
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Commentary - Open Access, Volume 6
Echogenicity patterns in amniotic fluid: Indicator of fetal well being
Sachin SK1; Archiya Habib2*; Sana S2; Aniket AC2; Mameeza A2
1Professor and Head of Department Radiodiagnosis, Era’s Lucknow Medical College and Hospital, Lucknow, Uttar Pradesh, India.
2Junior Resident, Department of Radiodiagnosis, Era’s Lucknow Medical College and Hospital, Lucknow, Uttar Pradesh, India.
*Corresponding Author : Archiya Habib
Junior Resident, Department of Radiodiagnosis, Era’s Lucknow Medical College and Hospital, Lucknow, Uttar Pradesh, India.
Email: drarchiyahabib@gmail.com
Received : Apr 05, 2025
Accepted : Apr 25, 2025
Published : May 02, 2025
Archived : www.jcimcr.org
Copyright : © Habib A (2025).
Abstract
Background: A highly dynamic and complicated system, the Amniotic Fluid (AF) is analysed as a data point to interpret the health of the fetus. Echogenic amniotic fluid is a rare finding that is caused by the presence of particles in the fluid. Vernix caseosa, blood and meconium have all been implicated as the cause of echogenic liquor. The purpose of the current study was to determine the importance of echogenicity of the amniotic fluid in predicying the fetal outcome.
Methods: From January 2023 to August 2024, the Department of Radiodiagnosis, carried out a prospective observational study. The study comprised 35 patients in total who showed ultrasonographic signs of echogenic liquor. To ascertain the foetal outcome, they were monitored till delivery. The Appearance, Pulse, Grimace, Activity, and Respiration (APGAR) score, Neonatal Intensive Care Unit (NICU) admission rate, and stillbirth rate were used to examine the foetal outcome.
Result: A study of 35 participants found that 22 had vernix caseosa, 7 had meconium-stained liquor, 4 had blood-stained liquor, and 2 had clear liquor. Meconium and blood-stained liquor was associated with negative outcomes.
Conclusion: According to our research, when echogenic amniotic fluid is encountered, a suitable workup should be done to determine the underlying cause because these deviations from normal can occasionally result in poor outcome. Ultrasonography is unable to accurately distinguish meconium in amniotic fluid from other causes of echogenicity. It significantly affects the fetal fate if meconium and blood can be accurately recognized during pregnancy. Hence, discovery of hyperechogenic amniotic fluid alone does not warrant a change in the way pregnancy is managed.
Keywords: Amniotic fluid; Echogenic liquor; Ultrasonography; Meconium; Fetal outcome.
Citation: Sachin SK, Habib A, Sana S, Aniket AC, Mameeza A. Echogenicity patterns in amniotic fluid: Indicator of fetal well being. J Clin Images Med Case Rep. 2025; 6(5): 3576.
