
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Use of therapeutic plasma exchange in IgG-paraprotein- induced haemorrhagic diathesis in patients with multiple myeloma: A case report and literature review
Michael Liu1; Isabel Wiedl2; Ioannis Chanias1; Elisaveta Motoori Beifuss1; Martin Andres1; Johanna Kremer-Hovinga1; Michael Daskalakis1; Katarzyna Aleksandra Jalowiec1*
1Department of Haematology and Central Haematology Laboratory, Inselspital, Bern University Hospital, University of Bern, 3010 Bern, Switzerland.
2University of Bern, 3012 Bern, Switzerland.
*Corresponding Author : Aleksandra Jalowiec K
Department of Haematology and Central Haematology Laboratory, Inselspital, Bern University Hospital, University of Bern, 3010 Bern, Switzerland.
Tel: +41 31 632 96 01;
Email: katarzynaaleksandra.jalowiec@insel.ch
Received : Apr 01, 2025
Accepted : Apr 22, 2025
Published : Apr 29, 2025
Archived : www.jcimcr.org
Copyright : © Aleksandra Jalowiec KA (2025).
Abstract
Paraproteins are monoclonal immunoglobulins produced by clon- al plasma cells or B-lymphocytes. In myeloma patients, paraproteins can impair fibrin monomer polymerisation or cause thrombocyte dys- function. The indication for therapeutic plasma exchange for bleed- ing diathesis caused by them is not included in the current apheresis guidelines. Here we present a case report of a patient with relapsed, refractory myeloma in whom therapeutic plasma exchange was used to treat a life-threatening haemorrhagic diathesis, most probably due to impaired fibrin polymerisation. This treatment was conducted as a bridging to chimeric antigen receptor therapy and resulted in the ces- sation of bleeding. Further, a literature review was conducted to iden- tify similar cases with multiple myeloma in which therapeutic plasma exchange was conducted to treat bleeding symptoms.
Keywords: Therapeutic apheresis; Plasma exchange; Paraprotein; Myeloma; Bleeding.
Abbreviations: ACDA: Acid Citrate Dextrose Solution A; ACGH: Array Comparative Genomic Hybridisation; APTT: Activated Partial Prothrom- bin Time; ASFA: American Society for Apheresis; CAR: Chimeric Antigen Receptor; EPD: Elotuzumab, Pomalidomide and Dexamethasone; FBC: Full Blood Count; FISH: Fluorescence In Situ Hybridization; FFP: Fresh Frozen Plasma; HSCT: Haematopoietic Stem Cell Transplantation; Hb: Haemoglobin; HVS: Hyper viscosity Syndrome; IA: Immunoadsorption; MGUS: Monoclonal Gammopathy of Undetermined Significance; MM: Multiple Myeloma; IG: Immunoglobulin; KD: Carfilzomib And Dexa- methasone; PLTC: Platelet Concentrate; PD: Progressive Disease; PR: Partial Remission; PRBC: Packed Red Blood Cell Concentrate; PT: Pro- thrombin Time; RR: Relapsed And Refractory; SD: Stable Disease; Tc: Thrombocyte; TPA: Therapeutic Plasma Exchange; TT: Thrombin Time; WM: Waldenström’s Macroglobulinemia; VRD: Bortezomib, Lenalido- mide, Dexamethasone.
Citation: Liu M, Wiedl I, Chanias I, Motoori Beifuss E, Aleksandra Jalowiec K, et al. Use of therapeutic plasma exchange in IgG-paraprotein-induced haemorrhagic diathesis in patients with multiple myeloma: A case report and literature review. J Clin Images Med Case Rep. 2025; 6(4): 3572.
