likely to lead to physical disorders, especially in adolescents, include depression, anxiety, and disorders such as oppositional defiant disorder (ODD) [2]. Mental disorders can unintentionally lead to the weakening or the alteration of the immune system. There is evidence to suggest that such illnesses can lead to decreased immune functioning and immunity, with depression in particular linked to changes in cellular immunity [2]. Significance of dermatological health in daily life Healthy skin is vital for more than just aesthetic reasons; it serves as a barrier against environmental hazards, regulates body temperature, and provides sensory information. Skin, the body’s largest organ, serves a vital role in the body’s integumentary system, protecting the individual from external factors such as bacteria, chemicals, UV rays, etc. [3]. Skin conditions can significantly affect one’s quality of life, self-esteem, and social interactions. Issues like chronic itching, visible lesions, and discomfort can lead to social withdrawal and psychological distress, underscoring the importance of dermatological health [4]. In a study done by Kowalewska and team, it was found that according to patients and nurses of those struggling with skin diseases, that they are not fully able to deal with the disease itself and overall have a negative attitude towards it, causing issues of low self-esteem and confidence [5]. Furthermore, such negative feelings can spiral into more severe mental health issues, potentially exacerbating the symptoms of the skin disease. As the emotional and psychological burden of the condition grows, it may hinder the individual’s ability to manage their overall health, creating a cycle of worsening symptoms and declining mental well-being.
The foundations of psych dermatology
Overview of the mind-skin connection
The mind-skin connection refers to psychodermatology, a complex interplay between psychological well-being and dermatological health. This relationship highlights how emotional and mental states and conditions can exacerbate skin conditions and conversely, how skin issues can impact mental health. Stress, anxiety, and other psychological factors can intensify skin problems like eczema, psoriasis, and acne, while chronic skin conditions can lead to emotional distress, creating a cyclicyclical effect that influences mental and physical health. The term psychodermatology is derived from the merging of two major medical specialities- psychiatry and dermatology [6]. Psychiatry is known as the branch of medicine which focuses on the diagnosis and treatment of mental, emotional, and behavioral disorders such as depression, obsessive-compulsive disorder (OCD), bipolar disorder, etc. that are internally developed [7,8]. Dermatology is a medical discipline that deals with the diagnosis and the treatment of diseases regarding skin, nails, and hair such as skin cancer, warts, skin infections, etc. that are manifested externally [9]. Such connections within medicine should be made aware to a practicing dermatologist in order to make well-informed diagnosis and treatment plans [10].
The history of psych dermatology
The history of psych dermatology is quite old, dating back to around 640-377 BC with Hippocrates mentioning the relationship between stress and the effects it has on the skin. Aristotle (384-322 BC) also mentioned a fact similar, believing that the mind and body were complementary and had an effect on each other [10]. The first known psycho-dermatological case vignette was from 1155 AD. In Persia, the prince had been known to have developed psoriasis due to anxiety stemming from the succession of the royal throne. The one suggested to have healed him utilizing what we call psychodynamic psychotherapy, had understood and noted the dynamic relationship between the presence of psoriasis within the patient and the mental conflicts they were facing [11]. Historical cases of trichotillomania, a hair-pulling disorder that may stem from OCD, was seen in the bible (done out of anger, frustration, and as punishment, manifesting negative emotions [12]. Within the 19th century, there was more interest regarding such ideas with the field of psychiatry emerging along with the understanding of a more scientific understanding and approach concerning the mind’s influence on the body. With such influential and known psychiatrists such as Sigmund Freud and his colleagues and Pierre Janet, who studied and argued that such unconscious mental processes and illnesses could manifest themselves into physical symptoms, there was more insight into such topics [13]. The concept of “somatization” emerged from such early ideas, where psychological distress is expressed and manifested through physical symptoms, including those that affect the skin. Such a concept is crucial in understanding how conditions such as dermatitis, hives, and other skin issues may have a psychological component, leading the way for the development of ‘psych dermatology’. This period marked a shift from speculative ideas to more scientific inquiry, as case histories and systematic studies began to document the impact of emotional and mental states on physical well-being. These developments laid the groundwork for the eventual emergence of psych dermatology as a recognized field. In the early 20th century, the field of psych dermatology began to gain traction, particularly in Europe, where medical professionals were increasingly recognizing the intricate relationship between the mind and the skin. Meanwhile, in the United States, the field was still in its formative stages, with a few pioneers beginning to explore these connections [14]. During this period, dermatologists and psychiatrists started collaborating more closely, laying the groundwork for the eventual development of psychodermatology as a distinct discipline. As the century progressed, the development of World War II helped progress the field tremendously. The psychological stress that was experienced by soldiers and those in the face of war had led to a noticeable increase in stress-related skin conditions, which led to most study into the topic. This period saw the emergence of eczematous conditions and psoriasis [15]. Although such flare ups could have been through a contact basis due to the rough environments during war, it was found that around 37% of the patients experiencing psoriasis flare ups was due to the psychological stress they were experiencing [16]. Such information helped further solidify the relationship between dermatology and psychology. In the late 20th and early 21st centuries, psychodermatology continued to expand globally, with increasing recognition in Asia, Latin America, and Africa [17]. The establishment of specialized associations and research centers in countries like Brazil, Japan, and South Africa underscored the growing importance of this interdisciplinary field. These developments were bolstered by advances in neuroscience, which provided a deeper understanding of the neurochemical pathways that link the brain and the skin, offering new insights into how psychological interventions could be used to treat dermatological conditions. Today, psych dermatology is recognized as an essential component of both dermatological and psychiatric care, with ongoing research exploring new therapies and approaches to managing the complex interplay between the mind and the skin.
Overview of inflammatory skin conditions acne
(https://www.niams.nih.gov/health-topics/acne) Acne is a well-known condition involving sebum or oil that clogs the hair follicles under the skin. The skin cells, keratinocytes, which line the follicle normally will rise to the surface of the skin when the skin sheds, however within individuals with acne, these cells along with hair and sebum, get trapped inside the pore. This prevents them from shedding and hinders sebum’s ability to reach the skin’s surface. Combining the cells and the oils promotes the growth of the bacteria that normally lives on the skin. Such growth increases inflammation, heat, redness, swelling and pain. The wall of the clogged follicle will eventually break down and the mixture of bacteria, skin cells and oils will create pimples or lesions [18]. The risk of developing acne may be increased by androgens (male sex hormones) or cortisol. An increased level of androgens or hypersensitivity of the sebaceous glands to normal levels of androgens will increase sebum production [19]. Due to the presence of androgen receptors and enzymes near the part of the follicle where clogging occurs, they may contribute to acne lesions. Hypersensitivity of sebaceous glands to even normal levels of androgens may contribute to acne lesions, particularly in individuals predisposed to the condition [20]. High cortisol also reduces collagen production and skin cell regeneration (as skin fibroblast activity is reduced), hence making it difficult for the skin to heal, making acne lesions last longer than typical. Chronic stress promotes systemic inflammation by increasing the release of pro-inflammatory cytokines such as interleukin-6 (IL-6) and tumor necrosis factor-alpha (TNF-α). These cytokines exacerbate the inflammatory response within hair follicles, contributing to acne pathogenesis. Moreover, stress impairs the skin barrier function, making it more susceptible to irritation and microbial colonization [21]. However, this is not a one way street. Like other stressors, having a skin condition such as acne can directly contribute to increased stress levels, hence creating a vicious cycle. There is a positive correlation between stress and acne severity as well [22].
