
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Commentary - Open Access, Volume 6
Evidence-based medicine has reached maturity: Constant adaptation is imperative for its sustained progress
Spyridon Gkoufas1; Dimitrios Farmakis2; Dennis V Cokkinos3*
1Doctor in Training, Molai General Hospital, University of Athens, Greece.
2Assistant Professor of Medicine, University of Athens, Greece.
3University Research Associate, Biomedical Research Foundation, Academy of Athens, Greece.
*Corresponding Author : Dennis V Cokkinos
University Research Associate, Biomedical Research Foundation, Academy of Athens, Greece.
Email: dcokkinos@bioacademy.gr
Received : Apr 02, 2025
Accepted : Apr 22, 2025
Published : Apr 29, 2025
Archived : www.jcimcr.org
Copyright : © Cokkinos DV (2025).
Citation: Gkoufas S, Farmakis D, Cokkinos DV. Evidence-based medicine has reached maturity: Constant adaptation is imperative for its sustained progress. J Clin Images Med Case Rep. 2025; 6(4): 3571.
Short commentary
When in 1992 Gordon Guyatt and David Sackett introduced the principles of evidence-based medicine (EBM) as a new paradigm for medical practice in a ground-breaking article, they expressed the anxiety that it might eventually be “hijacked” by industry [1]. Since then, ΕΒΜ has dramatically changed our practice of medicine and luckily their fears have not been realized. Industry may largely guide evidence generation but safety valves for braking its influence are continuously being introduced.
The changing face of evidence base medicine
A new danger may however be lurking: The overtaking of clinical trials, which have been the backbone of EBM. They have gradually been replaced not only by meta-analyses, which are of higher value but more difficult to produce by systematic reviews, and finally even “critically appraised topics” (CATs). According to the Charles Sturt University (Australia) a CAT is a short summary of the best available evidence on a focused question, a shorter, less rigorous type of systematic review, providing an assessment of what is known about an intervention or issue by searching and appraising relevant studies. Even critically appraised individual articles a lesser endeavour are placed above RCTs [2].
This is another effort of the scholars and cartographers to undermine the daring navigators.
It has been suggested that these “filtered” forms of information are higher in the hierarchy of evidence as they assess the quality of data generated by individual studies, provide more definite answers and help knowledge application in clinical practice, while saving scholars’ time. However, to the large groups of practicing physicians who arduously and assiduously plan, execute, follow, review and finally publish a large clinical trial, which may often include thousands of individuals, this is equivalent to adding insult to injury. The pains of steering committees, safety boards, reviewing bodies and numerous enrolling centres, along with the huge costs of up to many million dollars in large randomized clinical trials (RCTs) may be annulled by one consultant and two students using a somewhat advanced computer, with minimal costs. Indeed, EBM is in lesser danger of being “hijacked” than actually being grounded. As time goes by, the meditating spectators might be dominating the gladiators who are exposed to the killing field.
Even so, M-A and SA are not sacrosanct. In 2021 it was estimated that nearly 1/3 of published systematic reviews and M-A published in orthopaedic journal are not completely reliable [3].
JPA Ioannidis, one of the acknowledged experts in the field, refers to M-A, tongue in cheek, as a good tool to make mistakes [4].
Heart Journal in 2022 state that we are now facing an overproduction of metanalyses, because of ease of conduction and high likelihood of many citations; the question whether they are precious or fool’s gold [5].
The future structure of the EBM pyramid
Can this trend be reversed? There are no easy answers, but some evidence is already emerging.
First of all, RCTs are being rejuvenated by virtue of technological advances in the fields of artificial intelligence (AI), wearable sensors and data transfer protocols. The impact of AI is being felt more significantly over time and may renovate all stages of medical research including discovery of new drug or old drug repurposing discovery, image interpretation, data organization and analysis and study workflow [6].
Additionally AI can provide an additional support: The in silico clinical trial thus rendering clinical trials more “intelligent’, ensuring a better performance in the following aspects: Design, recruitment, conduct and analysis.
Askin et al stressed that AI could contribute in the design, recruitment, conduct and analysis of RCTs [7]. It can also identify patients most likely to benefit, thus reducing neutral trials.
The humble case report
Another important aspect is case reports. Although not regarded as the next to last lower evidence by some sources [2]. It is been realized that well studied case reports if can create reliable M-A especially in rare or with long latency and orphan diseases [8].
Darren Mylotte deputy board of Europe Intervention wrote in 2018 an Editorial with a provocative title: The humble case report: bottom of the evidence-based medical pyramid or the foundation of clinical research? [9].
Trisha Greenhalgh in a paper of 2020 [10] mentions the proposal by Murad et al [11] towards a new pyramid in which the limits among RCTS, Cohort Studies, Case Control studies and Case Series/Reports are not straight any more but allow crossovers (Figure 1).
This places a responsibility on journal publishing case reports to follow a homogeneous approach for better utilization and recruitment of data to be used in M-A.
The comeback of mechanistic and pathophysiological reasoning
During the years after its introduction and maturity, RCTS and other clinical studies are the systematic analysis and meta analysis derived from them have been the Mainstay of EBM. However, subsequent research in the pathophysiology of many diseases has shifted the attention to mechanistic reasoning in EBM.