Introduction
Paraproteins are monoclonal immunoglobulins produced by clonal plasma cells or B-lymphocytes. They are related to a myriad of conditions from which most common are Monoclonal Gammopathy of Undetermined Significance (MGUS), Multiple Myeloma (MM) or B-cell lymphoproliferative disorders. Para- proteins contain either both, heavy and light chains, or either heavy or light chains of Immunoglobulin (Ig). The most common paraprotein type in plasma cell related diseases is IgG, whereas Waldenström’s Macroglobulinemia (WM) is associated with IgM paraprotein. Paraproteins can cause several complications and end organ damages like nephropathy, polyneuropathy, or cardi- opathy. Also, it has been described, that they can impair fibrin monomer polymerisation and cause Thrombocyte (Tc) disfunc- tion. According to the American Society for Apheresis (ASFA) guidelines, a Therapeutic Plasma Exchange (TPA) is a procedure in which blood of the patient is passed through a medical device which separates plasma from other blood components. During the procedure, the plasma is removed and replaced with a re- placement solution such as colloid solution (e.g., albumin and/ or plasma) or a combination of crystalloid/colloid solution. TPA is used to treat several neurological, congenital or haematologi- cal conditions. The indication for TPA is accepted as first-line therapy, either as a standalone treatment or in conjunction with other therapies (strong recommendation and high-quality evi- dence; 1A), for conditions like acute inflammatory demyelinat- ing polyradiculoneuropathy (Guillain-Barré syndrome), familial hypercholesterolemia, acute attack of multiple sclerosis, and Thrombotic Thrombocytopenic Purpura (TTP). According to ASFA guidelines [1]. There are two indications for TPA related to paraprotein associated disorders. Firstly, the treatment of symptomatic symptomatic Hyperviscosity Syndrome (HVS) in hypergammaglobulinemia (strong recommendation, moderate quality evidence; grade 1B), or it’s prophylaxis before treatment with rituximab (strong recommendation, low-quality or very low- quality evidence; grade 1C), a humanized monoclonal anti- CD20 antibody. This aims to avoid transient increase in parapro- tein level which is a known rebound phenomenon after the first therapy, short described as a ‘’flare’’ [2]. HVS is defined by clini- cal symptoms like mucosal bleeding, visual disturbances, neuro- logical symptoms ranging from headache, vertigo, and seizures to coma, as well pulmonary or cardiac decompensation and it is caused by increased viscosity of blood. It is most typically seen in WM associated with monoclonal IgM or, less frequently, with MM associated with monoclonal IgA or IgG3. Secondly, TPA can be used for treatment of chronic acquired demyelinating polyneuropathies like IgG/IgM/IgA paraproteinemic polyneu- ropathy (strong recommendation, moderate quality evidence; grade 1B). Here we present a case report of a patient with MM in whom TPA was used to treat IgG paraprotein-induced haem- orrhagic diathesis. Further, a literature review was conducted to identify similar cases with MM in which TPA was conducted to treat bleeding symptoms.
Case presentation
A 42-year-old Caucasian patient was initially diagnosed with IgG kappa multiple myeloma (MM) with a plasma cell infiltration of 90% on bone marrow trephine, and high-risk abnormalities on array Comparative Genomic Hybridisation (aCGH) including but not restricted to a gain of 1q with chromothripsis, monoso- my 13 and nullsomy Y, which lead to hypodiploidy (≤44), as well as near-tetraploid monoclonal plasma cells on Fluorescence In Situ Hybridization (FISH) with ploidy ±2n/±4n. He received multiple previous lines of treatment namely: 3 cycles of bort- ezomib, lenalidomide, dexamethasone (VRD) resulting in Stable Disease (SD); 3 cycles of Daratumumab (Dara)-VRD resulting in SD; 1st high-dose chemotherapy (treosulfan, melphalan) with autologous Haematopoietic Stem Cell Transplantation (HSCT) resulting in Partial Remission (PR); 2nd high-dose chemotherapy (treosulfan, melphalan) with rituximab and autologous-HSCT resulting in PR; maintenance therapy with Dara, resulting in Progressive Disease (PD); 9 cycles of carfilzomib and dexameth- asone (Kd) resulting in PD; 4 cycles carfilzomib, cyclophospha- mide and dexamethasone (KCd) resulting in PD; 3rd high-dose chemotherapy (treosulfan, melphalan) and autologous-HSC re- sulting in PD and he was awaiting manufacturing of Chimeric Antigen Receptor (CAR) T-cell therapy and receiving bridging therapy with elotuzumab, pomalidomide and dexamethasone (EPd). He presented to the emergency department with severe Gastrointestinal (GI) bleeding, namely hematemesis, melena and haematochezia, and syncopal episodes. The bone marrow trephine performed around 4 months before the start of bleed- ing symptoms, showed a plasma infiltration of 60%, whereas the trephine 4 weeks after, showed