Eczema
Eczema, also known as Atopic Dermatitis, results in dry, irritated and inflamed skin that causes itchiness and discomfort for patients [23]. Though it is most common in younger children, individuals may have symptoms into adulthood or manifest in adulthood. Individuals with eczema often have other conditions such as asthma, allergies, depression, anxiety, or sleep loss [24]. The factors that may further the condition can be categorized as genetics, the immune system and the environment. Genetic variations affecting the skin proteins, such as those responsible for maintaining the skin’s barrier function, play a role in the progression of the condition. Hyperactivity or inefficiency of the immune system may further the inflammation of the skin and worsen the condition [24]. In addition to these factors, environmental factors such as pollutants, allergens, or fragrances, can compromise the skin barrier, leading to more moisture to escape the skin can contribute to the manifestation of eczema within the individual. These external irritants often heighten the condition by triggering inflammatory responses and impairing the skin’s ability to retain hydration [23]. One major trigger to eczema flare ups is stress, being noted as the single biggest trigger in a NES 2020 patient survey, affecting significantly more women (57%) than men (41%). Stress not only worsens existing symptoms, but also creates a negative feedback loop, where the irritation and discomfort from the skin condition can amplify stress levels, hence contributing to the cycle. With the skin’s heightened sensitivity under stress, it makes it more reactive to other environmental irritants such as allergens and pollutants [25].
Psoriasis
Psoriasis is a chronic condition involving scaly and inflamed patches of skin as a result of an overactive immune system [26]. As the immune system is overactive, it causes skin cells to multiply too quickly. The cause of the condition is still unknown but those with the condition are at greater risk of developing psoriatic arthritis, cardiovascular issues, mental health conditions (such as low self-esteem, anxiety, and depression) and other metabolic conditions including diabetes, obesity or kidney or liver disease. There are various triggers for psoriasis but stress is one of the most common with 31-88% of cases where patients report stress being a trigger for their flare-up [27]. It is also noted that this stress can be furthered as a consequence of the psoriasis flare-up, hence, becoming an endless loop.
Prominent mental health conditions and their dermatological impact
Common mental health conditions
Mental health conditions can be split into multiple different groups based on the Diagnostic and Statistical Manual of Mental Illnesses (DSM-5). The manual, written by the American Psychiatric Association (APA), has multiple sections, with specifically section II focusing on diagnostic criteria and codes, highlighting around 22 different categories into which known mental illness may fall into [28]. A couple of the most common disorders that may be seen, especially in adults (18 and older) are depression (and its subcategories) and anxiety disorders (and its subcategories) [29]. Although those may be the most common disorders, it is important to note that the effects of disorders are detrimental to the health of the individual, therefore, affecting their skin health.
Mood disorders
Mood disorders are characterized as a mental health condition that causes severe changes within an individual’s emotional state. The changes can be noted by long periods of sadness, depression, even excessive happiness or mania, etc. These symptoms must be present for a longer period of time (several weeks or longer). These mood disorders include depressive disorders, bipolar disorders, disruptive mood dysregulation disorder, and premenstrual dysphoric disorder [30] (https://www.ncbi.nlm.nih.gov/books/NBK558911/#:~:text=These%20include%20bipolar%20dis order%2C%20cyclothymia,increase%20in%20morbidity%20and%20mortality).
Depressive disorders: Major depressive disorder (MDD) MDD causes the persistent feeling of sadness and loss of interest. This affects how the individual thinks, feels, and behaves. The amount of episodes of depression an individual falls into depends, but during the episodes there can be feelings of sadness, frustration, loss of interest in most or all activities, lack of sleep, reduced appetite and many more. Increased cortisol levels associated with MDD reduce skin cell regeneration and impairing repair- often exacerbating inflammatory skin conditions like acne and psoriasis. Additionally, depressed levels of serotonin in individuals with MDD may contribute to skin hypersensitivity and delayed wound healing [31].
Persistent depressive disorder (PDD): PDD is a long-term form of depression characterized by a constantly depressed mood, in addition to having poor appetite, insomnia, low energy or fatigue, poor concentration or feelings of hopelessness. A definite diagnosis can only be made if the individual has never had a manic episode, mixed episode, hypomanic episode or symptoms similar to cyclothymia [31]. Chronic stress from PDD weakens the immune system and skin barrier, making individuals more prone to flare-ups of conditions like eczema flare-ups [32]. Premenstrual Dysphoric Disorder (PMDD): PMDD includes symptoms such as mood swings, anger/increased irritability, anxiety and depression and suicidal thoughts [33]. It is known that women experience hormonal changes of progesterone and estrogen up to two weeks. In order to have a definite diagnosis, the individual must experience at least five symptoms in the majority of their menstrual cycles in the final week before the menses onset. These symptoms must not be attributable to any substance or other medical condition [34]. Hormonal changes involving progesterone and estrogen during the menstrual cycle can heighten skin sensitivity and trigger inflammatory responses, exacerbating acne and other inflammatory skin conditions.
Bipolar disorders: Bipolar disorder is considered a mental disorder separate from depressive disorders. Bipolar disorders are characterized by extreme shifts in mood, energy, activity and concentration [35]. These mood episodes influence hormone level, affecting skin health in multiple ways.
Bipolar I disorder: Bipolar I disorder involves manic episodes with abnormal, elevated moods that last at least 1 week for a majority of the day. During this time the patient experiences, inflated self-esteem, decreased sleep, increased talking, racing thoughts, increase in goal-directed activity and excessive involvement in dangerous activities [36].
