
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 6
Accelerated idioventricular rhythm post primary angioplasty in myocardial infarction: Two sides of the coin
Amanpreet Singh Wasir1; Jagroop Doad2*; Ravi Kalra3; Prashant Bharadwaj4
1Bharati Vidyapeeth (Deemed to be University) Medical College and Hospital, Pune, Maharashtra, India.
2Department of Internal Medicine, Campbell University School of Medicine, Lillington, NC, USA.
3Professor and Head, Department of Cardiology, Bharati Hospital and Research Centre, Pune, Maharashtra, India.
4Professor, Department of Cardiology, Bharati Hospital and Research Centre, Pune, Maharashtra, India.
*Corresponding Author : Jagroop Doad
Department of Internal Medicine, Campbell University School of Medicine, Lillington, NC, USA.
Email: j_doad0916@email.campbell.edu
Received : Apr 07, 2025
Accepted : Apr 28, 2025
Published : May 05, 2025
Archived : www.jcimcr.org
Copyright : © Doad J (2025).
Abstract
Accelerated Idioventricular Rhythm (AIVR) is a ventricular ectopic rhythm commonly observed during Acute Myocardial Infarction (AMI), often seen as a marker of successful revascularization. The occurrence of AIVR post-successful primary angioplasty has not been well described in terms of its time course and associated symptoms, leaving the underlying threat of a potential re-occlusion. We present two patients who developed AIVR following successful primary angioplasty and subsequently became symptomatic again with AIVR at varied intervals. Electrocardiogram (ECG) is useful in establishing the diagnosis of AIVR; however, limited data are available on the clinical presentation of AIVR. This challenge is further complicated by the overlapping occurrence rates of AIVR and Ventricular Tachycardia (VT), necessitating a personalized interdisciplinary approach.
Keywords: Accelerated idioventricular rhythm; Ventricular arrhythmia; Electrophysiology.
Abbreviations: AIVR: Accelerated Idioventricular Rhythm; AMI: Acute Myocardial Infarction; ECG: Electrocardiogram; VT: Ventricular Tachycardia; IRA: Infarct-Related; STEMI: ST- Segment Elevation Myocardial Infarction; TTE: Transthoracic Echocardiogram; TIMI: Thrombolysis in Myocardial Infarction; LAD: Left Anterior Descending Artery; RCA: Right Coronary Artery; LVEF: Left Ventricular Ejection Fraction.
Citation: Wasir AS, Doad J, Kalra R, Bharadwaj P. Accelerated idioventricular rhythm post primary angioplasty in myocardial infarction: Two sides of the coin. J Clin Images Med Case Rep. 2025; 6(5): 3577.
Introduction
Accelerated Idioventricular Rhythm (AIVR) defined as a ventricular ectopic rhythm with more than 3 consecutive beats at a rate between 50 and 120 beats/minute [1,2], indicates successful reperfusion in Acute Myocardial Infarction (AMI) with thrombolytic drugs. Ventricular Tachycardia (VT) is also another ventricular ectopic rhythm with a rate greater than 100 beats/minute which indicates ischemia. There is an overlap in the rates of these two rhythms between 100 to 120 beats/minute. The occurrence of AIVR post-successful primary angioplasty is not well described with respect to the time course and associated symptoms. We present two cases of AIVR occurring post-successful primary angioplasty, where patients became re-symptomatic with the development of AIVR ranging at intervals from 6-12 hours. A repeat coronary angiography showed no change in the Infarct-Related Artery (IRA) from the post-procedure outcome. The rhythm subsided spontaneously after approximately an hour’s duration in both these cases, however when AIVR occurs after a significant time following PCI, there is a risk of re-occlusion of the IRA.