a plasma cell infiltration of nearly 100%. His Full Blood Count (FBC) showed a cytope- nia with life-threatening anaemia with Haemoglobin (Hb) of 27 g/L (normal range 135-168 g/L) and severe thrombocytopenia with Tc count of 16x109/L (normal range 150-450x109/L). The coagulation panel showed prolonged Thrombin Time (TT) with 31.8 sec (normal range 15.5-19.4 sec) while Prothrombin Time (PT), Activated Partial Prothrombin Time (appt) and fibrinogen were in normal ranges. The blood viscosity testing was not per- formed as this testing is not available in Switzerland anymore. The patient did not receive any anticoagulation, and any poten- tial intake was additionally excluded by thromboelastometric tests (Cloture®). Cloture® also did not show any clear pathol- ogy. A gastroscopy was performed and revealed diffuse mucosal bleeding in the corpus of the stomach, without any possibility of interventional bleeding cessation. After fluid replacement and transfusions of Packed Red Blood Cells (PRBC) and Plate- let Concentrates (PLTC), the patient was treated with high dose intravenous proton pump inhibitor and maximal daily dose of tranexamic acid. Further transfusions of PRBC and PLT concen- trates were needed as the defined transfusion thresholds of 70 g/L for Hb and 20x109/L for Tc count were not reached. The cu- mulative transfusion requirement was 17 units PRBC, 6 units of PLTC and 1 unit of Octuplets® (solvent/detergent treated pooled plasma; Octa pharma AG, Switzerland) over 4 consecutive days (4.25 PRBC/d, 1.5 PLTC/d, 0.25 Octuplets®/d) starting directly after hospital admission. Under this therapy, the patient con- tinued having GI bleeding. It was suspected that the elevated monoclonal paraprotein with an M-gradient of 39.9 g/L and to- tal serum-IgG of 47.8x109/L was impairing fibrin polymerization and resulting in TT prolongation. However, just one month prior to this bleeding episode, the TT was 63.8 sec and the M-gradi- ent 82.4 g/L with total serum-IgG of 104.4 G/L and the patient did not have any bleeding symptoms at that time. As the pa- tient was not responding to the current bridging chemotherapy, the sudden decrease in monoclonal paraprotein was attributed to the significant blood loss. On day 4 after hospital admission and with no significant improvement of the bleeding situation, an indication for TPA was made to further decrease the para- protein in order to improve fibrin polymerization. TPA was per- formed with the Spectra Optima® (Terumo CT, Lakewood, CO, USA), using replacement fluids consisting of 0.9% saline and 5% human albumin at the ratio of 1:2. As there was no suspicion that the patient was suffering from Thrombotic Thrombocyto- penic Purpura (TTP) due to negative haemolysis parameters (a Disintegrant and Metalloproteinase with a Thrombospondin Type 1 motif, member 13 (ADAMTS-13) was not measured), no plasma exchange with Octuplets® was performed. In our country, only Octuplets® which is a solvent/detergent treated, pooled human plasma indicated for replacement of multiple coagulation factors including in patients with TTP, could poten- tially be used. Blood products like cryoprecipitate or cry super- natant are not available. At our centre, for plasma exchanges, we usually use anticoagulation with Acid Citrate Dextrose Solu- tion A (ACDA) at ratio 1:14. During the first session, only 0.8- fold of blood volume was exchanged due to concerns of bleed- ing, as plasma exchange also removes procoagulant proteins. As a result, the total serum-IgG decreased from 47.5 to 27.0 g/L, the TT normalized from 26.0 sec to 17.5 sec. On the fol- lowing day, the Hb and Tc counts were stable and there was no need for further PRBC or PLT transfusions. Already after 12 hours, the serum IgG-level increased again to 40.6 g/L, owing both, the redistribution of tissue-bound IgG, as well as high dis- ease burden with constant production of paraprotein. The TPA was continued daily for 3 more sessions, with 1.2-fold of blood volume exchanged, and plasma transfusions were applied post apheresis if fibrinogen dropped <1 g/L. Those four TPA session were well tolerated by the patient and his transfusion require- ment reduced to 1 PRBC and 3 PLTC concentrates over the next 4 days, however during this time period 5 units Octuplets® were needed due to hypofibrinogenemia caused by TPA (1 PRBC/d, 0.75 PLTC/d, 1.25 Octuplets®/d). With stable haemoglobin level 24 hours after the last TPA, the patient was discharged home. TPAs were continued weekly in the outpatient setting, for alto- gether 10 sessions as the RRMM was progressive, despite bridg- ing antineoplastic therapy, and serum IgG levels were increasing continuously. In the outpatient setting, the transfusion require- ment reduced to 8 PRBC, 15 PLTC and 15 units of Octaplas® over the next 35 days (0.23 PRBC/d, 0.43 PLTC/d, 0.43 Octaplas®/d). In (Figure 1), a summary of treatment modalities and lab results is shown.