Bipolar II disorder: Bipolar II disorder involves at least one hypomanic episode (not manic episode) and at least one major depressive episode separate from symptoms that may characterize other psychotic disorders. The symptoms of said depres depression or the alteration of periods of depression and hypomania causes clinically significant distress to the individual within important areas of functioning [36]. Studies have shown that the manic episodes are associated with higher testosterone levels and depressive episodes involve lower testosterone levels. Mood episodes in men aged 45 or older had alterations in gonadal hormones such as testosterone, estradiol and progesterone, as well as, ACTH, cortisol and C-reactive protein [37]. Hormonal changes during mood episodes can impact sebaceous gland activity, leading to increased oil production and acne. Additionally, chronic cortisol elevation during stress phases can weaken skin barrier integrity [38,39].
Anxiety disorders
Anxiety disorders involve heightened cortisol and adrenaline production due to chronic stress, which affects the immune system and skin repair mechanisms [40]. Common anxiety disorders include:
Generalized anxiety disorder: Generalized anxiety disorders (GAD) involves a recurring feeling of anxiety for extended periods such as months. GAD may hinder daily activities by increasing restlessness, fatigue, irritability, unexplained pains, and sleep problems [41].
Panic disorder: Individuals with Panic disorder often experience frequent unexpected “attacks” of intense fear, discomfort, or loss of control without a recognizable danger [41].
Social anxiety disorder: Social anxiety disorder involves anxiety that heightens seemingly beyond control in social situations. Individuals may experience sweating, fast heart rate, body rigidness, and feelings of self-consciousness [41].
Phobia-related disorders: Phobia-related disorders involve an out-of-proportion rise in anxiety in response to certain situations or objects. Such phobias may be heights, blood-related procedures, or certain animals [41]. All of these disorders can impair the skin’s ability to repair itself and maintain hydration, increasing susceptibility to conditions like eczema and psoriasis [42].
Overview of hormonal and neurotransmitter impacts
Dopamine
Dopamine is a neurotransmitter that also acts as a hormone that typically increases in response to rewards and a variety of strongly addictive drugs [43]. Its function is essential to motor control function and promote motivation based on feelings of pleasure [44,45]. If the brain decides that an action or behavior is beneficial then dopamine release is triggered. Despite dopamine being viewed as a good hormone, imbalances may result in further health issues. Increased dopamine levels may cause impulse control issues, hyper-competitiveness or increased aggression [46]. In the context of mood disorders, dopamine’s role is multifaceted. In depression, reduced dopamine transmission is often associated with anhedonia, the inability to feel pleasure. This loss of interest and motivation is a hallmark symptom of depressive episodes [47]. Additionally, dopamine dysregulation is implicated in bipolar disorder, where the highs of mania are associated with increased dopamine activity, while the lows of depression correspond to decreased dopamine signaling. Such dysregulation of dopamine can contribute to behaviors such as skin-picking, induce psoriasis, and influence stress-related HPA axis activity, discussed later [47].
Serotonin
The neurotransmitter plays a pivotal role in stabilizing mood and preventing extreme emotional fluctuations that are associated with mood disorders [48]. Low levels of serotonin can and have been linked with emotional disorders such as depression, anxiety, and OCD [49]. To combat such disorders, the development of selective serotonin reuptake inhibitors (SSRIs) was set into play. SSRIs are a class of antidepressants that work to increase the availability of serotonin within the synaptic cleft, thereby enhancing its mood-stabilizing effects [49]. Serotonin also impacts various physiological processes, including sleep, appetite, and digestion. It is synthesized in the brain and the gastrointestinal tract, with about 90% of the body’s serotonin found in the gut. Serotonin influences inflammatory responses and plays a role in gut health, affecting conditions such as irritable bowel syndrome (IBS) [50]. Low levels of serotonin are now noted to have a significant role within eczema and other ‘itch’ conditions such as psoriasis [48].
Adrenaline (Epinephrine)
Adrenaline, also known as epinephrine, is another key hormone that is involved in the body’s stress response. This hormone, produced by the adrenal medulla, prepares the body for immediate action by increasing heart rate, dilating airways, and boosting energy [51]. However, chronic stress and repeated surges of adrenaline can lead to cardiovascular strain, anxiety disorders, and long-term negative effects on metabolic health. In terms of skin, adrenaline was found to delay early-stage wound healing by activating “ß-ARs in skin cells” as well as promote growth of unwanted bacteria on the skin surface and near skin injuries [52].
Cortisol
Cortisol is a steroid hormone that is released into the bloodstream by the adrenal gland in response to stress. It is essential to the “fight or flight” response that may increase glucose metabolism, control blood pressure, and reduce inflammation [53]. Cortisol is considered a potent anti-inflammatory important in mobilizing glucose reserves for energy and control of inflammation. The symptoms of elevated levels of cortisol include weight gain, acne, fragile skin, hirsutism, and menstrual health irregularities. Low levels of cortisol can cause nausea, weight loss, fatigue, and abdominal pain [54]. Such irregular levels of cortisol can lead to conditions such as anxiety, depression, and metabolic disorders. Cortisol has one of the most profound effects on skin conditions regarding sebum production, skin integrity, and skin appearance [41].
Production and regulation of related hormones
The stress response system (HPA axis)
The hypothalamic-pituitary-adrenal (HPA) axis is the central response system in the body, which hence, plays a crucial role in the production and regulation of stress-related hormones [56]. It consists of the hypothalamus, the anterior pituitary gland, and the adrenal glands (adrenal cortex). The hypothalamus is essentially keeping the body in a state of equilibrium regarding body temperature, state of hunger, mood, etc by having an influence of the autonomic nervous system [56]. The pituitary gland is oftentimes stated as the master gland. Although its small size, it makes a key difference regarding the production of essential hormones. The adrenal glands are fairly small, sitting on the top of each kidney. They produce certain hormones that assist in this axis.
How does the HPA axis Work?
When an individual undergoes an event that induces stress, the autonomic nervous system triggers the individual’s hypothalamus, inducing it to release corticotropin-releasing hormone. When the release of this hormone, it signals to the anterior pituitary gland to secrete adrenocorticotropic hormone (ACTH) [57]. The ACTH then triggers the adrenal glands to release cortisol which is the primary stress hormone. Cortisol is the main hormone that corresponds with stress- vital for managing stress and maintaining the body’s homeostasis. This reaction acts in what is considered a negative feedback loop [56], where the resulting cortisol hormones signal the hypothalamus to reduce/stop the production of CRH. However, if such events are occurring often within an individual, it can create dysfunction within the HPA axis.
