
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Peutz-Jeghers polyposis presenting with intussusception in a Nigerian male: A case report and management challenges in a resource-limited setting
Michael E Aghahowa1,2*; Okundayo Emuze3,4; Kevin N Ezike5,6; Kehinde Osisanya7,8; Damian I Okonkwo5,9; Bata M Gali1,2; Sunday I Atinko10; Emmanuel Oguntebi6
1Department of Surgery, College of Health Sciences, Nile University of Nigeria, Abuja, Nigeria.
2Department of Surgery, Asokoro District Hospital, Abuja, Nigeria.
3Department of Surgery, College of Health Sciences, Igbinedion University, Okada, Edo State, Nigeria.
4Department of Surgery, University of Benin Teaching Hospital, Benin City, Nigeria.
5Department of Anatomic Pathology & Forensic Medicine, Nile University of Nigeria, Abuja, Nigeria.
6Department of Anatomic Pathology & Forensic Medicine, Asokoro District Hospital, Abuja, Nigeria.
7Department of Surgery, College of Health Sciences, Baze University, Abuja, Nigeria.
8Department of Surgery, Maitama District Hospital, Abuja, Nigeria.
9Department of Anatomic Pathologic & Forensic Medicine, Maitama District Hospital, Abuja, Nigeria.
10Department of Surgery, National Hospital, Abuja, Nigeria.
*Corresponding Author : Michael E Aghahowa
Department of Surgery, College of Health Sciences, Nile University of Nigeria, Abuja, Nigeria.
Email: Michael.ehienagudia@nileuniversity.edu.ng
Received : Apr 03, 2025
Accepted : Apr 23, 2025
Published : Apr 30, 2025
Archived : www.jcimcr.org
Copyright : © Aghahowa ME (2025).
Abstract
Background: Peutz-Jeghers (P-J) syndrome is a rare autosomal dominant disease characterised by haematomata’s polyps involving the gastrointestinal tract and melanosis of the lips, mouth, or anus. Though mostly benign, these polyps can transform into cancers affecting the bowel, breast and cervix. Screening is important for early diagnosis and treatment. We report a case of P-J haematomata’s polyps involving the large bowel presenting with intussusception and the challenges with its management highlighted.
Case summary: A 33-year-old male, presents with hematochezia and features of acute large bowel obstruction due to intussusception with numerous pedunculated polyps of the entire colon. He had emergency total colectomy and ileorectal anastomosis. Histological examination of the resected intestines showed numerous harmatomatous polyps, consistent with P-J syndrome. He was lost to follow-up because of the need for colon cancer surveillance. P-J polyps commonly present with bleeding and intussusception. Although benign, adenomatous changes have been reported in the polyps and extra-colonic cancers commonly affect the small intestine, stomach, pancreas, ovary, lung, uterus, and breast. Treatment of Peutz-Jeghers syndrome is directed mainly at the complications such as intestinal obstruction, persistent bleeding or cancer. However, regular surveillance with colonoscopy for colonic cancer and, mammography and PAP’s smear for breast and cervical cancer screening respectively for females is advocated. These screening and surveillance modalities, cost as well as adequate personnel are a challenge for many centres in a resource-limited country.
Conclusion: A rare case of P-J syndrome affecting the entire large bowel is presented. Proper screening and surveillance of P-J syndrome patients can be challenging in resource-limited setting.
Keywords: Peutz-Jeghers; Haematomata’s polyps; Intussusception; Surveillance; Cancer.
Citation: Aghahowa ME, Emuze O, Ezike KN, Osisanya K, Okonkwo DI, et al. Peutz-Jeghers polyposis presenting with intussusception in a Nigerian male: A case report and management challenges in a resource-limited setting. J Clin Images Med Case Rep. 2025; 6(4): 3574.
Introduction
Puetz-Jaghirs (P-J) syndrome was first described by Hutchinson in 1896 but separate descriptions by Peutz in 1921 and Jaghirs in 1944 and 1049 later brought the condition to recognition [1,2]. It is a rare autosomal dominant-inherited disorder with a reported incidence of 1 in 100,000 individuals [3] and seen in males and females in equal proportion [4,5]. It is characterised by multiple hamartomata’s (benign tumour-like malformation resulting from faulty development in an organ) polyps in the small bowel and colon as well as melanosis of the mouth and lips (and sometimes of the digits and perianal skin) [6,7]. Melanin can also occur in the mucosa of the stomach and multiple small moles on the skin of the face and in the buccal mucous membrane [6]. Mutation of the Serine Threonine Kinase (STK11 D) tumour-suppressor gene on chromosome 19p13.3 has been found in 90% of patients with this condition [6,7]. The syndrome is associated with an increased (2% to 10%) risk for cancer of the intestinal tract [2].