Case presentations
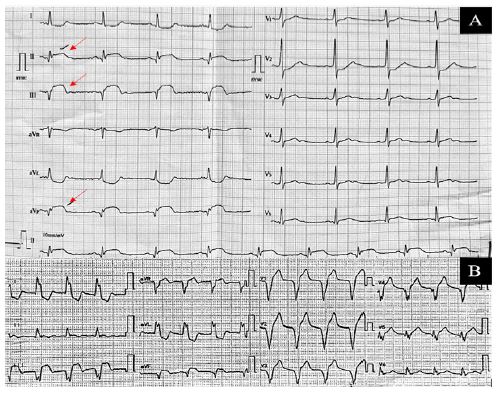
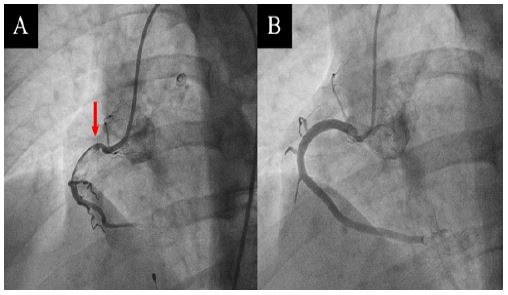
Case 1: Patient X, a 26-year-old male and non- smoker, presented with anginal chest pain for 6 hours associated with diaphoresis. He had no history of drug habituation or cardiac family history. ECG revealed inferior wall ST- Segment Elevation Myocardial Infarction (STEMI) (Figure 1A) and a Transthoracic echocardiogram (TTE) showed inferior wall hypokinesia with Left Ventricular Ejection Fraction (LVEF) of 50%. Troponin-T level was 0.68 ng/mL (reference range: positive >0.01 ng/mL). A decision was made for the patient to undergo primary angioplasty which showed 99% thrombotic occlusion of the proximal Right Coronary Artery (RCA) (Figure 2A). Thrombus aspiration was performed using a thrombus aspiration catheter. Post-aspiration, there was no significant culprit lesion and the RCA showed Thrombolysis in Myocardial Infarction (TIMI)- grade 3 flow (Figure 2B). Twelve hours post-procedure, the patient again developed anginal chest pain with recurrent episodes of vomiting. On re-examination a pericardial rub was appreciated, ECG showed AIVR with a heart rate of 114/minute (Figure 1B) but no new echocardiographic findings. A repeat coronary angiogram displayed no change in flow of the IRA from the final post-procedure angiogram. The rhythm lasted an hour with spontaneous conversion to sinus rhythm within an hour.
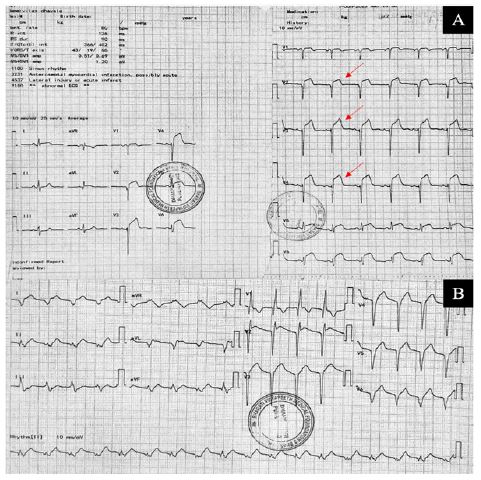
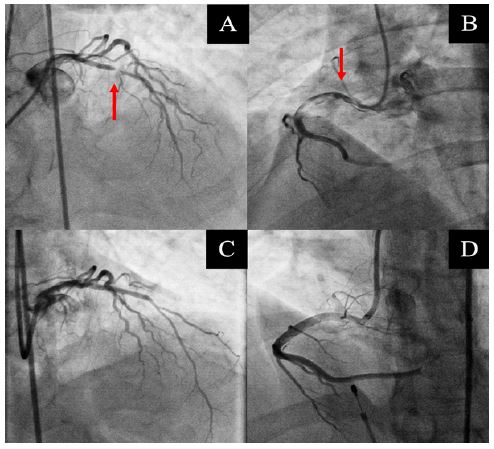
Case 2: Patient Y, a 67-year-old male and non- smoker, presented with anginal chest pain for 10 hours associated with diaphoresis and dyspnea. ECG revealed anteroseptal STEMI (Figure 3A). Echocardiography demonstrated mid and distal septal hypokinesia with an LVEF of 35%. Troponin-T level was elevated at 1.12 ng/mL. The patient was taken for primary angioplasty which showed 99% discrete stenosis of the proximal left anterior descending artery (LAD) (Figure 4A and B). He underwent PCI and LAD stent implantation (TRUCOR ONYXTM– 2.75x22 mm) with successful reperfusion (Figure 4C and 4D). Six hours post procedure, the patient developed anginal chest pain accompanied by recurrent episodes of vomiting. On re-examination, ECG showed AIVR with a rate of 110/minute (Figure 3B), with no new echocardiographic findings. A repeat coronary angiogram displayed no change from the post-procedure angiogram in the IRA. The rhythm lasted half an hour with spontaneous conversion to sinus rhythm.