The cortisol pathway for skin conditions
Cortisol, a hormone produced by the adrenal glands in response to adrenocorticotropic hormone (ACTH), exerts its effects throughout the body by binding to glucocorticoid receptors (GR) present in various tissues, including keratinocytes in the skin. These receptors regulate the expression of glucocorticoid-responsive genes, playing a key role in skin homeostasis [57]. While short-term elevations in glucocorticoids can reduce inflammation and support skin cell turnover, chronic overexposure, as observed in conditions like Cushing’s Syndrome, may overstimulate GR [58]. This dysregulation compromises the skin’s immune defenses, impairs its repair mechanisms, and leads to thinning and increased fragility of the skin. The overstimulation of GR can affect various pathways such as the extracellular matrices, the genes that affect collagen and elastin development etc. The key genes that are affected are FKBP5 and GILZ which are upregulated, contributing to fibroblast dysfunction [59]. Genes such as COL1A1 and COL3A1 are downregulated, reducing collagen production [60].
Neurotransmitter pathways
Neurotransmitters are essential chemical messengers that transmit signals across synapses between neurons, playing a critical role in regulating a wide array of physiological and psychological processes. These neurotransmitters operate through specific pathways in the brain, each with distinct functions that are crucial for maintaining mental health and emotional stability. [70].
Dopamine pathway for skin conditions
Dopamine is a critical neurotransmitter that is primarily associated with the brain’s ‘reward’ system. It is produced in several brain regions, including the substantia nigra, which is involved in motor control, the ventral tegmental area (VTA), which plays a key role in reward and motivation [71].
There are 5 types of dopamine receptors, which include D1, D2, D3, D4 , and D5 of which D1 receptors (via nerve endings) are found within the dermis of the skin, the lower epidermal layers, and the subcutaneous tissue [72]. Dopamine itself is secreted into keratinocytes within the skin layers. These keratinocytes have the capability to produce dopamine by synthesizing L-DOPA [72]. In skin conditions such as psoriasis, there is increased keratinocytes.
Therefore, those with psoriasis have high dopamine levels. Such elevated levels of dopamine within the skin can cause T-cell activation hence creating cell mediated immunity that ultimately leads to infection or disease. Such high levels have also been associated with vitiligo, where such high levels of dopamine are lethal to melanocytes within the skin [72].
Research suggests that the D1 and D2 receptors exhibit a maintaining effect of the HPA axis even after the stressor has passed [73]. The longer the stress levels, the greater the potential for pathological (harmful) effects on the body. The long-term or excessive activation of the HPA axis (keeping glucocorticoid levels high for an extended period) can lead to negative health effects, such as chronic stress, immune suppression, or other stress-related disorders [74].
The serotonin pathway for skin conditions
The serotonin pathway is one of the most well-studied neurotransmitter systems, which contributes to mood regulation and emotional well-being. It is most commonly known for its effect on the mood but it plays a crucial role in an individual’s memory, fear, appetite, and stress [54]. Serotonin is synthesized from the amino acid tryptophan through the process of hydroxylation to 5-hydroxy-L-tryptophan (5-HTP) and decarboxylation to 5-hydroxytryptamine (5-HT) and is predominantly produced in the brainstem’s raphe nuclei and in the gastrointestinal tract. Once released, serotonin binds to various receptors in the brain, influencing mood, sleep, appetite, and social behavior [75].
There are several serotonin receptors that are found throughout the skin including 5-HT1A and HTR7 that contribute to ‘itch disorders’ such as eczema and psoriasis. In research done by those at Buck Institute for Research on Aging and University of California, Berkley have discovered that the serotonin receptor HTR7 was a key activator of the ion channel TRPA1, hence, triggering itching behavior linked with skin conditions like eczema and atopic dermatitis [76].
Adrenaline (Epinephrine) pathway
Adrenaline (epinephrine), is a key hormone within the sympathetic-adrenal-medullary axis (SAM axis), that plays a significant role in the body’s stress response and thus, exerts effects on the skin. With the activation of the SAM axis, adrenaline is released into circulation, where it interacts with adrenergic receptors within the skin, including keratinocytes, hence affecting fibroblast proliferation and its ability to form connective tissue- important within wound healing and maintaining the structure of tissues [42]. Such stress-induced epinephrine can compromise the dermal fibroblasts through the β-adrenoceptor which was seen in the activity of neonatal mouse skin fibroblasts [77].
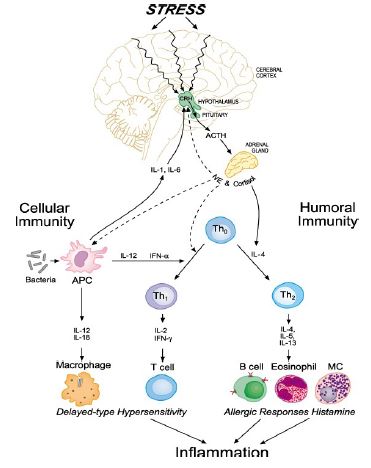
Table 1: Highlights the cytokine effect based on each hormone and its respective cutaneous manifestation [21].
| Hormone | Effects oncytokine production | Impact on skin conditions |
|---|---|---|
| Cortisol | Suppresses IL-1, IL-6, andTNF-α; Reduces inflammation; Chronicexposure can impair immunefunction | Impaired wound healing, increased susceptibility toinfections, contributes topsoriasis and atopic dermatitis |
| Dopamine | Increases IL-6 and TNF-α, promoting inflammation; Regulates IL-10, influencing immune suppression | Elevated levels exacerbate psoriasis, contributeto vitiligo and other autoimmune skinconditions |
| Serotonin | Activates HTR7, increasing IL-1β and IL-6; Affects mastcells, triggering inflammatoryresponses | Contributes to eczema,psoriasis, anditch disorders |
| Adrena- line | Suppresses IL-1 andTNF-α initially; PromotesIL-10; Chronic elevation impairs immunedefense | Delayed wound healing, increased skin fragility |
Inflammatory cytokines: All mentioned hormones also have the ability to modulate the levels of pro- and anti-inflammatory cytokines within the individual’s immune system, furthering the cutaneous manifestations of the mental health conditions the hormones contribute to. They may be produced as part of a cascade [79,78].
Cytokine imbalances and skin disorders
a. Psoriasis: Elevated IL-6 and TNF-α drive chronic inflammation and excessive keratinocyte proliferation [79, 78]
b. Atopic dermatitis: Increased IL-4 and IL-13 contribute to immune dysregulation and barrier dysfunction [80].
c. Acne vulgaris: IL-1β and TNF-α promote inflammation in sebaceous glands [81].