A bone marrow trephine as baseline assessment prior to CAR T-cell therapy showed a nearly 100% plasma cell infiltra- tion. A follow-up gastroscopy showed a complete remission of the bleeding. The last (11th) TPA was conducted directly before the infusion of CAR-T cells, which took place one month after the bleeding episode and is therefore not shown in (Figure 1). In case of our patient, TPA was used as a part of bridging strategy until the CAR T-cell therapy. During the inpatient stay following the CAR T-cell infusion, the patient suffered from multiple CAR T-cell related complications. The bone marrow trephine for ear- ly response assessment at day 20 showed SD, with plasma cell infiltration of 100% and increase in M-gradient to 74 g/L. The coagulation parameters after the CAR-T infusion showed nor- mal PT, persistently prolonged TT (20-43 sec), in the last 5 days before death prolonged APTT (36-63 sec), as well as decreased fibrinogen (0.87-1.5 g/L), most likely due to cytokine release syndrome. The thrombocytopenia persisted (9-30x109/L). Upon developing new bleeding complications with haemorrhagic pleural effusions and repeated GI bleeding, and lack of further therapeutic options, a transition to palliative care was decided, and the patient died at day 38 after the CAR T-cell infusion.
Table 1: Case characteristics, including age, gender, type of monoclonal protein, clinical presentation and sequence of bleeding occurrence, pathological coagulation parameters, treatment and outcome of bleeding are provided.
| Reference | Age | Sex | MM type | Paraprotein level | MM treatment during bleeding | Previous MMtreatment | Bleeding symptoms | Othersymptoms | Abnormal coagulationresults | TPA | Vital status |
|---|---|---|---|---|---|---|---|---|---|---|---|
| (Tan BL,Cleton FJ, van Beusekom GT, Veltkamp JJ, van Rood JJ., n.d.)[3] | 48 | M | IgGλ | NA | NA | Melphalan | Epistaxis, SAH,rectal | headache, unconsciousness | Prolonged TT,PT, andBT | 5.7 L (in first3 days),total22 L in 2 months | Survived |
| (Powles et al.1971) [4] | 30 | F | IgG | NA | NA | NA | GIbleeding, ulcer | NA | NA | 5 Lexchanged, exchangefluid: feezed-dried plasma | NA |
| (Palmer et al.1984) [5] | 49 | M | IgG4λ | NA | None | None | GI bleeding | nausea, vomiting, polydipsia, polyuria | Prolonged TT,PT, andapt | 1.5 L/cycle, 2 cycles | Died |
| (Wallace et al.1984) [6] | 52 | F | IgGλ | 70.7g/L | None | None | Delayed postoperative bleeding, prolongedhaematuria | No | Abnormal Tcfunction | 2.6 L,exchange fluid: saline, 1 L 5%albumin,1-liter FFP | Survived |
| (Goddard et al. 1990) [7] | 60 | M | LCMMλ | NA | MCP | MCP | Recurring GI bleeding, bleeding from laparotomy wound,epistaxis, oozing from dialysis cannulation sites | No | Prolonged TT and apt. | 3cycles onday1,3,8 | Survived |