Long-term follow-up of the original family described by Puetz showed reduced survival as a consequence of complications of bowel obstruction and the development of a range of cancers [5] affecting the bowel, breast and cervix, ovary, fallopian tubes, thyroid, lung, gallbladder, bile ducts, pancreas, and testicles. It is logical to perform regular colonic surveillance on all diagnosed patients using colonoscopy/enteroscopy and encourage female patients to attend breast and cervical cancer screening using mammography and PAP’s smear respectively [6]. Despite the increased risk of malignancy, malignant change in the polyps themselves rarely occurs and the polyps can be left alone unless they are the cause of symptoms like bleeding, obstruction or malignancy. Resection may be indicated however, for heavy and persistent or recurrent bleeding or intussusception. Polyps may be removed by enteroscopy or, at laparotomy, or snared through a colonoscope introduced via an enteroscopy. Heavily involved segments of small intestine may occasionally be resected [6]. The autosomal dominant pattern of inheritance has a high degree of penetrance. The classic pigmented lesions are small, 1-2 mm, and brown or black spots located in the circum-oral region of the face, buccal mucosa, forearms, palms, soles, digits, and perianal area [8]. The entire jejunum and ileum are the most usual portions of the gastrointestinal tract involved with these hamartomata’s polyps. However, 50% of patients may also have rectal and colonic lesions, and 25% of patients have gastric lesions. The small intestine represents the most frequent site for cancer compared with that of the general population [8].
Case presentation
A 33-year-old male, twin, presented with a one-week history of recurrent colicky, lower abdominal pains, constipation associated with post-prandial bilious vomiting and abdominal distension. There was also a mass which moved from the right to the left side of the lower abdomen. He had two episodes of passing dark stool (melena) and frank blood (hematochezia) per rectum a week before presentation. His only sibling is a male-twin, alive and well. His parents died from unknown causes. He denies any family history of cancer. On examination, he was ill-looking, dehydrated but not pale. The abdomen revealed a mobile 6 cm x 10 cm palpable, tender mass in the right iliac fossa. A digital rectal examination was unremarkable. A Computed Tomography (CT) scan of the abdomen showed a mass in the right iliac fossa with telescoping of the ileum into the ascending colon, and numerous intra-luminal colonic masses of varying sizes. A diagnosis of large bowel obstruction due to ileo-colic intussusception from polyposis was made. His full blood counts, liver function tests, serum electrolytes and urea levels were normal. He had an emergency exploratory laparotomy and findings were reduced viable ileo-colic intussusception, multiple and palpable intra-luminal firm, discreet masses spread along the terminal ileum (15 cm from ileocecal junction) and up to the sigmoid colon. He had total colectomy and ileo-rectal anastomosis. He had watery diarrhoea (5-6 times daily) from the 3rd postoperative day for 4 days which was controlled with oral loperamide and CocodamolRX. The gross pathologic findings were multiple variable-sized polypoid masses (mostly pedunculated and a few sessile), in the lumen of both the terminal ileum, base of the appendix and the entire large intestine. The largest polyp measures 4.5 cm x 3.5 cm x 3 cm while the smallest was 0.2 cm x 0.1 cm x 0.1 cm (Figure 1).
There were 36 enlarged lymph nodes in the mesocolon harvested and they showed features of reactive hyperplasia. A histological diagnosis of Peutz-Jeghers haematomata’s polyps was made. He was discharged home on the 8th postoperative day in satisfactory condition and scheduled for follow-up at the outpatient clinic in 6 weeks with his twin brother for both of them to have proctoscopy and enteroscopy but he never honoured the appointment. Multiple phone calls to convince him were unsuccessful as patient kept saying he was fine. He was therefore lost to follow-up.

