
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Bilateral complete duplex system with right intravesical & left extravesical ureteroceles: Case report
Yirgalem Teklebirhan Gebreziher1*; Hadush Tesfay Negash1; Zeamanuel Berihu Teshome2; Seare Halefom Kahsay3
1Department of Pediatric Surgery, Ayder Comprehensive Specialized Hospital, Mekelle University, Ethiopia.
2Department of Radiology, Ayder Comprehensive Specialized Hospital, Mekelle University, Ethiopia.
3Department of Surgery, Ayder Comprehensive Specialized Hospital, Mekelle University, Ethiopia.
*Corresponding Author : Teklebirhan Gebreziher Y
Department of Pediatric Surgery, Ayder Comprehensive Specialized Hospital, Mekelle university, Ethiopia.
Email: yirgalemtek1@gmail.com
Received : Mar 20, 2025
Accepted : Apr 17, 2025
Published : Apr 24, 2025
Archived : www.jcimcr.org
Copyright : © Teklebirhan Gebreziher Y (2025).
Abstract
Introduction: Bilateral duplex system with ureteroceles is one of the rarest entities in urology. Duplex collecting system is a common urologic anomaly with a wide range of clinical symptoms and a variety of associated urologic abnormalities such as an ectopic ureter, ureterocele, vesicoureteral reflux and ureteropelvic junction
Clinical Presentation: We present a 12-year-old male adolescent presented with nocturnal enuresis since birth and right flank pain of 8 months duration. There were no pertinent physical findings. A complete blood count, renal function test, urine analysis, ultrasound of the abdomen and pelvis, computed tomography urography, and cystoscopy were performed. A single-setting right upper pole hemi nephroureterectomy and left ureteropyelostomy were performed. He is now asymptomatic and regularly followed up on an outpatient basis.
Conclusion: This case report describes the presentation, workup, and surgical management of a very rare congenital anomaly.
Keywords: Bilateral; Complete duplex system; Ureteroceles.
Citation: Teklebirhan Gebreziher Y, Tesfay Negash H, Berihu Teshome Z, Halefom Kahsay S. Bilateral complete duplex system with right intravesical & left extravesical ureteroceles: Case report. J Clin Images Med Case Rep. 2025; 6(4): 3567.
Introduction
Background and rationale: Bilateral complete duplication of the ureters is a rare condition. In a study, of 5196 excretory urograms performed on both children and adults, duplex systems were present in 95 (1.8%) patients. The condition was bilateral in only 16 (0.3%) patients while complete duplication was demonstrated in <1/3 of the duplicated systems [1]. We report a case of severe hydronephrosis and ureter ectasis in the upper moiety of bilateral duplex kidney with extravesical ureterocele on the left side and intravesical ureterocele on the right side. To our knowledge, we report the first case of simultaneous bilateral open procedures for a bilateral complete duplex system with right intravesical & left extravesical ureteroceles.
Guidelines: SCARE 2023 paper: This case report has been reported in line with the SCARE Criteria [2].
Patient information
Demographics and presentation: A 12-year-old male adolescent presented with nocturnal enuresis since birth and right flank pain of 8 months duration. Otherwise, no history of fever, burning during micturition and dysuria. He had a normal voiding pattern.
Past medical and surgical history: He had no known history of TB, Hypertension; Diabetes Mellitus. He had no surgical interventions done in the past.

Drug and allergy history: No history of long-term drug intake and no known allergies until date.
Family history: He had no history of similar illness in the family.
Clinical findings: The physical examination was unremarkable.
