
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Case report on craniotomy for bilateral epidural hematoma
Vaishnavi Dongare1*; Manjusha Mahakalkar2; Shalini Moon3
1Msc (Nursing), Department of Obstetrics and Gynecological Nursing, Datta Meghe Institute of Medical Sciences (Deemed to be University) and Smt. Radhikabai Meghe Memorial College of Nursing Sawangi (Meghe), Wardha, Maharashtra, India.
2HOD of Department of Obstetrics and Gynaecological Nursing, Datta Meghe Institute of Medical Sciences (Deemed to be University) and Smt. Radhikabai Meghe Memorial College of Nursing Sawangi (Meghe), Wardha, Maharashtra, India.
3Assistant Professor, Department of Obstetrics and Gynaecological Nursing, Datta Meghe Institute of Medical Sciences (Deemed to be University) and Smt. Radhikabai Meghe Memorial College of Nursing Sawangi (Meghe), Wardha, Maharashtra, India.
*Corresponding Author : Vaishnavi Dongare
Msc (Nursing), Department of Obstetrics and Gynecological Nursing, Datta Meghe Institute of Medical Sciences (Deemed to be University) and Smt. Radhikabai Meghe Memorial College of Nursing Sawangi (Meghe), Wardha, Maharashtra, India.
Email: vaishnavidongare2169@gmail.com
Received : Mar 31, 2025
Accepted : Apr 21, 2025
Published : Apr 28, 2025
Archived : www.jcimcr.org
Copyright : © Dongare V (2025).
Abstract
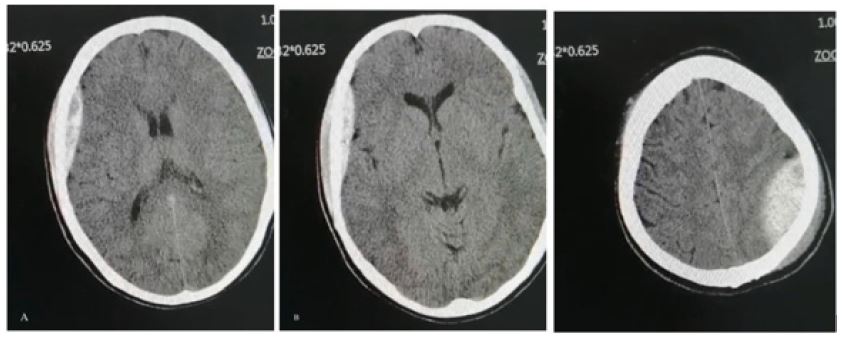
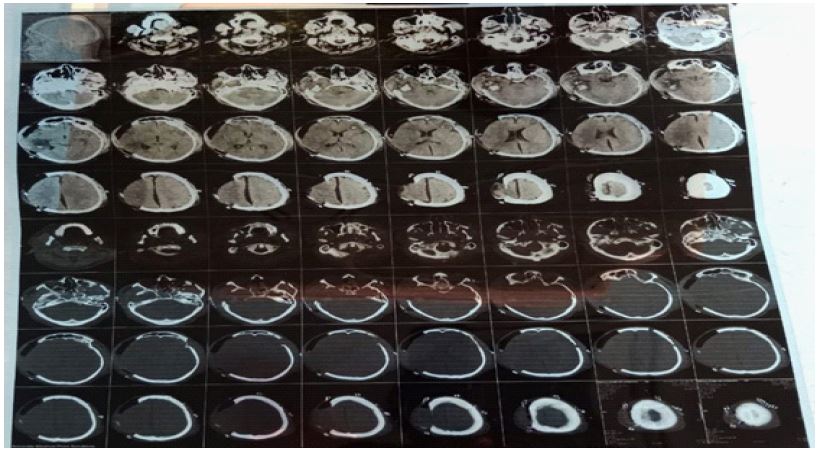
The most frequent type of traumatic brain is an Epidural Hematoma (EDH). Because the brain stem is so close to this condition, it can become fatal very quickly if it is not recognized and treated appropriately. Early magnetic resonance imaging (MRI) of the head allows for a prompt diagnosis, and prompt evacuation is crucial. Under general anesthesia, this procedure makes a hole in the skull so that a blood clot between the dura (the membrane enclosing the brain) can be removed. Trauma to the head frequently results in epidural hematomas, which can put dangerous pressure on the brain. Following an RTA resulting from a fall from a drunken bridge, a 27-year-old male patient complained of a head injury, a right ear bleed, and one episode of vomiting. A 1.5 mm section has been used to perform a CT scan starting at the foramen magnum and working upward. Right frontotemporal-parietal craniotomy status with extra-axial rheumatic collection at the surgical site and a subdural hygroma component, as previously mentioned. Pericranial soft tissue thickening on both sides of the surgical site may indicate postoperative changes. A diffuse axonal injury affecting the corticomedullary area of the left high frontal convexity and the corpus callosum splenium region is evident in the intraparenchymal hemorrhagic contusion, which primarily affects the lobe as previously described. As previously mentioned, the hemosinus, left zygomatic maxillary complex, and medial orbital wall are visible in the visualized size lesion.