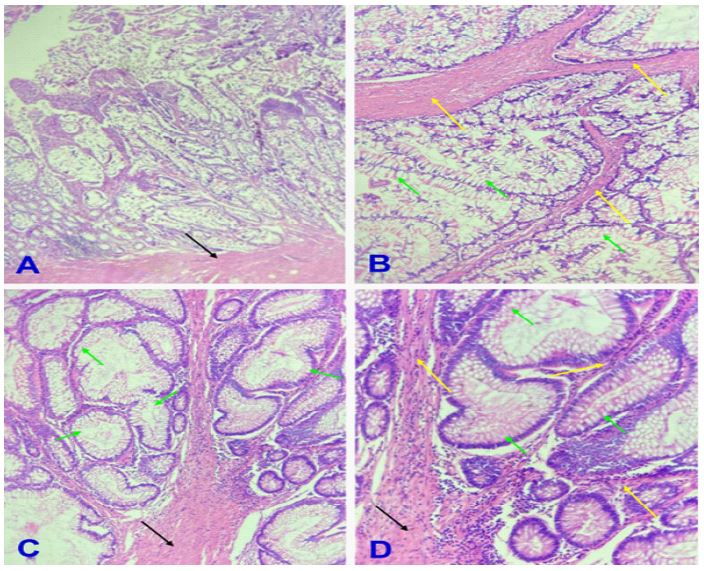
Legend: (A) Note papillary architecture with arborizing streaks of smooth muscle fibers anchored off the muscularis mucosa (black arrow) and fanning out (H&E x40); (B) Note streaks and trabeculae of smooth muscle fibers (yellow arrows) coursing through the variably sized and shaped hyperplastic, goblet-cell rich, colonic-type glands (green arrows), demarcating them into lobules (H&E x100); (C) Note broad band of smooth muscle fibers (black arrow) splitting into smaller bands and coursing through the variably sized and shaped hyperplastic, goblet-cell rich, colonic-type glands (green arrows) closely packed together (H&E x200); (D) Note broad band of smooth muscle fibers with infiltrates of lymphocytes (black arrow) splitting into smaller bands (yellow arrows) and coursing through the variably sized and shaped hyperplastic, goblet-cell rich, colonic-type glands (green arrows) closely packed together (H&E x400)
Discussion
Hamartomata’s polyps of the small and large bowel occur as part of Peutz-Jeghers syndrome, which is an inherited syndrome of mucocutaneous melanotic pigmentation and gastrointestinal polyps. The most common symptom is recurrent colicky abdominal pain because of intermittent intussusception and associated with a palpable mass reported in one-third of patients [8]. Bleeding as a result of auto-amputation of the polyps occurs less frequently and most commonly manifest by anemia. Our patient presented with a recurrent history of colicky abdominal pain, Gastrointestinal (GI) bleeding (hematochezia and melena) and acute intestinal obstruction due to intussusception as demonstrated by a tender abdominal mass which is consistent with the typical presentation of P-J syndrome and confirmed with a CT abdomen. According to the WHO, diagnosis of P-J syndrome is clinched with one or more of these four criteria [9].
a) Three or more P-J polyps confirmed on histology.
b) Any number of P-J polyps with a positive family history.
c) Prominent and characteristic mucocutaneous pigmentation.
d) Any number of P-J polyps and characteristic mucocutaneous pigmentation.
Even though our patient did not have the typical lentigines on the skin or mucous membranes associated with P-J syndrome, his numerous haematomata’s polyps on histology meet the first WHO criterion of three or more P-J polyps confirmed on histology and also supports a previous case by Oluyemi et al. [10], where only solitary GI (gastric, small intestinal, and colorectal) harmotomes polyps that are histologically similar to those of the P-J syndrome type without the typical mucocutaneous lesions or family history of P-J syndrome was reported. Our patient had both macroscopic and microscopic features of severe P-J haematomata’s polyposis as shown in (Figures 1) and 2 above. The treatment of Peutz-Jeghers haematomata’s polyps is directed mainly at the complication of persistent bleeding or intestinal obstruction. Resection is limited to the segment of bowel involved in the complications. Even though cure is said to be impossible because of the widespread nature of intestinal involvement thus extensive resections are not indicated as reported in literature [8], our patient had an emergency total colectomy and ileorectal anastomosis because of the recent history of recurrent hematochezia and the widespread nature of long intestinal involvement of polyposis (from terminal ileum, appendix, caecum to the sigmoid colon), complicated by intestinal obstruction (intussusception). We are yet to ascertain if this surgery provided a long-term cure for the patient. The polyps of Peutz-Jeghers syndrome are considered to be hamartomas and are not at significant risk for malignant transformation. However, carcinoma may occasionally develop. Although once considered a purely benign disease, adenomatous changes have been reported in 3% to 6% of hamartomas. There were no adenomatous changes demonstrated in all the polyps of our patient on histology. Similarly, extra-colonic cancers are said to be common, occurring in 50% to 90% of patients (small intestine, stomach, pancreas, ovary, lung, uterus, and breast) [8]. We could not ascertain if our patient had any extra-colonic cancer. However, there was no atypia or evidence of malignancy on the histological examination of all the resected intestinal specimens including all the polyps. Screening for cancer consists of a baseline colonoscopy and upper GI endoscopy at age 20 years, followed by annual flexible sigmoidoscopy thereafter [11]. Whereas the traditional enteroscopy (small bowel endoscopy) is a simple technique with wide availability using a paediatric colonoscope, performed under sedation and can only access proximal small bowel, the video-capsule endoscopy is able to visualise the entire small bowel, preferable for patients because no sedation is required and it is painless. However, single/double balloon enteroscopy is able to visualise the entire small bowel with a full range of therapeutic benefits [10]. Both enteroscopy and colonoscopy would have been performed by us to examine the small bowel during the surgery but these were not available. Genetic screening for Serine Threonine Kinase (STK11 D) on chromosome 19 which has been found in 90% of patients [12] with this condition was also not done in our patient because these investigating tools are not available even though the patient was lost to follow-up. This has reduced our ability to detect any complication of P-J haematomata’s polyps such as cancer through surveillance after surgery. Our patient could not be screened for any possible cancer and genetic studies were not done because he did not honour the follow-up appointments and when contacted severally on phone, he claimed his twin brother and he were well and they will not submit themselves for further clinical evaluations. Moreover, they could not afford the cost of further surveillance. Thus, poor health education and inability to afford cost of healthcare in a resource-limited setting as demonstrated by our patient pose a great challenge to the necessary surveillance for patients with P-J syndrome and their immediate family members.