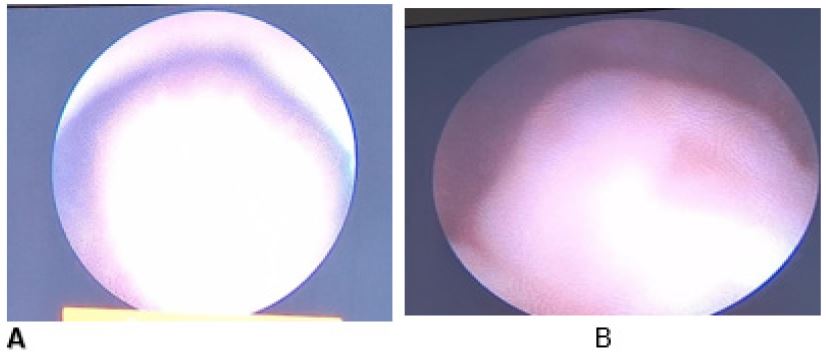
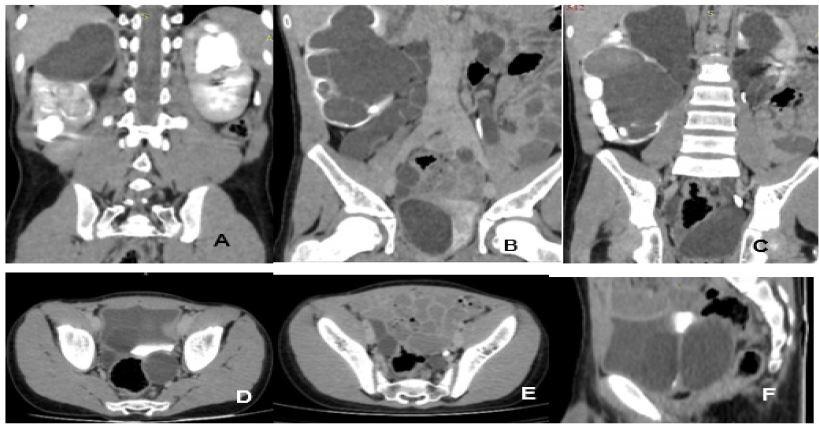
Diagnostic assessment and interpretation: The laboratory investigations of complete blood count, creatinine, urinalysis, including renal function tests, were within normal limits. Ultrasound of the abdomen and pelvis showed on both sides, duplex collecting systems with double ureters were present. There was also right intravesical and left evtravesical ureterocele. Voiding Cystourethrography (VCUG) was performed. It showed a round intravesical-filling defect. Otherwise, there was no Vesicoureteral Reflux (VUR). Cystoscopy was performed later, where a ureterocele located in the prostatic urethra and another intravesical ureterocele were found (Figure 1). A CT IVU showed bilateral complete ureteral duplication. The right upper moiety had severe hydronephrosis and thinned-out, non-excreting parenchyma with hydroureter and intravesical ureterocele. The right lower moiety had moderate hydronephrosis and a dilated normally inserted ureter. The left lower moiety appeared normal with a non-dilated ureter. The left upper moiety had moderate hydronephrosis with a dilated ureter draining below the bladder neck into the prostatic urethra (Figure 2). A renal scan was not performed due to unavailability.
Intervention
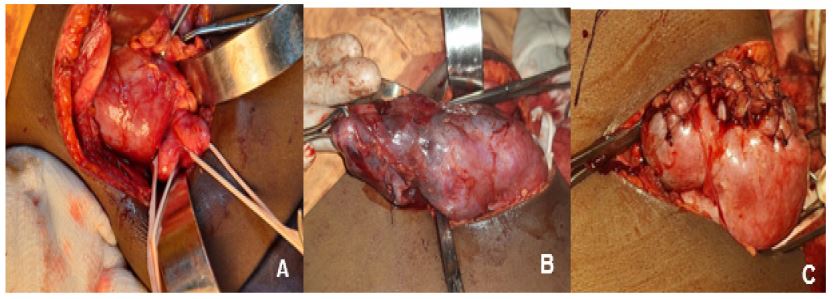
After thorough history and relevant investigations, diagnosis of bilateral complete duplication of ureter with right upper moiety severe hydroureteronephrosis & intravesical ureterocele, and left upper moiety hydroureteronephrosis with extravesical ureterocele was made. The patient was planned for single-setting upper tract procedures, as there was no vesicoureteral reflux (VUR). For the right side, a right hemi nephroureterectomy was planned because the upper moiety in the right kidney was nonfunctional. For the left side, a ureteropyelostomy was planned. Intra operative cystoscopy was performed to stent the lower pole ureters. However, it was difficult to visualize the orifices. On the right side, there was thinned out renal parenchyma with dilated upper moiety and dilated ureters. Right hemi nephroureterectomy was done (Figure 3). Upper moiety ureter was excised as distal as possible.