Keywords: Head injury; Magnetic resonance imaging; Tracheotomy; Decompressive craniotomy; Hematoma.
Citation: Dongare V, Mahakalkar M, Moon S. Case report on craniotomy for bilateral epidural hematoma. J Clin Images Med Case Rep. 2025; 6(4): 3570
Introduction
An Epidural Hematoma (EDH) is a blood clot that forms between the dura mater, the outermost protective membrane surrounding your brain, and your skull. Usually, a fractured skull causes an artery to tear. Among the symptoms are a severe headache and loss of consciousness. Emergency surgery may be necessary due to this potentially fatal condition. This procedure involves making an incision through the skull while under general anesthesia in order to remove a blood clot that is between the dura [1], or membrane that surrounds the brain, and the skull. An epidural hematoma is a common after effect of head trauma that can put dangerous pressure on the brain. Following a head trauma, an individual with an epidural hematoma (EDH) briefly loses consciousness. After that, there may be a few hours of alertness before there is a loss of consciousness and a decline in brain function [2]. Some people go into a coma after losing consciousness. Keep in mind that while not all EDH patients experience these symptoms, most do [3]. A severe headache, nausea, vomiting, an enlarged pupil (a large, black area in the center of one eye), confusion, slurred speech, dizziness, and weakness in one side of the body are some additional symptoms that can result from a head injury and may manifest minutes to hours later. If the bleeding is not stopped, brain pressure will increase and symptoms might get worse. At this point, symptoms could include brain damage, coma, seizures, dyspnea, and even death. It usually requires immediate treatment if left untreated, as it can result in brain damage or even death. In as many as 15% of cases, an EDH is fatal. A bilateral hematoma epidural (EDH) [4], 75% of cases involve a skull fracture. Most often, bleeding originates from a fractured skull that tears the middle meningeal artery. Sometimes, vein bleeding results in the formation of an EDH. It’s also possible for non-trauma-related factors to raise an EDH. These can include bleeding tumors (hagic tumors), infections/abscesses, coagulopathy (blood not clotting as it should), vascular malformations (such as cavernous and arteriovenous malformations). Most frequently, spontaneous bleeding from veins due to coagulopathies or excessive blood thinning from anticoagulant medications causes spinal epidural hematomas. Extraneous causes comprise vertebral fractures, lumbar punctures, epidural anesthesia, tumors in the spinal cord, and spinal arteriovenous malformations. Epidural hematomas are caused by bleeding between the dura mater [5], the brain’s tough outer membrane, and the skull. After a head injury, consciousness is frequently lost, briefly regained, and then lost again.Headache, disorientation, vomiting, and immobility in certain body parts are possible additional symptoms. Errors could be among the complications [5]. An injury to the head usually causes bleeding from the middle meningeal artery and a fracture of the temporal bone. A bleeding disorder or blood vessel malformation may occasionally be the cause. Usually, an MRI or CT scan is used to diagnose conditions. The name “spinal epidural hematoma” refers to this condition when it affects the spine. An emergency craniotomy or burr hole is typically the method of treatment. Death usually follows without treatment. In one to four percent of head injuries [1], the condition manifests. A bleeding between the dura mater, the brain’s protective outer membrane, and the skull is known as an epidural hematoma. After a head injury, consciousness is frequently lost, briefly regained, and then lost again. Headache, disorientation, nausea, and immobility in certain body parts are possible additional symptoms. Seizures are one type of complications. Usually, a head injury that fractures the temporal bone and causes bleeding from the middle meningeal artery is the cause. It can sometimes be brought