Integrative approaches to treatment
Holistic and multidisciplinary approaches: Combining dermatological and psychological care, A multidisciplinary approach that integrates dermatological and psychological care is essential for individuals whose skin conditions are exacerbated by mental health issues. Treating only the skin condition may temporarily improve self-esteem and reduce symptoms, but without addressing the underlying psychological factors, the individual remains vulnerable to ongoing stress and potential flare-ups. By incorporating mental health support alongside dermatological treatment, patients can achieve more sustainable improvements in both skin health and overall well-being. This incorporation of the two fields can be seen in approaches such as psychodermatology, dietary and lifestyle interventions, support groups, etc.
Role of psychodermatology clinics
Psychodermatology clinics offer essential care for patients dealing with both dermatological and psychological conditions, streamlining treatment by eliminating the need for multiple appointments and preventing conflicting treatment plans from separate practitioners. A study by Seale et al. proposes the establishment of such a clinic within Detroit’s major health system. Their findings emphasize that all referred patients successfully received comprehensive care tailored to their overlapping medical needs. The role of these clinics are crucial to providing the most efficient and effective care for patients [82].
Stress management techniques
Cognitive-behavioral therapy (CBT)
As the name suggests, cognitive behavioral therapy is a combination of cognitive and behavioural therapy methods. Cognitive therapy encourages the client to have a better understanding of their own thoughts, attitudes and expectations. Any negative habits or thought patterns would be replaced with less harmful and more realistic thoughts. Behavioral therapy analyzes behavioral patterns and categorizes them as beneficial or hindering. Then actions will be taken to alter behaviors and make an individual more productive or at ease such as what is done in anxiety disorders. Cognitive Behavioral therapy is now commonly used for conditions such as anxiety, depression, or obsessive-compulsive disorder. In order for the therapy to be effective the patient needs to be actively involved. The therapist and the patient would go through determining a patient’s problems and outlining what the patients’ goals are and then incorporate relaxation exercises or stress-reducing/ pain-relieving techniques. This is considered a short-term treatment due to individuals reporting feeling better after only a few months [83]. Such therapy has been used to treat skin diseases which have been associated with high levels of stress, anxiety and negative feelings. Though it has not been proven that CBT itself has improved skin conditions, it has been found that the combination of CBT and standard medical treatments resulted in greater improvement in physical functioning [84]. The most common skin disorders with treatment involving CBT are acne and skin-picking disorders. CBT would be aimed at increasing patient’s awareness of their negative cognitive distortions that limit treatment adherence. It has been found that CBT was 2.67 times more likely to reduce the clinical severity of lesions from moderate/severe to mild when compared to controls [85].
Mindfulness and meditation practices
Mindfulness-based meditation/ therapy (MBT) practices involve therapeutic approaches within group classes and daily mindfulness exercises that are practiced at home that teaches people to increase their mindfulness through yoga and meditation. It has been found through a systematic review of over 200 MBT studies that MBT is effective for reducing stress, anxiety, and depression [86]. Such use of this form of stress mediation allows for the shifting of emotional regulation and reducing stress, hence, allowing for the decrease of hormonal dysregulation within an affected individual.
Pharmacological interventions
Medications targeting both mental health and skin conditions. Certain antipsychotics have been used to treat both psychological and dermatological conditions. For example, gabapentin which is typically prescribed for burning pain of nerves after shingles, or postherpetic neuralgia and idiopathic trigeminal neuralgia Dermatologically, it can be prescribed for pruritus (itching/irritation) [87]. Topiramate, an antiepileptic medication, may be prescribed to treat individuals diagnosed with dermatillomania (skin picking) in order to reduce the time, they spend picking at their skin thereby reducing scarring [88]. Lamotrigine, also an antiepileptic, has been found to do the same. Another drug is Naltrexone which is a long-lasting opioid antagonist typically prescribed for those who are opioid dependent, and may also be prescribed for pruritus.
Hormonal therapies and their impact on skin
Hormonal therapies are also used to treat skin conditions whether the cause is mental health related or not. These therapies aim to address the hormones that typically exacerbate conditions such as acne. A majority of the hormonal therapies available suppress sources of androgens, block activation or block the actions of androgens in sebaceous glands or follicular keratinocytes. An example of a treatment that has been used to suppress adrenal androgen secretion is the use of glucocorticoids specifically used when a patient experiences an acute acne flare or when the patient has a very severe acne for a few weeks [20].
Preventive strategies and lifestyle modifications
Promoting mental health for skin well-being
Healthy lifestyle choices (diet, exercise, sleep), adopting a healthy lifestyle positively influences every aspect of life, from physical and mental health to emotional resilience and social interactions. Proper nutrition, regular physical activity, and sufficient sleep are foundational elements that enhance immune function, regulate hormonal balance, and reduce systemic inflammation [89]. These factors not only contribute to clear skin and improved dermatological health but also promote cardiovascular health, cognitive function, and emotional stability.
Skin care practices: A consistent and scientifically supported skin care regimen plays a crucial role in managing chronic dermatological conditions. Proper hydration, the use of non-comedogenic products, and barrier repair strategies (such as ceramide-based moisturizers) help maintain skin integrity and prevent exacerbations. Furthermore, avoiding known environmental and behavioral triggers, such as allergens, irritants, and excessive ultraviolet (UV) exposure can reduce the frequency and severity of flare-ups. Personalized dermatological recommendations, in conjunction with psychological support, may provide a more comprehensive approach to managing stress-related skin disorders.
Conclusion
The intricate relationship between mental health and skin conditions, highlights the impact that psychological well-being can have on dermatological health. Stress, anxiety, and other emotional factors can exacerbate or even trigger various skin disorders, highlighting the necessity for a holistic, multifaceted approach to dermatological care. Recognizing this connection is essential for developing effective treatment strategies that address both the mind and the skin for affected individuals. Hormonal fluctuations play a pivotal role in dermatological health, with stress-related increases in cortisol and androgens contributing to inflammatory skin disorders. Elevated cortisol, lowered dopamine, and lowered serotonin levels can weaken the skin barrier by reducing production of essential skin structures such as cortisol or upregulating pro-inflammatory cytokines, making conditions like Additionally, stress-induced androgen surges stimulate sebaceous gland activity, increasing sebum production and inflammation, which can aggravate acne. Understanding the hormonal mechanisms that underlie these conditions is crucial for designing targeted treatment strategies that account for both internal endocrine changes and external skin symptoms. While research has advanced in connecting the mind-skin connection, further investigation is needed to explore the precise molecular pathways through which stress and hormones impact skin health. Examining how chronic psychological stress influences keratinocyte function, immune signaling, and neuroinflammatory pathways could lead to more effective dermatological interventions. Such research is vital for refining treatment approaches that integrate both mental health and skin care. A comprehensive approach that incorporates both dermatological and psychological care is crucial for improving patient outcomes. Dermatologists should consider mental health screenings as part of routine skin assessments, ensuring that stress-related triggers are identified and managed alongside conventional dermatological therapies. Collaborative efforts between dermatologists, endocrinologists, and mental health professionals can enhance treatment efficacy, promoting a more holistic approach to skin health that acknowledges the deep interconnection between the mind and skin.