| (Colwell, Tollefsen and Blinder,1997)[8] | 58 | M | IgGκ | 51.0g/L | NA | after 1st event: 3 cyclesof monthly melphalan (9 mg/m2), prednisone(40 mg/m2) for 4 d; after3rd event: CD34+selected autologous peripheral blood progenitor celltransplantation,high dose sulpha, cyclophosphamide (plasmapheresis) | recurrent bleeding,including haematuria, epistaxis and ICB | No | Prolonged TT andRT | intermittent, during 3 years | Survived |
| (Morita et al.2010)[9] | 84 | F | LCMMκ | 9.4g/L | Steroids | None | pulmonary haemorrhage, haematuria | Acute renalfailure | Prolonged apt | 3.2 L/cycle,for 3 d, exchange fluid:FFP | Survived |
| (Mortimer et al. 2021)[10] | 66 | M | IgAκ | 33g/L | VCD | None | post-BMAT buttockhaematoma | No | Abnormal Tcfunction | 3x, no furtherdetails | Survived |
| Ourcase | 42 | M | IgGκ | 39.9g/L | Pomelle | Auto-HSCT | GIbleeding | Syncopal symptoms | Prolonged TT | 11x,exchange fluid:albumin 5%,NaCl 0.9%,ratio 2:1. | Survived |
Abbreviations: APT: Activated Partial Thrombin Time; BMAT: Bone Marrow Aspirate and Trephine; BT: Bleeding Time; FFP: Fresh Frozen Plasma; GI: Gastrointestinal; HSCT: Haematopoietic Stem Cell Transplantation; ICB: Intracerebral Bleeding; F: Female; IgA: Immunoglobulin A; IgG: Immunoglobulin G; LCMM: Light Chain Multiple Myeloma; M: Male; MCP: Melphalan, Cyclophosphamide, Prednisolone; MM: Multiple My- eloma; NA: Not Available; Pomelle: Pomalidomide, Elotuzumab, dexamethasone; PT: Prothrombin Time; RT: Reptiles Time; SAH: Subarachnoid Haemorrhage; TC: Thrombocyte; TT: Thrombin Time; VCD: Bortezomib, Cyclophosphamide, Dexamethasone; κ: kappa, λ: lambda.
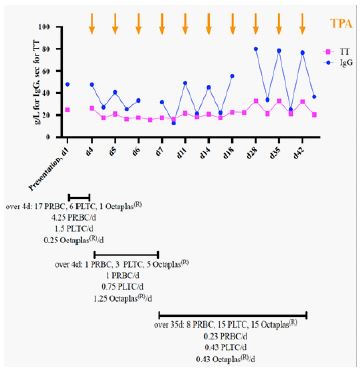
Abbreviations: d: day; PLTC: Platelet Concentrate; PRBC: Packed Red Blood Cell Concentrate; IgG: Immunoglobulin G; TPA: Therapeutic Plasma Exchange; TT: Thrombin Time; Sec: Seconds.
Literature review
A literature search was conducted in PubMed to eluci- date similar cases where TPA was used to treat MM patients with bleeding diathesis related to paraprotein. The following search terms were used: “plasma exchange”, “plasmapher- esis”, “myeloma”, “paraprotein”, “bleeding”, “haemorrhage”. It was aimed to exclude cases where HVS was probable cause of bleeding. As such, cases with retinal bleeding due to HVS or cases where increased blood viscosity was reported, were ex- cluded. The reason why HSV cases were excluded is that the indication for TPA in those is clear according to guidelines. Our aim was to focus on cases with haemorrhagic diathesis and no clear indication. Also, cases were acquired haemophilia second- ary to plasma cell neoplasms was diagnosed, were excluded. The focus of this literature review was to identify cases with abnormal coagulation panel related to IgG monoclonal protein. Altogether, 9 cases were identified, including our patient. Case characteristics, including age, gender, type of monoclonal pro- tein, clinical presentation and sequence of bleeding occurrence, pathological coagulation parameters, treatment and outcome of bleeding, are provided in (Table 1).