on by a blood vessel malformation or bleeding disorder [6]. An MRI or CT scan is usually used to make the diagnosis. When this illness affects the spine, it is. Usually, young adults experience it [3]. Compared to females, males are more commonly affected. Pinning the patient’s head and neck in place during surgery is a common and necessary procedure for ensuring optimal safety and positioning of the patient. Only infrequently but possibly fatally, application-specific complications arise [7]. Complicated cases involving adults have been documented. The scalp is then incised above the hematoma by the surgeon in a lengthy, arched fashion. In order to reveal the skull, the soft tissue is folded back. A portion of bone is liberated from the skull by the surgeon by sawing in between one or more tiny holes that were drilled. This “skull flap” comes off and gets put away. This gives the surgeon direct access to the hematoma. Using a suction device [1], the surgeon carefully removes the hematoma from the space between the dura and the skull. Treatment will be administered to the area surrounding the cauterized bleeding hematoma [5]. After the hematoma is removed, the skull flap can be replaced and secured with screws and plates. To avoid fluid accumulation at the surgical site, a temporary drain may occasionally be implanted. After the skin flap is folded back, it is sealed with surgical staples or sutures.[6]. If the patient has had significant brain swelling, the bone flap might need to be taken out and put back in place during a follow-up procedure a few weeks later. The family of the patient gave their written, informed consent so that this case study and any associated images could be published [7].
Case presentation
A 27-year-old man who had been drinking was admitted with complaints of head trauma, a bleed in his right ear, and one episode of vomiting after suffering a rib fracture. He weighs 70 kg, is 160 cm tall, and has a BMI of 27. Patient with No prior medical history exists. At 42 weeks, he underwent a normal prenatal screening and was born via full-term vaginal delivery. No, birth defect. For the past five to six years, the patient has chewed tobacco or kharra for seven or eight years. After every investigation was completed, my patient’s diagnosis was craniotomy for bilateral epidural hematoma. He was periodically admitted to the hospital for the illness’s treatment. The patient did not experience complications until that point, proving its effectiveness. Investigation completed: gathering of medical history, physical examination (such as a routine pelvic or rectal exam), blood work, ultrasound of the abdomen and pelvis, magnetic resonance imaging, CT scan plan, etc. Syp. Duphalac 30ml, Vitamin D3 sachet 60k, Inj. Heparin 5000 IU subcutaneous, Nebulization (dulin+Budocort+Mucomix), Tab. pan 40 mg, Tab. Dolo 650 mg, Tab. levepil 500 mg, Cap. Felicita, syp. Kesol 10 ml, Inj. dextrose 25%, syp. Glycerol 30 ml, Tab. Parkidin 100mg, Tab. Amlo 5mg, Inj. piptaz 4.5 gm IV, and Inj. Neomol 100ml IV are also included in the Therapeutic Intervention. Regarding the administration of procedures, the recommended surgical procedures are craniotomy and hemostatectomy. To accomplish this, a piece of your skull must be removed, the blood clot must be removed, any visible bleeding must be stopped, and a small screw must be used to replace the missing skull bone. A different kind of surgery involves making one or more holes in your skull to let blood out. Drawing blood releases the pressure that the blood clot exerts on the brain. The drain may remain in place for a few days following surgery to allow the blood to drain. After surgery, your neurologist or neurosurgeon might advise you to take medication to reduce inflammation and intracranial pressure. Glycerol, hypertonic saline, and mannitol can be prescribed. A prescription for an anti-seizure medication may also be given for a period of time. Seizures can occasionally be brought on by head trauma. Your neurologist will prescribe physical, occupational, and/or speech therapy since the doctor has found brain damage.