Discussion/conclusion
AIVR is a common arrhythmia often observed during reperfusion therapy in AMI. In the current thrombolytic era, the prevalence of AIVR after successful reperfusion is between 25-90% in STEMI patients [3,4]. However, in patients with 100% successful mechanical reperfusion in STEMI, the prevalence of AIVR occurrence was extremely low, ranging between 12-18% [5-7]. The cause of this varied prevalence can be attributed to the distinct demography of patients, different diagnostic criteria of AIVR, various imaging techniques of coronary artery visualization, and importantly different reperfusion modalities [5]. In terms of pathophysiology, AIVR is thought to be caused because of the sudden influx of blood, oxygen, and chemical mediators during reperfusion of ischemic myocardial tissue [8]. This state also results in transient alterations in the cell membrane potential and ionic gradients which lead to increased automaticity of the ventricular myocardium, thereby potentiating AIVR [9]. Clinically, AIVR during reperfusion is often considered a marker of successful revascularization, but its prognostic significance is debated. While some studies associate AIVR with a larger infarct size in AMI [10,11], others suggest that it may indicate successful thrombolysis, especially when occurring within two hours after a streptokinase infusion [12,13]. Most patients are asymptomatic, however, some may experience palpitations, syncope, or dizziness [14]. Management of AIVR in the acute setting typically involves close monitoring and continuous telemetry. Guideline-directed anti-arrhythmic therapy is generally not warranted in these patients due to the benign nature of AIVR. However, if AIVR leads to sustained VT or hemodynamic instability, further interventions may be considered. In such cases, the focus should be on optimizing post- AMI care and managing comorbidities to improve patient outcomes. Another important aspect is the paucity of data on the clinical presentation and timing of AIVR, particularly due to the overlap in rates of AIVR and VT between 100-120 beats/minute. AIVR typically occurs shortly after PCI, with a study reporting that 42% of patients experience it within the first 90 minutes [10]. While VT typically serves as an indicator of myocardial ischemia, AIVR on-the-other-hand is classically associated with successful reperfusion. This electro- diagnostic conundrum may indicate more extensive myocardial damage and delayed microvascular perfusion, if not diagnosed and managed appropriately [10]. A holter-monitor study of 40 post-PCI AIVR patients observed asymptomatic episodes at a heart rate of less than 100 beats/minute within five hours [5,13]. However, AIVR occurring beyond 6-12 hours of reperfusion, especially at rates greater than 100 beats/minute and with recurrence of pain raises concerns for potential re-occlusion. The delayed presentation, associated symptoms, and heart rates in the VT zones are rare and noteworthy aspects of these two cases. Future research should fofocus on the clinical characteristics and prognostic implications of post- AMI patients presenting with atypical features associated with AIVR.
Acknowledgements: The authors gratefully acknowledge the contribution of the patients, who consented for their clinical report findings to be documented and published in medical literature.