Introduction
The aquatic environment of the fetus has long remained an enigma to the patient and their obstetricians. Amniotic fluid, produced by the amnion, is crucial for the embryo’s early development. It protects the fetus from trauma and desiccation, reflecting life’s aquatic origins. Adequate amniotic fluid is essential for normal fetal growth, cushioning against trauma, preventing infection, and providing nutrients. It also allows for proper skeletal development, promotes lung growth, and helps prevent umbilical cord compression. Amniotic Fluid (AF) is mainly formed from fetal plasma volume, fetal urine, fetal respiratory system, gastrointestinal tract, umbilical cord, and fetal surface of the placenta. The composition of the AF changes with the gestational age with an average pH of 7.2 and specific gravity of 1.0069-1.008. The echogenicity of AF indirectly represents the size, number, and distribution of particles in AF and in turn turbidity of AF. This could give rise to the ultrasound detection of echogenic particles, also known as AF sludge or appearance of a homogeneously echogenic AF. AF “sludge” is dense aggregates of particulate matter. In the first‐ and second‐trimester ultrasound imaging, the presence of such particulate matter in AF is seen in approximately 4%. Prior research has indicated that the presence of high-density intra-amniotic particles may be associated with vernix caseosa, intraamniotic bleeding, and meconium [1-3]. By the third trimester, the incidence rises to about 80% and has been mainly attributed to the presence of vernix caseosa and/or meconium. Vernix caseosa is a complex fatty substance derived from the desquamated epithelial cells and sebaceous material [4]. Congenital conditions associated with particulate matter in the AF include harlequin ichthyosis and epidermolysis bullosa legalism. Presence of meconium in amniotic fluid is associated with an increased risk of fetal asphyxia [5] and hence its detection is important. Ultrasound offers a non-invasive alternative for detecting meconium during the antepartum period, unlike current methods such as amniocentesis, angioscopy, or amniotomy, which are invasive. This non-invasive technique would be advantageous for perinatologists. Benacerraf et al. stated that the ultrasound diagnosis of meconium-stained amniotic fluid could be made if the following criteria are met: (a) a diffuse echogenic pattern throughout the amniotic cavity, (b) a clear contrast between the amniotic fluid and the umbilical vessels, and (c) layering in the more dependent areas. Homogeneously, echogenic AF is due to the presence of innumerable echogenic particles in the fluid and is an uncommon finding. In most cases, this is due to the presence of vernix caseosa in AF; however, in minority of cases, this could be due to meconium or blood (Figures 2-5). The ultrasound diagnosis of echogenic or meconium AF could be made if the following criteria are met:
1. Diffuse echoes within the amniotic cavity.
2. Clear contrast between the AF and the umbilical vessels. Normally, there is no clear contrast between clear/ anechoic liquor and anechoic lumen of the umbilical vessels. In the presence of echoes within liquor, there is a contrast between echogenic liquor and anechoic lumen of vessels.
3. Layering in the more dependent areas of the uterus.
4. Thus, it appears prudent to evaluate AF during any assessment of fetal status whether as a part of the antenatal testing protocol or in the labor suite.
Material and methods
A prospective study was conducted in the Department of Radiology at a tertiary center, from January 2023 to August 2024. A total of 35 pregnant women with gestational age between 37 weeks and 39 weeks without any medical and obstetric complications were enrolled in the study with ultrasonographic evidence of echogenic liquor. History and examination details were noted. All necessary Antenatal Checkup (ANC) investigations, nonstress tests, and ultrasound examinations were done to see the fetal well‐being, congenital anomalies, AF index, and echogenicities in liquor. The patients were delivered either vaginally or by a cesarean section and were followed till 7 days after delivery. The condition of babies was assessed by the Appearance, Pulse, Grimace, Activity, Respiration (APGAR) score at birth, need for neonatal Neonatal Intensive Care Unit (NICU) admissions, and stillbirths.
Inclusion criteria
1. Patients who were sure of their last menstrual period.
2. Gestational age between 37 and 39 weeks.
3. Singleton pregnancy
4. Amniotic Fluid Index (AFI) between 8 cm and 15 cm.
5. Normal fetal doppler indices.
Exclusion criteria
1. Gestational age <37 weeks and >39 weeks.
2. Oligohydramnios or polyhydramnios.
3. Multiple gestation.
4. Any medical or obstetric complication of pregnancy.
5. Congenital anomaly in the fetus.
Results
The present study was undertaken to study the outcome of term pregnancy with echogenic Amniotic Fluid. Out of 35 participants, 22 participants had vernix caseosa, 7 had meconium‐stained liquor, 4 had blood‐stained liquor, and 2 had clear liquor. Out of 22 participants with vernix, all fetuses had APGAR score >7/10 with no NICU admission and no stillbirth. Vernix was associated with positive fetal outcome (APGAR values >7/10) (P<0.01). Out of seven participants with meconium, one baby had APGAR score >7/10 and three babies had APGAR score <7/10, out of which two had NICU admission, and there was one stillbirth. Meconium was associated with negative fetal outcome (APGAR values <7/10) (P<0.01). Out of four participants with blood‐stained liquor, two babies had APGAR score >7/10 and two babies had APGAR score <7/10, out of which two had NICU admissions and there was no stillbirth. Two patients with blood‐stained liquor had marginal placental site abruption, one had evidence of scar dehiscence, and in one case, we found no cause for blood‐stained liquor.