In physical examination, A low GCS score, orbital enema on the left side, unconsciousness, lack of assessment of the airway and spine, ETT 7.5 mm intubation, B/L RTL 3 mm pupils, auditory S2 sounds, and non-visible jugular venous pulse are all present in this patient. Although the patient’s vital signs-blood pressure, pulse, respiration rate, and saturation point-were stable upon admission (156/90 mmHg, 18/min, 100%), his GCS (M=6, V=4, E=4) indicated confusion. During the neurological exams, pupils were found to be bilaterally equally reactive and to have no motor or sensory deficiencies.
The complete blood count shows the following: AB+ve blood group, 14.6% hemoglobin, 19900 total leucocytes/microliter, 220,000 total platelets/microliter, 30.3 seconds for the APTT, and 122 mg/dl of blood sugar. Blood urea: 13 mg/dl, serum creatinine: 1.0 mg/dl, sodium: 139 mEq/L, potassium: 3.0 mEq/L, SGPT: 95 units/liter, SGOT: 112 units/liter are the results of the kidney function test. Protein: 6.9 g/dl, Albumin: 4.2 g/dl, Globulin: 2.7 g/dl, in relation to liver function the levels of conjugate, unconjugate, and total bilirubin are 0.2 mg/dl, 0.3 mg/dl, and 0.5 mg/dl, respectively.
In USG Abdomen and Pelvis, impression: hepatomegaly with a 16.2 cm liver and an 11.3 cm spleen, both with grade I fatty livers. renal: the left kidney measures 9.3-4.3 cm, while the right kidney measures 9.2-4.1 cm. CT brain plan, Right tempo parietal convexity and left frontal convexity both have acute extradural hematomas. Right temporal lobe hemorrhagic contusion with mild perilesional edema, Pneumocephalus, mild acute subarachnoid hemorrhage in the basal cistern involving the peri mesencephalic and interpeduncular cistern, multiple tiny hemorrhagic contusions in the left frontal and bilateral parietal lobes, Compression of the lateral ventricles, a 2 mm shift in the midline to the left, and the multiple calvarial and fac-io-maxillary fractures mentioned above are indicative of the mass effect.
Thickness of the pericranial soft tissues in both operative sites, indicating possible postoperative changes. There is evidence of diffuse axonal injury involving the corticomedullary area of left high frontal convexity and corpus callosum splenium region in intraparenchymal hemorrhagic contusion, which primarily affects the left frontal lobe and right temporal lobe as previously described. Hemisinus, the left zygomatic maxillary complex, and the medial orbital wall are visible in the visualized size lesion, as mentioned previously.