Reported cases of 5 male und 3 female patients were identi- fied. The median age was 54.3 (range, 30-84) years. Monoclonal protein of subtype kappa and lambda were equally distributed, (for both n=4, 44%, for one case the data is missing). In most cases (n=5, 56%), the level of paraprotein was provided and the paraprotein levels were listed in (Table 1) with a range of 9.4 g/l - 70.7 g/l. Overall, we could not observe a clear correlation between level of monoclonal immunoglobulins and bleeding severity. GI bleeding was the most common type of bleeding (n=4, 44%). Apart from haemorrhage, other symptoms varied, if mentioned at all. In all cases, TPA was used to treat the bleeding disorder. In most cases, the exact TPA conditions were not spec- ified. Interestingly, in 4 cases fresh frozen plasma, respectively freeze-dried plasma, were used as replacement fluid. Almost half (n=4, 44%) of patients were treated with systemic therapy for MM before the haemorrhage, or rather between events. Besides TPA, 5 patients received systemic therapy during the bleeding episodes. (Table 1) also demonstrate a chronology of MM treatment: Melphalan was used in older publications, while other alkylating agents, steroids, immunomodulating drugs, as well as proteasome inhibitors were administered in more re- cent studies. Almost half of patients (n=4, 44%) were initially di- agnosed with MM when presented with bleeding. The majority of patients (n=7, 78%) who were treated with TPA, survived the bleeding event. Nevertheless, the authors defined the bleeding events as life threatening in all patients using terms like “seri- ous”, “severe “, and “fatal” and describing clinical complications.
Discussion and conclusion
The prolongation of TT can be attributed to several reasons, including decreased levels of fibrinogen, dysfibrinogenaemia, increased fibrin (open) degradation products and heparin or other circulating anticoagulants. While it is known and de- scribed that high levels of monoclonal paraprotein can result in impaired fibrin polymerization [11,12], there is a paucity of pub- lished data on the use of TPA as treatment modality of bleeding complications, especially when there are no further options for local haemostatic interventions, or other coagulation distur- bances amenable to substitution with, Octuplets®, Fresh Frozen Plasma (FFP) or factor concentrates. Colwell and colleagues [8] found that at low concentrations the IgG is a direct inhibitor of thrombin, but at high concentrations it also inhibits fibrin po- lymerization. They concluded, that this dual effect of IgG may have accounted for the clinical bleeding in a patient with MM and a paraprotein level >50 g/l. The authors observed, that the TPA ameliorated the patient’s bleeding manifestations and par- tially corrected the TT without affecting other coagulation pa- rameters. However, our case shows that monoclonal protein at lower levels (<50 g/l) can lead to TT prolongation and significant transfusion-dependent bleeding diathesis requiring treatment. Our patient suffered from TT prolongation only. However, in other cases [9,5,7], parameters like PT and/or APTT were pro- longed as well, and other, unclear mechanisms might have been responsible for this. Interestingly, in two cases identified in our literature search [6,10], the paraprotein-induced abnormal Tc function was successfully treated with TPA. Also, in one case [5] a circulating heparin-like anticoagulant and in another, endog- enous glycosaminoglycan [7] anticoagulant production, were identified as bleeding causes and successfully treated with TPA. The possibility of HVS contributing to the bleeding diathesis was considered in our case, however it was regarded unlikely for HVS to be the leading contributing factor for the bleeding as there were no clinical signs of HVS. Furthermore, the bleed- ing continued despite a reduction of IgG paraprotein by 50%, resulting from the initial large blood loss. Unfortunately, a direct measurement of the serum viscosity was no longer available, as this test was systematically phased out in Switzerland as of 2022. Our case and other cases identified during the literature review, show that TPA can not only improve the elevated TT due to high levels of monoclonal paraprotein resulting in impaired fibrin polymerization, but also achieve haemostasis upon cor- rection of this pathophysiologic mechanism via removal of the paraprotein. As it can be seen in (Figure 1), the decrease in IgG level correlates well with decrease in TT and also reduces the transfusion requirement for PRBC and PLTC dramatically. How- ever, the transfusion requirement for plasma (Octuplets® in our case) can remain high or even increase, due to hypofibrinogen- emia related to TPA. Also, the literature review shows a variety of aetiologies that can be responsible for bleeding diathesis in patients with MM and be potentially treated with TPA. Other treatment options like Immunoadsorption (IA) were not applied in any case in the literature. IA was firstly reported in 1989 [13], after the first four cases were described. However, it can be a valuable option in such situations and should be taken into con- sideration if it is available in those urgent situations. However, a high level of Ig can be a limiting factor due to fast saturation of IA columns, making the therapy less efficient. In summary, we identified only a few cases of paraprotein-related haemor- rhagic diathesis described where TPA was used to treat bleeding symptoms. Despite the lack of official recommendation in ASFA guidelines, we suggest to early evaluate intervention with TPA in cases with plasma cell disorder causing a bleeding diathesis.