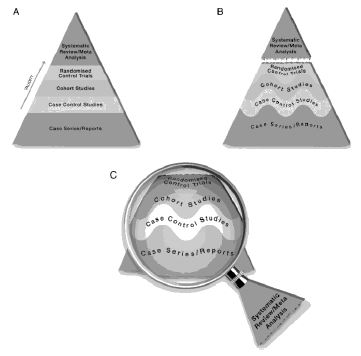
The proposed new evidence-based medicine pyramid. (A) The traditional pyramid. (B) Revising the pyramid: (1) lines separating the study designs become wavy (Grading of Recommendations Assessment, Development and Evaluation), (2) systematic reviews are ‘chopped off’ the pyramid. (C) The revised pyramid: systematic reviews are a lens through which evidence is viewed (applied).
Howick et al [15] have argued, 15 years ago, that just relying on the results does not give an explanation on how they were derived, that the explanation remains in a “black box”. However the place great importance of the caveat that only high-quality mechanistic reasoning should be accepted.
The Russo-Williamson thesis is frequently mentioned or employed. It maintains that establishing a causal claim in medicine requires establishing both correlation and the mechanism [13].
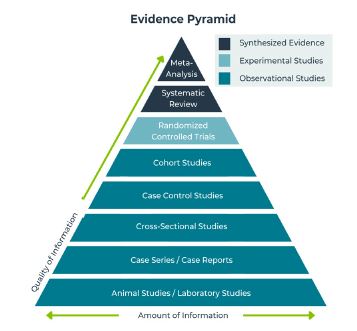
Holly Anderson [14] as early as 2012 argued that while EBM reasoning relies on recommendation derived from high quality studies, in clinical practice. She argues that reasoning based on mechanisms has a distinct role in broad treatment guidelines. It should be remembered that pathophysiological mechanisms to a great extent provided by vitro and animal studies which up to now occupy the lowest position in the evidence pyramid (Figure 2). It is not surprising that pathophysiology is gaining ground in view of the great progress in research on mechanisms.
Mechanisms are also very important when addressing the results of drug combination. In order to explain the favourable or deleterious results emanating from these interactions [15].
Conclusion
The current pyramids of evidence based medicine (EMB) differ from their early structures, which placed randomized control trials of the top. Filtered information, consisting of systematic reviews –which are gradually and tacitly replacing the more demanding but also more reliable meta-analyses are gaining predominance. This is downgrading originality and quest of novel knowledge. Also, high quality case studies can add useful evidence.
Finally, pathophysiologic mechanisms are becoming relevant and important.
Declarations: None.
Disclosure of interest: None.
References
- Evidence-Based Medicine Working Group. Evidence-based medicine. A new approach to teaching the practice of medicine. JAMA. 1992; 268: 2420-5.
- Evidence-Based Practice in Health: The Evidence Hierarchy - What is the “Best Evidence”, https://canberra.libguides.com/c.php?g=599346&p=4149721 (accessed on Jan 14, 2024).
- Sudhakar P, Selvarathinam S, Anjali G. Artificial Intelligence in Clinical Trials- Future Prospectives. Bioequivalence & Bioavailability International Journal. 2023; 7(1): 2-6.
- Ioannidis JPA. Meta research: the act of getting it wrong. Research synthesis. Meth. 2010; 1: 169-84.
- Biondi-Zosia G, Windecker S, Juni P, Bhatt DL. Cardiovascular metanalyses: Fool’s gold or gold for fools? Eury heart J.LB3008-13.
- Subbiah V. The next generation of evidence-based medicine. Review. Nat Med. 2023; 29: 49-58.
- Askin S, Burkhalter D, Calado G, Dakrouni S EL. Artificial Intelligence Applied to clinical trials: opportunities and challenges. Health Technol (Berl). 2023; 13(2): 203-213.
- Sampayo-Cordero M, Miguel-Huguet B, Pardo-Mateos A, et al. Agreement between results of meta-analyses from case reports and clinical studies, regarding efficacy and safety of idursulfase therapy in patients with mucopolysaccharidosis type II (MPS-II). A new tool for evidence-based medicine in rare diseases. Orphanet J Rare Dis. 2019; 14(1): 230.
- Mylotte D. The humble case report: Bottom of evidence-based medical pyramid or the foundation of clinical research? EuroIntervention. 2018; 13. DOI:4244/EIJV13I18A343.
- Baek YS, Lee SC, Choi W, Kim DH. A new deep learning algorithm of 12-lead electrocardiogram for identifying atrial fibrillation during sinus rhythm. Sci Rep. 2021; 11: 12818.
- Murad MH, Asi N, Alsawas M, et al. new evidence pyramid. Evid Based Med. 2016; 21(4): 125-7.
- Howick J, Glasziou P, Aronson JK. Evidence-based mechanistic reasoning. J R Soc Med. 2010; 103(11): 433-41.
- Russo F, Williamson J. Interpreting casualty in the health science. Int studies philosophy science. 2007; 21: 257-70.
- Andersen Holly. Mechanisms: What are they evidence for in evidence-based medicine? J Eval Clin Pract. 2012; 18(5): 992-9.
- Düsing R, Waeber B, Destro M, et al. Triple-combination therapy in the treatment of hypertension: A review of the evidence. J Hum Hypertens. 2017; 31(8): 501-510.