References
- ADAM Medical Encyclopedia. Johns Creek (GA): Ebix, Inc, ADAM; c1997-2020. Nail abnormalities. 2019; 4. https://medlineplus.gov/ency/imagepages/8912.htm.
- Centers for Disease Control and Prevention. About Mental Health [Internet]. Centers for Disease Control and Prevention. US Department of Health & Human Services. 2024. https://www.cdc.gov/mentalhealth/learn/index.htm.
- Aarons GA, Monn AR, Leslie LK, Garland A, Lugo L, et al. The Association of Mental and Physical Health Problems in High-Risk Adolescents: A Longitudinal Study. The Journal of Adolescent Health: Official Publication of the Society for Adolescent Medicine [Internet]. 2008; 43(3): 260-7. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2768339.
- Tuckman A. The Potential Psychological Impact of Skin CondiConditions. Dermatology and Therapy. 2017; 7(1): 53-7.
- Kowalewska B, Jankowiak B, Krajewska-Kułak E, Khvorik DF, Niczyporuk W. Quality of life in skin diseases as perceived by patients and nurses. Advances in Dermatology and Allergology. 2020; 37(6): 956-61.
- Koo J. Psychodermatology: A practical manual for clinicians. Current Problems in Dermatology. 1995; 7(6): 204-32.
- American Psychiatric Association. Patients & Families [Internet]. Psychiatry.org. 2019. https://www.psychiatry.org/patients-families.
- Medline Plus. Mental Disorders [Internet]. Medlineplus.gov. National Library of Medicine; 2021. https://medlineplus.gov/mentaldisorders.html.
- Ferreira IG, Weber MB, Bonamigo RR. History of dermatology: the study of skin diseases over the centuries. Anais Brasileiros de Dermatologia [Internet]. 2021; 96(3): 332-45. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8178570/.
- França K, Chacon A, Ledon J, Savas J, Nouri K. Pyschodermatology: A trip through history. Anais Brasileiros de Dermatologia [Internet]. 2013; 88(5): 842-3. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3798372/.
- Shafi M. Exploratory Psychotherapy in the Treatment of Psoriasis. Archives of General Psychiatry. 1979; 36(11): 1242.
- Yasuhisa P. “Trachta’ll” in the Testaments. International journal of trichology [Internet]. 2015; 7(2): 47-7.
- Gottlieb RM. Psychosomatic Medicine: The Divergent Legacies of Freud and Janet. Journal of the American Psychoanalytic Association. 2003; 51(3): 857-81.
- Minoli RN. Psych dermatology: An Overview of History, Concept, Classification, and Current Status [Internet]. www.ijiapp.com. 2020. https://www.ijiapp.com/abstractArticleContentBrowse/IJPP/24618/JPJ/fullText
- Gelman AB, Norton SA, Valdes-Rodriguez R, Yosipovitch G. A Review of Skin Conditions in Modern Warfare and Peacekeeping Operations. Military Medicine. 2015; 180(1): 32-7.
- Griffiths CEM, Richards HL. Psychological influences in psoriasis. Clinical and Experimental Dermatology. 2001; 26(4): 338-42.
- Rodríguez-Cerdeira C, Telmo Pera-Grasa J, Isa-Isa R, Arenas-Guzmán R. Psychodermatology: Past, Present and Future. The Open Dermatology Journal [Internet]. 2011; 5: 21-7. https://opendermatologyjournal.com/contents/volumes/V5/TODJ-5-21/TODJ-5-21.pdf.
- Garrick N. Acne [Internet]. National Institute of Arthritis and Musculoskeletal and Skin Diseases. 2016. https://www.niams.nih.gov/health-topics/acne.
- Horszowski D, Niedzielska M, Kozłowski M, Brodowska A, Przepiera A, et al. Evaluation of Hormonal Factors in Acne Vulgaris and the Course of Acne Vulgaris Treatment with Contraceptive-Based Therapies in Young Adult Women. Cells. 2022; 11(24): 4078.
- Ghosh S, Jain V, Aggarwal K, Chaudhuri S. Profiling and hormonal therapy for acne in women. Indian Journal of Dermatology. 2014; 59(2): 107.
- Zhang H, Wang M, Zhao X, Wang Y, Chen X, et al. Role of stress in skin diseases: A neuroendocrine-immune interaction view. Brain, Behavior, and Immunity. 2024; 116: 286-302.
- Zari S, AL Rahmani D. The association between stress and acne among female medical students in Jeddah, Saudi Arabia. Clinical, Cosmetic and Investigational Dermatology. 2017; 10(1): 503-6.
- Mayo Clinic. Atopic dermatitis (eczema) - Symptoms and causes [Internet]. Atopic dermatitis (eczema). Mayo Clinic. 2023. https://www.mayoclinic.org/diseases-conditions/atopic-dermatitis-eczema/symptoms-causes/syc20353273.
- NIAMS. Atopic Dermatitis [Internet]. National Institute of Arthritis and Musculoskeletal and Skin Diseases. 2017. https://www.niams.nih.gov/health-topics/atopic-dermatitis%20%20.
- Lambert A. Stress and eczema [Internet]. National Eczema Society. 2021. https://eczema.org/information-and-advice/triggers-for-eczema/stress-and-eczema/.
- NIAMS. Psoriasis [Internet]. National Institute of Arthritis and Musculoskeletal and Skin Diseases. 2017. https://www.niams.nih.gov/health-topics/psoriasis%20%20.
- Rousset L, Halioua B. Stress and psoriasis. International Journal of Dermatology. 2018; 57(10): 1165-72.
- American Psychiatric Association. Section I: DSM-5 Basics Introduction Use of the Manual Cautionary Statement for Forensic Use of DSM-5 [Internet]. 2013. https://www.psychiatry.org/File%20Library/Psychiatrists/Practice/DSM/APA_DSM-5-Contents. Pdf.
- National Collaborating Centre for Mental Health (UK). COMMON MENTAL HEALTH DISORDERS [Internet]. Nih.gov. British Psychological Society; 2011. https://www.ncbi.nlm.nih.gov/books/NBK92254/.
- Cleveland Clinic. Mood Disorders [Internet]. Cleveland Clinic. 2018. https://my.clevelandclinic.org/health/diseases/17843-mood-disorders.
