
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Cannabis triggered acute myocardial infarction leading to acute limb ischemia: A case report
Deepak R1; Vineeth Chandran KP2; Ahammed Shaheem PT3*; Vaishnavi T1; Rajeesh R1
1Department of Emergency Medicine, Malabar Medical College, Kozhikode, India.
2Department of Emergency Medicine, All India Institute of Medical Sciences, New Delhi, India.
3Department of Emergency Medicine, PK Das Institute of Medical Sciences, Palakkad, India.
*Corresponding Author : Ahammed Shaheem PT
Department of Emergency Medicine, PK Das Institute of Medical Sciences, Palakkad, India.
Received : Apr 08, 2025
Accepted : Apr 29, 2025
Published : May 06, 2025
Archived : www.jcimcr.org
Copyright : © Shaheem PTA (2025).
Abstract
Acute limb ischemia is defined as any sudden decrease in limb perfusion, which threatens both limb viability and mortality. Acute limb ischemia with concomitant acute myocardial infarction with left ventricular thrombus in a young male without any comorbidities is rare. Cannabis use has been associated with acute myocardial infarction. We report the case of a 29-year-old male with no known comorbidities who presented with acute onset bilateral lower limb weakness and numbness. He was diagnosed with acute bilateral lower limb ischemia due to infrarenal aortic occlusion, along with a concomitant acute myocardial infarction and a left ventricular thrombus. The patient reported cannabis use the day prior to symptom onset. Despite a multidisciplinary management approach, the outcome was unfavorable.
Keywords: Acute limb ischemia; Myocardial infarction; Left ventricular thrombus; Cannabis; Thromboembolism.
Citation: Deepak R, Chandran KPV, Shaheem PTA, Vaishnavi T, Rajesh R. Cannabis triggered acute myocardial infarction leading to acute limb ischemia: A case report. J Clin Images Med Case Rep. 2025; 6(5): 3580.
Introduction
Acute limb ischemia is an emergency condition requiring early recognition and rapid therapy [1]. Acute myocardial infarction among young is relatively uncommon [2]. Left ventricular thrombus is a known complication of myocardial infarction. Left ventricular thrombus can also lead to systemic thromboembolic events causing threatening limb ischemia [3]. Cannabis is considered as a risk factor for coronary thrombosis from literatures even though the exact role of this drug is not known [4,5]. Here discussing a case of young male without significant comorbidities who presented with acute bilateral lower limb ischemia with occlusion in large arteries resulted from concurrent myocardial infarction with left ventricular thrombus. He also gives a history of cannabis use on the day of symptom onset.
Case presentation