References
- Marriott HJ, Menendez MM. A-V dissociation revisited. Prog Cardiovasc Dis. 1966; 8: 522-538. doi: 10.1016/s0033-0620(66)80014-2.
- Grimm W, Hoffmann J, Maisch B. [Accelerated idioventricular rhythm]. Z Kardiol. 1994; 83: 898-907.
- Pop T, Erbel R, Treese N, von Olshausen K, Meyer J. [Incidence and kind of reperfusion arrhythmias in thrombolytic therapy of acute myocardial infarct]. Z Kardiol. 1987; 76: 81-85.
- Cercek B, Lew AS, Laramee P, Shah PK, Peter TC, et al. Time course and characteristics of ventricular arrhythmias after reperfusion in acute myocardial infarction. Am J Cardiol. 1987; 60: 214-218. doi: 10.1016/0002-9149(87)90216-5.
- Bonnemeier H, Ortak J, Wiegand UK, Eberhardt F, Bode F, et al. Accelerated idioventricular rhythm in the post-thrombolytic era: incidence, prognostic implications, and modulating mechanisms after direct percutaneous coronary intervention. Ann Noninvasive Electrocardiol. 2005; 10: 179-187. doi: 10.1111/j.1542-474X.2005.05624.x.
- Yoshida Y, Hirai M, Yamada T, Tsuji Y, Kondo T, et al. Antiarrhythmic efficacy of dipyridamole in treatment of reperfusion arrhythmias: Evidence for cAMP-mediated triggered activity as a mechanism responsible for reperfusion arrhythmias. Circulation. 2000; 101: 624-630. doi: 10.1161/01.cir.101.6.624.
- Ophuis AJ, Bär FW, Vermeer F, Janssen W, Doevendans PA, et al. Angiographic assessment of prospectively determined non-invasive reperfusion indices in acute myocardial infarction. Heart. 2000; 84: 164-170. doi: 10.1136/heart.84.2.164.
- Heck-Swain KL, Koeppen M. The Intriguing Role of Hypoxia-Inducible Factor in Myocardial Ischemia and Reperfusion: A Comprehensive Review. J Cardiovasc Dev Dis. 2023; 10. doi: 10.3390/jcdd10050215.
- Riera AR, Barros RB, de Sousa FD, Baranchuk A. Accelerated idioventricular rhythm: history and chronology of the main discoveries. Indian Pacing Electrophysiol J. 2010; 10: 40-48.
- Terkelsen CJ, Sørensen JT, Kaltoft AK, Nielsen SS, Thuesen L, et al. Prevalence and significance of accelerated idioventricular rhythm in patients with ST-elevation myocardial infarction treated with primary percutaneous coronary intervention. Am J Cardiol. 2009; 104: 1641-1646. doi: 10.1016/j.amjcard.2009.07.037.
- Majidi M, Kosinski AS, Al-Khatib SM, Lemmert ME, Smolders L, et al. Reperfusion ventricular arrhythmia ‘bursts’ predict larger infarct size despite TIMI 3 flow restoration with primary angioplasty for anterior ST-elevation myocardial infarction. Eur Heart J. 2009; 30: 757-764. doi: 10.1093/eurheartj/ehp005.
- Khan A, Nadeem S, Kokane H, Thummar A, Lokhandwala Y, et al. Is accelerated idioventricular rhythm a good marker for reperfusion after streptokinase? Indian Heart J. 2016; 68: 302-305. doi: 10.1016/j.ihj.2015.09.023.
- Gressin V, Louvard Y, Pezzano M, Lardoux H. Holter recording of ventricular arrhythmias during intravenous thrombolysis for acute myocardial infarction. Am J Cardiol. 1992; 69: 152-159. doi: 10.1016/0002-9149(92)91295-f.
- MacLellan-Tobert SG, Porter CJ. Accelerated idioventricular rhythm: a benign arrhythmia in childhood. Pediatrics. 1995; 96: 122-125.