Conclusion
This presents a rare form of P-J haematomata’s polyps affecting a large segment of the ileum and the entire colon with the typical features of bleeding, intestinal obstruction from intussusception and without the typical hyperpigmented oral or skin changes. The opportunity for either intraoperative screening or postoperative surveillance with enteroscopy and genetic screening of both the patient and his family member using Serine Threonine Kinase (STK 11D) were missed due to the unavailability of capacity and loss of patient to follow-up. This poses a great challenge in our resource-limited setting. There is the need to improve funding through insurance scheme and health education in order to achieve better yield for cancer surveilsurveillance and treatment outcomes for patients with P-J syndrome.
Declarations
Acknowledgement: We are grateful to the management of Asokoro District Hospital, Abuja for allowing us have access to the records of this patient.
Financial support and sponsorship: None.
Conflict of interest: None
Patient’s consent: The authors obtained consent from the patient to publish this case.
References
- Meles M, El-Bakary T, El-Gendy M, Darwish A. Adult Intussusception in Patients with Peutz-Jeghers Syndrome: Case Series and Review of Literature. 2017; 8: 118-132. doi: 10.4236/ss.2017.82014.
- Mahmoud NN, Bleier JIS, Aarons CB, Carter Paulson E, Shanmugan S, et al. Colon and Rectum In: CM Townsend, RD Beauchamp, BM Evers and KL Mattox. (Eds). Sabinston’s Textbook of Surgery. The Biological Basis of Modern Surgical Practice 20th Ed. Philadelphia: Elsevier Saunders. 2017; 1372.
- Syaiful RA, Supit C, Putrato AS. A case of ileocolic intussusception in an adult with Peutz-Jeghers syndrome. Int J. Surg. 2018; 1(2): 110.
- Pedersen IR, Hartvigsen A, Hansen BF, Toftgaard C, Konstantin-Hansen K, et al. Management of Peutz-Jeghers syndrome. Experience with patients from the Danish Polyposis Register. Int J Colorectal Dis. 1994; 9(4): 177-9. doi:10.1007/BF00292244.
- Bartholomew LG, Moore CE, Dahlin DC, Waugh JM. Intestinal polyposis associated with mucocutaneous pigmentation. Surg Gynecology Obstet. 1962; 115: 1-11.
- Calson GL and Soop M. The Small Intestine. In: NS Williams, PR O’Connell and AW McCaskie. (Eds). Bailey and Love’s Short Practice of Surgery. 27th Ed. Florida: CRC Press. 2018; 1233: 1250-1284.
- Jaghirs H, Mckusick VA, Katz KH. Generalised intestinal polyposis and melanin spots of the oral mucosa, lips and digits; a syndrome of diagnostic significance. N Engl J Med. 1949; 241(26): 1031-6. doi: 10.1056/NEJM194912292412601.
- Harris JW, Evers BM. Small Intestine In: CM Townsend, RD Beauchamp, BM Evers and KL Mattox. (Eds). Sabinston’s Textbook of Surgery. The Biological Basis of Modern Surgical Practice. 20th Ed. Philadelphia: Elsevier Saunders. 2017; 1271.
- Bosman FT, Carneiro F, Hruban RH, Theise ND, editors. WHO. Classification of Tumors of the Digestive System. 4th Ed. Lyon, France: International Cancer Research on Cancer. 2010.
- Oluyemi AO, Odeghe EA, Awolola NA. Solitary Peutz-Jeghers type hamartoma in a Nigerian: A case report of a rare finding and review of literature. Ann Afr Med 2021; 20(4): 307-309 doi: 10.4103/aam.aam_37_20.
- Lindsay JO, Woodland P. Gastrointestinal endoscopy. In: NS Williams, PR O’Connell and AW McCaskie. (Eds). Bailey and Love’s Short Practice of Surgery. 27th Ed. Florida: CRC Press. 2018; 225-227.
- Harbaum L, Geigl JB, Volkholz H, Schwarzbraun T, Oschmautz H, et al. Sporadic gastric Peutz-Jeghers polyp with intraepithelial neoplasia. APMIS. 2009; 117(12): 941-3. doi: 10.1111/j.1600-0463.2009.02549.x.