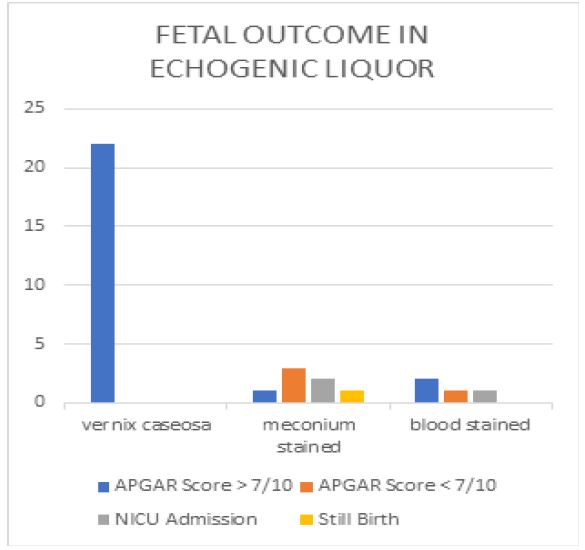




Table 1: Fetal outcome based on liquor characteristics.
| Liquor characteristic | APGAR>7/10 | APGAR<7/10 | NICUAdmissions | Still births |
|---|---|---|---|---|
| Vernix Caseosa | 22 | 0 | 0 | 0 |
| Meconium- Stained Liquor | 1 | 3 | 2 | 1 |
| Blood-Stained Liquor | 2 | 2 | 2 | 0 |
| Clear Liquor | 2 | 0 | 0 | 0 |
Conclusion
According to our research, the presence of echogenic particles in the amniotic fluid is a result of various causes. Vernix caseosa is one of the most common causes of echogenicity in the amniotic fluid with favourable outcome. In a small percentage of cases, meconium or blood may be the cause of echogenicity of the amniotic fluid. It is advised that direct visualization of amniotic fluid by amniocentesis or amnioscopy to be done since meconium or blood stained liquor cannot be ruled out by ultrasonography. Fetal monitoring by non-stress test and/or biophysical profile provide added information about fetal wellbeing.
References
- Karamustafaoglu Balci B, Gaymer G. Incidence of echogenic amniotic fluid at term pregnancy and its association with meconium. Archives of gynecology and obstetrics. 2018; 297: 915-8.
- Elsabe AH, Atef AM, Salama DN, Abdallah LM, Saada SM. Sonography Assessment of Amniotic Fluid Volume as a Predictor of Fetal Outcome in Low-Risk Pregnancy. The Egyptian Journal of Hospital Medicine. 2022; 88(1): 3022-8.
- El Darwish AE, Abdallah KM, Suliman HI. Clinical Significance of Echogenic Amniotic Fluid on Perinatal Outcome. Al-Azhar International Medical Journal. 2024; 5(9): 12.
- Posh, Sheema; Rafiq, Suhail1; Dar, Musaib Ahmad1; Aslam, Rasiq1; Bhat, Shabir Ahmad1. Role of Amniotic Fluid Echogenicities in the Prediction of Fetal Outcome. Journal of the Scientific Society. 2020; 47(1): 33-36. DOI: 10.4103/jss.JSS_9_20.
- Shrestha S, Bhandary S, Dwa Y, Jaiswal P, Parmar B, Karki DB. Echogenic liquor at term pregnancy on ultrasonography is not always meconium. Journal of Patan Academy of Health Sciences. 2017; 4(1): 7-11.