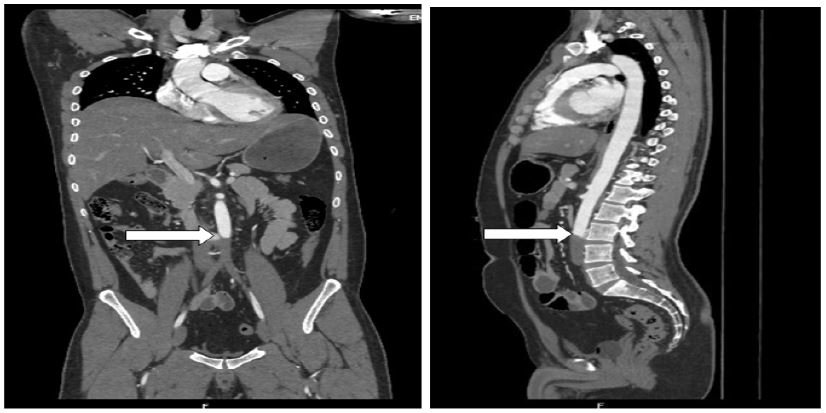
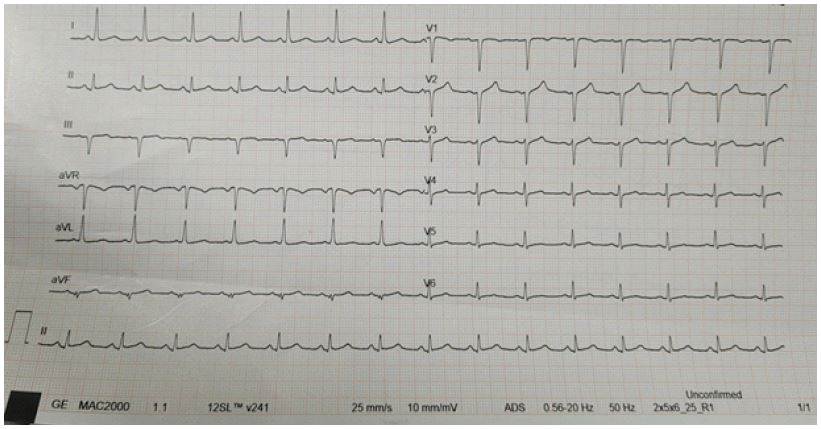
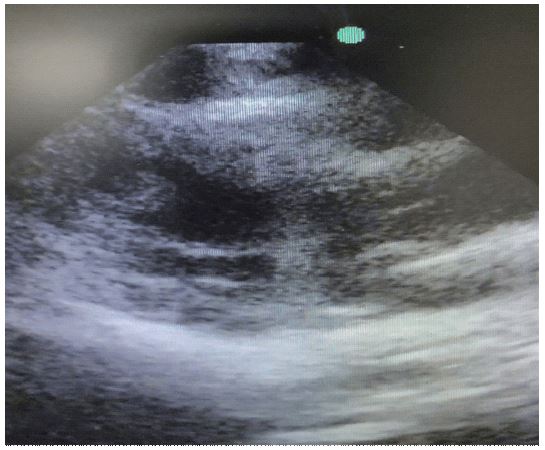
A 29-year-old male with no comorbidities presented to a peripheral hospital with complains of acute onset bilateral lower limb numbness and weakness around 5 pm. Evaluated from peripheral hospital and referred to our centre for further management. He presented to our hospital next day 4 am with features of lower limb pain and lower limb weakness. He denies the history of chest pain or any autonomic symptoms. On examination, vitals were stable, patient was drowsy, grade zero power both lower limbs, absent sensation from below inguinal area bilaterally, cold lower limbs bilaterally and bluish discoloration bilateral toes. Bilaterally lower limb pulsations not palpable till femoral artery. A CT aortogram was done which revealed occlusion of infrarenal aorta extending to both iliac arteries and additionally left renal infarction and splenic infarction was noted (Figures 1 and 2). His ECG revealed normal sinus rhythm with poor R progression (Figure 3) and echocardiogram revealed anterior regional wall motion abnormality, moderate LV dysfunction, and a large thrombus in LV cavity (Figure 4). He gives history of alcohol intake, tobacco smoking and cannabis use on the day of symptom presentation, and in the past. A diagnosis of non-ST elevation myocardial infarction with LV dysfunction followed by left ventricular clot formation associated with multiple thromboembolic phenomena was made. Vascular team discussion was emergently held and it was decided to proceed with embolectomy through a hybrid surgical and interventional approach. He was taken up for emergency surgery at 6 am on the same day. Bilateral femoral arteriotomy followed by Fogartys embolectomy-multiple runs- multiple large clots were retrieved. In view of persistent thrombus- multiple aspirations using 12 and 18 french sheaths using manual aspiration and Penumbra aspirations were performed. Huge residual thrombus burden was persistent with suboptimal flow downstream. He was continued on heparin infusion. Next day due to persistent coldness of lower limbs, he was taken up for intra-arterial thrombolysis with streptokinase via left radial access which was on flow, till the time of discharge. During the course of his stay in hospital he has been developing progressively worsening renal failure and features of rhabdomyolysis. It was managed conservatively with hydration and other supportive measures. Limbs were continuously monitored for compartment syndrome by the plastic surgery team. The need for amputation eventually was discussed with relatives. Patient was transferred to another centre at their request.