- Mayo Clinic. Depression (Major Depressive Disorder) [Internet]. Mayo Clinic. Mayo Foundation for Medical Education and Research; 2022. https://www.mayoclinic.org/diseases-conditions/depression/symptoms-causes/syc-20356007 31.
- Substance Abuse and Mental Health Services Administration. Table 3.5, DSM-IV to DSM-5 Dysthymic Disorder Comparison [Internet]. Nih.gov. Substance Abuse and Mental Health Services Administration (US); 2016. https://www.ncbi.nlm.nih.gov/books/NBK519704/table/ch3.t6/
- Mayo Clinic. Persistent depressive disorder (dysthymia) - Symptoms and causes [Internet]. Mayo Clinic. Mayo clinic. 2022. https://www.mayoclinic.org/diseases-conditions/persistent-depressive-disorder/symptoms-causes /syc-20350929.
- Landén M, Eriksson E. How does premenstrual dysphoric disorder relate to depression and anxiety disorders? Depression and Anxiety. 2003; 17(3): 122-9.
- National Institute of Mental Health. Bipolar Disorder [Internet]. National Institute of Mental Health. 2024. https://www.nimh.nih.gov/health/topics/bipolar-disorder.
- Florida BH Center. DSM-5 criteria: Bipolar disorders [Internet]. 2019. https://floridabhcenter.org/wp-content/uploads/2021/02/Bipolar-Disorders_Adult-Guidelines-201 9-2020.pdf.
- Lyu N, Zhao Q, Fu B, Li J, Wang H, et al. Hormonal and inflammatory signatures of different mood episodes in bipolar disorder: A large-scale clinical study. BMC Psychiatry. 2023; 23(1).
- Sher L, Greenbaum MF, Sullivan GM, Burke AK, Cooper TB, et al. Testosterone levels in suicide attempters with bipolar disorder. Journal of Psychiatric Research [Internet]. 2012; 46(10): 1267-71. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3810946/.
- Maroufi M, Mousavizadegan S. Comparison of salivary testosterone levels in different phases of bipolar I disorder and control group. Journal of Research in Medical Sciences. 2018; 23(1): 31.
- NIMH. Anxiety disorders [Internet]. National Institute of Mental Health. 2024. https://www.nimh.nih.gov/health/topics/anxiety-disorders
- Substance Abuse and Mental Health Services Administration. Table 3.15, DSM-IV to DSM-5 Generalized Anxiety Disorder Comparison [Internet]. National Library of Medicine. Substance Abuse and Mental Health Services Administration (US). 2016. https://www.ncbi.nlm.nih.gov/books/NBK519704/table/ch3.t15/.
- Chen Y, Lyga J. Brain-Skin Connection: Stress, Inflammation and Skin Aging. Inflammation & Allergy-Drug Targets [Internet]. 2014; 13(3): 177-90. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4082169/.
- Juárez Olguín H, Calderón Guzmán D, Hernández García E, Barragán Mejía G. The role of dopamine and its dysfunction as a consequence of oxidative stress. Oxidative Medicine and Cellular Longevity [Internet]. 2015; 2016(1): 1-13. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4684895/.
- Ko JH, Strafella AP. Dopaminergic Neurotransmission in the Human Brain: New Lessons from Perturbation and Imaging. The Neuroscientist: A review journal bringing neurobiology, neurology and psychiatry [Internet]. 2012; 18(2): 149-68. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3479149/.
- Berridge Kent C, Kringelbach Morten L. Pleasure Systems in the Brain. Neuron [Internet]. 2015; 86(3): 646-64. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4425246/.
- Seo D, Patrick CJ, Kennealy PJ. Role of serotonin and dopamine system interactions in the neurobiology of impulsive aggression and its comorbidity with other clinical disorders. Aggression and Violent Behavior [Internet]. 2008; 13(5): 383-95. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2612120/.
- Wardhana M, Windari M, Puspasari N, Suryawati N. Role of Serotonin and Dopamine in Psoriasis: A Case-Control Study. Open Access Macedonian Journal of Medical Sciences [Internet]. 2019; 7(7): 1138-42. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6490488/.
- Bamalan OA, Al Khalili Y. Physiology, Serotonin [Internet]. PubMed. Treasure Island (FL): StatPearls Publishing. 2023. https://www.ncbi.nlm.nih.gov/books/NBK545168/.
- Villines Z. Serotonin deficiency: Symptoms, treatments, causes, and more [Internet]. www.medicalnewstoday.com. 2020. https://www.medicalnewstoday.com/articles/serotonin-deficiency.
- Strandwitz P. Neurotransmitter Modulation by the Gut Microbiota. Brain research. 2018; 1693(Pt B): 128-33.
- LeWine HE. Understanding the stress response [Internet]. Harvard Health. 2024. https://www.health.harvard.edu/staying-healthy/understanding-the-stress-response.
- Luqman A, Götz F. The Ambivalent Role of Skin Microbiota and Adrenaline in Wound Healing and the Interplay between Them. International Journal of Molecular Sciences [Internet]. 2021; 22(9): 4996. https://pubmed.ncbi.nlm.nih.gov/34066786/
- The role of cortisol in the body [Internet]. Healthdirect.gov.au. Healthdirect Australia. 2024. https://www.healthdirect.gov.au/the-role-of-cortisol-in-the-body%20
- Tataranni PA, Larson DE, Snitker S, Young JB, Flatt JP, et al. Effects of glucocorticoids on energy metabolism and food intake in humans. American Journal of Physiology-Endocrinology and Metabolism. 1996; 271(2): 317-25.
- Hannibal KE, Bishop MD. Chronic Stress, Cortisol Dysfunction, and Pain: A Psych neuroendocrine Rationale for Stress Management in Pain Rehabilitation. Physical Therapy [Internet]. 2014; 94(12): 1816-25.
- Zagami M, Klepper E, Wienecke E, Andrzejewski M, Sikder A, et al. A review of psych cutaneous disorders from a psychotherapeutic perspective-Toolkit for the dermatologist. Skin Health and Disease. 2023.
- Cleveland Clinic. HPA Axis: The stress response system [Internet]. Cleveland Clinic. 2024. https://my.clevelandclinic.org/health/body/hypothalamic-pituitary-adrenal-hpa-axis.
- Smith SM, Vale WW. The role of the hypothalamic-pituitary-adrenal axis in neuroendocrine responses to stress. Dialogues in Clinical Neuroscience [Internet]. 2006; 8(4): 383-95. https://pmc.ncbi.nlm.nih.gov/articles/PMC3181830/.