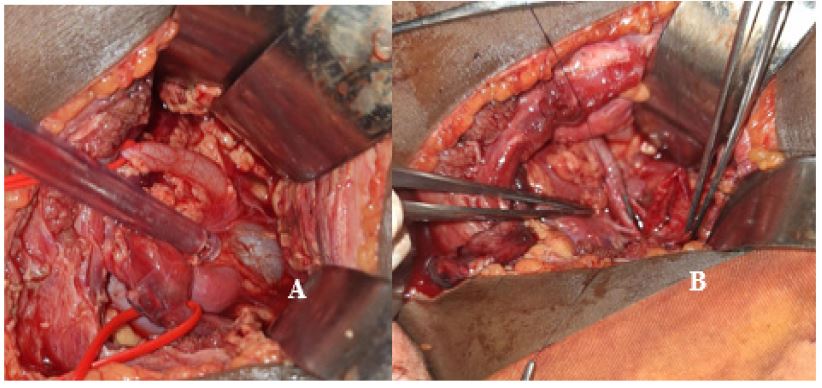
On the left side, the left upper moiety was dilated along with its ureter. The left lower moiety was normal with a non-dilated ureter. Left ureteropyelostomy was done (Figure 4). Upper moiety ureter was excised as distal as possible. For both kidneys, dj stents were inserted intraop antegrade and perinephric drains left in place. The operation was uneventful and blood loss was minimal. The patient was managed with IV fluids, antibiotics, analgesics, antiemetic and antipyretic. Post-operative renal function tests were normal. Drains were removed on the second postoperative day. Postoperative period was uneventful and the patient had recovered well.
Ureteric stents were removed after 6 weeks of surgery.
Outcome
The patient has been monitored and seen in the outpatient clinic every month for the past six months and has had no complaints since. The ureteroceles disappeared (Figure 5), the right lower moiety hydronephrosis decreased with an increase in cortical thickness, and there was significant improvement in left upper moiety hydronephrosis. His renal function tests are normal.
Discussion
Duplex collecting system is a congenital abnormality in which varieties of complete and incomplete duplications of the collecting system happen because of an incomplete fusion of upper and lower pole moieties [3]. The incidence of duplex kidney malformation is about 0.8%, and it is more common in women. The duplex kidney can be divided into incomplete type (Y type) and complete type. The incidence of complete ureteral deformity is about 0.2% [4]. Only 25% of these cases are reported to be bilateral [5]. Bilateral complete renal duplication with ureteral ectopia is a rare condition, found more commonly in females. The exact incidence is not known, as it is mostly an incidental finding [6]. Duplicated collecting systems could be associated with other deformities such as ureterocele, UPJO, VUR and ectopic ureter which is the most common [6]. A various range of symptoms might manifest according to the associated distortions and the case severity. The vast majority of cases are being diagnosed in early childhood [7]. However, a large number of patients are asymptomatic and diagnosed incidentally. The most important and common symptoms are those related to VUR and urinary tract infections [3]. Urinary incontinence is the commonest presenting complain of an ectopic ureter, usually in female as insertion of an ectopic ureter bypass the external urethral sphincter [7]. In addition, the distal segment of ectopic ureters inserting at the verumontanum can elevate the bladder neck, causing outlet obstruction in boys of any age [8]. In all cases, imaging is mandatory to confirm the diagnosis and uncover the associated deformities. Although the ultrasound provides excellent anatomic information, it struggles to detect the duplication and the related abnormalities [3]. Renal function and damage on kidney by duplication can be assessed by Intravenous Pyelogram (IVP) which appears as delayed excretion or even no excretion [9]. Intravenous pyelogram could also be used to clearly determine the level of convergence between ureters when diagnosis is in doubt between complete versus partial duplication. Computed tomography and MR Urography have been shown to more clearly demonstrate the anatomy of the renal parenchyma, the collecting system, and the ureter and ureteral orifice, when compared to visualization on IVU and ultrasound [6]. Renal Scintigraphy may be done to assess scar tissue, upper and lower pole function in complete duplication to help in choice of therapy [10]. Micturating Cystourethrogram (MCUG) could detect vesicoureteral reflux. Cystoscopy could help in detecting anomalies like ectopic ureter [7]. Treatment for duplex kidneys needs to be individualized [4]. The goals of treatment are control of infection, protection of normal ipsilateral and contralateral units, preservation of renal function, treatment of Vesicoureteral Reflux (VUR), minimization of surgical morbidity, facilitation of subsequent reconstructive procedures, and maintenance of continence [10]. When indicated, the type of surgery for children with the complicated duplex renal anomaly is based on renal moiety function and lower tract anatomy. Sequential treatment is meaningful to reduce bladder disturbance, reduce surgical trauma, and improve the success rate of surgery [4]. Surgical options include upper pole partial nephrectomy or heminephrectomy in nonfunctional duplex system, laparoscopic ureteral ligation (clipping), ureteral reimplantation in preserved renal function. When there is preserved kidney function or a functioning upper pole in duplex system kidney, the surgery technique consists of ureteroneocystostomy or distal and proximal ureteroureterostomy respectively [7]. Simultaneous bilateral renal procedures in children have been well documented in small numbers of patients. A few studies have shown efficacious open synchronous bilateral pyeloplasty’s. Kapoor et al performed a minimally invasive method of heminephrectomy and contralateral ureteroureterostomy to manage bilateral duplex systems in young children. There were no intraoperative or postoperative complications, establishing the safety of simultaneous bilateral robotic approach in bilateral duplex systems [11]. In our case, where the availability and expertise of minimally invasive surgery were not present, using the bilateral open approach, we were able to complete both the right hemi nephroureterectomy procedure and the left ureteropyelostomy in a single operative session, saving the patient from having to undergo a second surgery.