Discussion
Acute limb ischemia results from an acute (<2 weeks), abrupt decrease in arterial perfusion of the limb, and can lead to tissue loss and threaten limb viability. Acute limb ischemia is a vascular emergency and requires quick revascularization by endovascular, surgical, or a hybrid approach to avoid limb loss [1]. It may be due to a cardiac cause such as left atrial thrombus secondary to atrial fibrillation or LV thrombus following a myocardial infarction among various other potential causes [6]. Once acute limb ischemia has been identified, initial management should aim to prevent thrombus propagation with intravenous unfractionated heparin [7]. Literature suggests that cannabis use may contribute to the onset of myocardial infarction, particularly in young, otherwise healthy individuals presenting shortly after use. Proposed mechanisms include increased autonomic stimulation, altered platelet aggregation, coronary vasospasm, and exposure to toxic smoke constituents. However, the true pathogenesis is likely multifactorial [4]. In this case report, the patient had not received heparin, which may have contributed to an increased thrombus burden. He presented to our hospital 11 hours after symptom onset, during which time no anticoagulation had been administered. A careful clinical examination is essential for the early diagnosis of acute limb ischemia. Earlier identification and timely referral to a vascular centre could have potentially altered the outcome. Heart is the predominant source of emboli [6], and it is crucial to always investigate the underlying cause. In this patient, there were no initial cardiac symptoms; however, he was found to have an acute myocardial infarction with a large left ventricular thrombus prior to the development of bilateral limb ischemia. The patient was under the influence of drugs, which may have masked typical symptoms, and cannabis use itself is a known potential trigger for acute myocardial infarction.
Conclusion
This case highlights the critical importance of thorough clinical examination for the early recognition of acute limb ischemia and the prompt initiation of unfractionated heparin. It also underscores the need for early referral to a revascularization centre to optimize outcomes. Myocardial infarction and left ventricular thrombus can remain undiagnosed if not carefully evaluated. Additionally, this case reinforces the growing evidence that cannabis may act as a potential trigger for acute coronary syndrome in young individuals without traditional cardiac risk factors.
References
- Natarajan B, Patel P, Mukherjee A. Acute Lower Limb Ischemia-Aetiology, Pathology, and Management. Int J Angiola. 2020; 29(3): 168-174. doi:10.1055/s-0040-1713769.
- Bhardwaj R, Sharma SC, Rajeev R, et al. Myocardial infarction in young adults-risk factors and pattern of coronary artery involvement. Niger Med J. 2014; 55(1): 44-7. doi:10.4103/0300-1652.128161.
- Delia R, Zijlstra F, Piek JJ. Left ventricular thrombus formation after acute myocardial infarction. Heart. 2012; 98(23): 1743-9. doi:10.1136/heartjnl-2012-301962.
- Chetty K, Lavoie A, Deghani P. A literature review of cannabis and myocardial infarction-what clinicians may not be aware of. CJC Open. 2020; 3(1): 12-21. doi: 10.1016/j.cjco.2020.09.001. Erratum in: CJC Open. 2022; 4(9): 827. doi: 10.1016/j.cjco.2022.07.007.
- Mills B, Dishner E, Velasco CE. Acute myocardial infarction triggered by use of synthetic cannabis. Proc (Bayl Univ Med Cent). 2018; 31(2): 200-2. doi:10.1080/08998280.2017.1416243.
- Charmake D 3rd, Lahmidi I, Boutaybi M, Elouafi N. An acute limb ischemia concomitant with a myocardial infarction. Cureus. 2021; 13(2): 13538. doi:10.7759/cureus.13538.
- Hage AN, McDevitt JL, Chick JFB, Vadlamudi V. Acute limb ischemia therapies: when and how to treat endovascularly. Semin Intervent Radiol. 2018; 35(5): 453-60. doi:10.1055/s-0038-1676321.