- Tomoshige Kino. Glucocorticoid Receptor [Internet]. Nih.gov. MDText.com, Inc. 2017. https://www.ncbi.nlm.nih.gov/books/NBK279171/.
- Lamberts SWJ. Glucocorticoid receptors and Cushing’s disease. Molecular and Cellular Endocrinology [Internet]. 2002; 197(1-2): 69-72. https://www.sciencedirect.com/science/article/abs/pii/S0303720702002800.
- Lause M, Kamboj A, Fernandez Faith E. Dermatologic manifestations of endocrine disorders. Translational Pediatrics [Internet]. 2017; 6(4): 300-12. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5682371/.
- Leung CS, Kosyk O, Welter EM, Dietrich N, Archer TK, et al. Chronic stress-driven glucocorticoid receptor activation programs key cell phenotypes and functional epigenomic patterns in human fibroblasts. iScience [Internet]. 2022; 25(9): 104960. https://www.sciencedirect.com/science/article/pii/S2589004222012329#sec5.
- Teleanu RI, Niculescu AG, Roza E, Vladâcenco O, Grumezescu AM, et al. Neurotransmitters-Key Factors in Neurological and Neurodegenerative Disorders of the Central Nervous System. International Journal of Molecular Sciences [Internet]. 2022; 23(11): 1-24. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9180936/.
- Ilango A, Kesner AJ, Keller KL, Stuber GD, Bonci A, et al. Similar Roles of Substantia Nigra and Ventral Tegmental Dopamine Neurons in Reward and Aversion. The Journal of Neuroscience. 2014; 34(3): 817-22.
- Tammaro A, Cavallotti C, Gaspari AA, Narcisi A, Parisella FR, et al. Dopaminergic receptors in the human skin. Journal of biological regulators and homeostatic agents [Internet]. 2012; 26(4): 789-95. https://pubmed.ncbi.nlm.nih.gov/23241131/.
- Sreedevi K. Dopamine Dynamics in Dermatology and Behavioural Science. Journal of Addiction Science. 2020; 6(2): 34-6.
- Belda X, Armario A. Dopamine D1 and D2 dopamine receptors regulate immobilization stress-induced activation of the hypothalamus-pituitary-adrenal axis. Psychopharmacology. 2009; 206(3): 355-65.
- Herman JP, McKlveen JM, Ghosal S, Kopp B, Wulsin A, et al. Regulation of the Hypothalamic-Pituitary-Adrenocortical Stress Response. Comprehensive Physiology [Internet]. 2016; 6(2): 603-21. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4867107/
- Bakshi A, Tadi P. Biochemistry, Serotonin [Internet]. PubMed. Treasure Island (FL): StatPearls Publishing; 2022. https://www.ncbi.nlm.nih.gov/books/NBK560856/.
- Morita T, McClain Shannan P, Batia Lyn M, Pellegrino M, Wilson Sarah R, et al. HTR7 Mediates Serotonergic Acute and Chronic Itch. Neuron [Internet]. 2015; 87(1): 124-38. https://www.cell.com/neuron/pdf/S0896-6273(15)00483-3.pdf.
- Romana-Souza B, Otranto M, Almeida TF, Porto LC, Monte-Alto-Costa A. Stress-induced epinephrine levels compromise murine dermal fibroblast activity through β-adrenoceptors. Experimental Dermatology. 2011; 20(5): 413-9.
- Tausk F, Elenkov I, Moynihan J. Psychoneuroimmunology. Dermatologic Therapy. 2008; 21(1): 22-31.
- Condo A. The Role of Cytokines in The Patho mechanism of Cutaneous Disorders. Indian Journal of Dermatology [Internet]. 2012; 57(2): 90-6. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3352652/.
- Zhang JM, An J. Cytokines, Inflammation, and Pain. International Anesthesiology Clinics [Internet]. 2007; 45(2): 27-37. https://pmc.ncbi.nlm.nih.gov/articles/PMC2785020/.
- Zhou X, Chen Y, Cui L, Shi Y, Guo C. Advances in the pathogenesis of psoriasis: from keratinocyte perspective. Cell Death & Disease. 2022; 13(1).
- Pappa G, Sgouros D, Theodoropoulos K, Kanelleas A, Bozi E, et al. The IL-4/-13 Axis and Its Blocking in the Treatment of Atopic Dermatitis. Journal of Clinical Medicine. 2022; 11(19): 5633.
- Cruz SA, Vecerek N, Elbuluk N. Targeting Inflammation in Acne: Current Treatments and Future Prospects. American Journal of Clinical Dermatology. 2023; 24(5): 681-94.
- Seale L, Gaulding JV, Porto D, Prabhakar D, Kerr H. Implementation of a psychodermatology clinic at a major health system in Detroit. International Journal of Women’s Dermatology. 2018; 4(4): 227-9.
- Revankar RR, Revankar NR, Balogh EA, Patel HA, Kaplan SG, et al. Cognitive behavior therapy as dermatological treatment: a narrative review. International Journal of Women’s Dermatology. 2022; 8(4): 068.
- van Beugen S, Ferwerda M, Spillekom-van Koulil S, Smit JV, Zeeuwen-Franssen MEJ, et al. Tailored Therapist-Guided Internet-Based Cognitive Behavioral Treatment for Psoriasis: A Randomized Controlled Trial. Psychotherapy and Psychosomatics [Internet]. 2016; 85(5): 297-307. https://www.karger.com/Article/Pdf/447267.
- Mashayekhi Goyonlo V, Sardabi MS, Tavalaei AM, Khoshnevisan Z, Razmara M. Cognitive behavioral therapy as an adjuvant therapy in acne excoriée: A randomized controlled clinical trial. Journal of Dermatological Treatment. 2020; 1-7.
- Khoury B, Lecomte T, Fortin G, Masse M, Therien P, et al. Mindfulness-based therapy: A comprehensive meta-analysis. Clinical Psychology Review [Internet]. 2013; 33(6): 763-71. https://pubmed.ncbi.nlm.nih.gov/23796855/.
- Scheinfeld N. The role of gabapentin in treating diseases with cutaneous manifestations and pain. International Journal of Dermatology. 2003; 42(6): 491-5.
- Jafferany M, Osuagwu FC. Use of Topiramate in Skin-Picking Disorder. The Primary Care Companion for CNS Disorders. 2017; 19(1).
- Shao T, Verma HK, Pande B, Costanzo V, Ye W, et al. Physical Activity and Nutritional Influence on Immune Function: An Important Strategy to Improve Immunity and Health Status. Frontiers in Physiology. 2021; 12(751374).