Conclusion
Bilateral complete duplication of the ureters is a rare condition. To the best of our knowledge, we report the first case of bilateral complete duplication of the ureters with a right intravesical ureterocele and a left extravesical ureterocele that was managed with a single-setting right hemi nephroureterectomy and left pyeloureterostomy. This case report demonstrates the safety of simultaneous open bilateral procedures for complete bilateral duplex systems.
Declarations
Provenance and peer review: Not commissioned, externally peer reviewed.
Ethical approval: This type of study does not require any ethical approval by our institution.
Sources of funding: This case report hasn’t been funded by any person or any institutions.
Declaration of competing interest: There is no any conflicts of interest with this article.
Consent: Written informed consent was obtained from the patient’s mother for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this Journal on request.
References
- Privett JTJ, Jeans WD, Roylance J. The incidence and importance of renal duplication. Clinical Radiology. 1976; 27(4): 521-530. doi:10.1016/s0009-9260(76)80121-3.
- RA Agha, T Franchi, C Sohrabi, G Mathew, A Kerwan, et al. The SCARE 2020 guideline: Updating consensus surgical Case Report (SCARE) guidelines, Int. J. Surg. 2020; 84: 226-230. https://doi.org/10.1016/j. ijsu.2020.10.034.
- Muhamad Sinan Muhamad, Mohammad Anas Mousa, Majdy Oukan, Ali Razzok. Giant hydronephrosis secondary to an ectopic ureter associated with bilateral duplex collecting system: A case report, Oxford Medical Case Reports. 2022; 4: 034. https://doi.org/10.1093/omcr/omac034.
- Wu C, Ji F, Zhang H, Yao Z, Li L, et al. Treatment for complete bilateral duplex kidneys with severe hydronephrosis and ureterectasis of the upper moiety in a child: A case report and literature review. Front. Surg. 2022; 9: 1019161. doi: 10.3389/fsurg.2022.1019161.
- Cassell AK, Traoré A, Jalloh M, Ndoye M, Diallo A, et al. Bilateral Ureteral Duplication and Right Ectopic Ureter Presenting with Incontinence: A Case Report. Med Sur Urol. 2019; 8: 216. doi: 10.35248/2168-9857.19.8.216.
- Mittal MK, Sureka B, Gupta P, Mittal A. Bilateral duplex system with overlooked dysplastic moiety: A rare cause of incontinence. J Mahatma Gandhi Inst Med Sci. 2014; 19: 67-9.
- Singh, Sampurnaa, Bhusal, Narayan Prasada; Mishra, et al. Bilateral complete duplication of ureter with ectopic ureter presenting as persistent urinary dribbling with normal voiding pattern in 17-year-old female: Case report. Annals of Medicine & Surgery 2022; 84. | DOI: 10.1016/j.amsu.2022.104824.
- Docimo, Steven. The Kelalis--King--Belman Textbook of Clinical Pediatric Urology. 2018. 10.1201/9781315113982.
- Yuri P, Utama ETPA complete duplicated collecting system with giant ureterocele in adult: Case report. Int. J Surg. Case Rep. 2021; 79: 49-52. doi: 10.1016/j.ijscr.2020.12.083.
- Gearhart JG, Rink RC, Mouriquand PDE. Pediatric urology.Philadelphia: Elsevier Health Sciences. 2010.
- Kapoor V, & Elder JS. Simultaneous bilateral robotic-assisted laparoscopic procedures in children. Journal of Robotic Surgery. 2015; 9(4): 285-290. doi:10.1007/s11701-015-0528-x.