Discussion
Especially after the first one has been removed, sequentially developed hematomas are less common than bilateral epidural hematomas. The case study highlights the common misconception that some intracranial hematomas may develop gradually and go undetected on initial brain CT scans, emphasizing the significance of ongoing patient monitoring for head injuries. There are several possible causes of delayed hematomas, including CSF leakage, hypertension, hyperventilation, vascular necrosis from enzyme leakage, and underlying clotting abnormalities. Even when there are no more skull fractures, these hematomas can still develop, especially when there is venous bleeding [8]. Head trauma frequently results in epidural hematomas, which can put dangerous pressure on the brain. Should the patient’s course be entirely explained by the brain CT findings, or if the patient worsens following initial recovery, additional imaging should be taken into consideration [7]. Another significant point in the case study is intraoperative brain swelling in cases of epidural hematomas. If the patient does not become conscious again soon after the hematoma is removed, further brain imaging may be required as this could be the initial indication that a hematoma is growing on the lesion’s opposite side.In our case, a key indicator of the potential development of the hematoma on the opposite side may be the diastatic fracture’s extension to the contralateral side [9]. Bilateral epidural hematomas are associated with a high death rate because patients with double EDH most often lack lateralization, have lower GCSs, lucid intervals less frequently, and deteriorate more frequently than those with unilateral hematomas [5,8]. Bilateral EDH can be of two types: the commoner first type has venous bleeding that happens gradually, while the second type has arterial bleeding. Bilateral epidural hematomas may result from damage to the middle meningeal arteries, as in this instance. Two groups of neurosurgeons should perform simultaneous bilateral craniotomies when performing emergency and rapid decompression of the brain. Positive outcomes and a shorter recovery period can be achieved by excising the epidural hematomas and executing simultaneous bilateral craniotomies. A bilateral four-burr hole conventional craniotomy involving two scalp flaps may still not be possible to perform with two neurosurgeons operating at the same time, and in the absence of power-driven craniotomy facilities, the procedure may take longer to complete [9]. This will speed up and enhance the outcome of the procedure by removing the epidural hematomas and performing bilateral craniotomies at the same time. This was corrected by combining the anterior and posterior broad-base scalp flaps with a bi-coronal incision that provided sufficient exposure [10]. Observe that the right-sided EDH was also exposed prior to any damage being done to the left extradural hematoma [8]. Hemostasizing and clearing the blood clot may have taken longer than expected, delaying the decompression of the opposing side. With the bone flap removed and the left-sided craniotomy performed, the brain parenchyma decompressed, giving us more time to operate on the other side. To sum up, bilateral EDH is rare, and symmetrical EDH is extremely uncommon [6].
Conclusion
Despite their rarity, epidural hematomas need to be taken into consideration when treating patients. This case highlights the need for monitoring after an epidural hematoma operation and CT scans if the patient does not improve immediately after the hematoma is removed, especially if the initial CT scan was done less than six hours after the trauma. The contralateral side’s fracture line and the surgically observed, inexplicable brain swelling may shed some light on this case.
Declarations
Informed consent: creating a case report, the patient’s parents gave their informed consent and signed it.
Conflict of interest: Nil.
References
- Temporoparietal Craniotomy for Epidural Hematoma - cns.org [Internet]. 2023. https://www.cns.org/nexus/trauma/case/temporoparietal-craniotomy-epidural-hematoma.
- Default [Internet]. Craniotomy for Epidural Hematoma. 2023. https://www.wkhs.com/health-resources/wk-health-library/medical-procedures-tests-care-and-management/a-z/craniotomy-for epidural-hematoma
- Eftekhar B, Ketabchi E, Ghodsi M, Esmaeeli B. Bilateral asynchronous acute epidural hematoma: A case report. BMC Emerg Med. 2003; 3(1): 1.
- Cleveland Clinic [Internet]. Epidural Hematoma (EDH): Symptoms, Causes & Treatment. https://my.clevelandclinic.org/health/diseases/22034-epidural-hematoma. 2023.
- Cleveland Clinic [Internet]. Epidural Hematoma (EDH): Symptoms, Causes & Treatment. 2023. https://my.clevelandclinic.org/health/diseases/22034-epidural-hematoma.
- Agrawal A. Bilateral Symmetrical Parietal Extradural Hematoma. J Surg Tech Case Rep. 2011; 3(1): 34-6.
- Default [Internet]. Craniotomy for Epidural Hematoma. 2023. https://www.wkhs.com/health-resources/wk-health-library/medical-procedures-tests-care-and-management/a-z/craniotomy-for-epidural-hematoma.
- Microvascular Decompression for Trigeminal Neuralgia - Birmingham, AL - Spine and Neurosurgery [Internet]. 2023. https://neurosurgicalassociatespc.com/microvascular-decompression-for-trigeminal-neuralgia/.
- Craniotomy for Epidural Hematoma-Birmingham, AL - Spine and Neurosurgery [Internet]. 2023. https://neurosurgicalassociatespc.com/craniotomy-for-epidural-hematoma/
- Agrawal A. Bilateral Symmetrical Parietal Extradural Hematoma. J Surg Tech Case Rep. 2011; 3(1): 34-6.