Declarations
Funding statement: No funding.
Institutional review board statement: No Ethic Committee Approval is needed for case reports according to the Swiss Hu- man Research Act.
Data availability statement: For this study, there are no pub- licly archived datasets analysed or generated during the study.
Conflicts of interest disclosure: The authors declare no con-flict of interest.
References
- Colwell, N.S., Tollefsen, D.M. and Blinder, M.A. (1997) Identifica- tion of a monoclonal thrombin inhibitor associated with mul- tiple myeloma and a severe bleeding disorder. British Journal of Haematology [online]. 97 (1), pp. 219–226.
- Ghobrial, I.M., Fonseca, R., Greipp, P.R., Blood, E., Rue, M., Ve- sole, D.H., Gertz, M.A., and Eastern Cooperative Oncology Group (2004) Initial immunoglobulin M ‘flare’ after rituximab therapy in patients diagnosed with Waldenstrom macroglobulinemia: an Eastern Cooperative Oncology Group Study. Cancer [online]. 101 (11), pp. 2593–2598.
- Goddard, I.R., Stewart, W.K., Hodson, B.A. and Dawes, J. (1990) Plasma exchange as a treatment for endogenous glycosamino- glycan anticoagulant induced haemorrhage in a patient with myeloma kidney. Nephron [online]. 56 (1), pp. 94–96.
- Hosokawa, S., Oyamaguchi, A. and Yoshida, O. (1989) Successful immunoadsorption with membrane plasmapheresis for multiple sclerosis. ASAIO transactions [online]. 35 (3), pp. 576–577.
- Kotlín, R., Sobotková, A., Riedel, T., Salaj, P., Suttnar, J., Reicheltová, Z., Májek, P., Khaznadar, T. and Dyr, J.E. (2008) Acquired dysfibrinogenemia secondary to multiple myeloma. Acta Haematologica [online]. 120 (2), pp. 75–81.
- Morita, Y., Yasuda, M., Nakao, M., Tsujimura, Y. and Isono, M. (2010) Pulmonary hemorrhage and acute renal failure as an initial presentation of multiple myeloma. Internal Medicine (Tokyo, Japan) [online]. 49 (14), pp. 1401–1403.
- Mortimer, J., Gray, N., Desborough, M., Baker, P., Kothari, J. and Eyre, T. (2021) Acquired platelet dysfunction in newly diagnosed myeloma. EJHaem [online]. 2 (1), pp. 17–19.
- O’Kane, M.J., Wisdom, G.B., Desai, Z.R. and Archbold, G.P. (1994) Inhibition of fibrin monomer polymerisation by myeloma immunoglobulin. Journal of Clinical Pathology. 47 (3), pp. 266–268.
- Padmanabhan, A. et al. (2019) Guidelines on the Use of Therapeutic Apheresis in Clinical Practice - Evidence-Based Approach from the Writing Committee of the American Society for Apheresis: The Eighth Special Issue. Journal of Clinical Apheresis [online]. 34 (3), pp. 171–354.
- Palmer, R.N., Rick, M.E., Rick, P.D., Zeller, J.A. and Gralnick, H.R. (1984) Circulating heparan sulfate anticoagulant in a patient with a fatal bleeding disorder. The New England Journal of Medicine [online]. 310 (26), pp. 1696–1699.
- Powles, R., Smith, C., Kohn, J. and Hamilton Fairley, G. (1971) Method of removing abnormal protein rapidly from patients with malignant paraproteinaemias. British Medical Journal [online]. 3 (5776), pp. 664–667.
- Tan BL, Cleton FJ, van Beusekom GT, Veltkamp JJ, van Rood JJ. (no date) Plasmapheresis treatment of haemorrhagic complications in a patient with multiple myeloma. Folia Med Neerl 1967;10:174–9.
- Wallace, M.R., Simon, S.R., Ershler, W.B. and Burns, S.L. (1984) Hemorrhagic diathesis in multiple myeloma. Acta Haematologica [online]. 72 (5), pp. 340–342.