
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Fibrosing alopecia in a pattern distribution after hair transplantation: A case report and literature review
Sánchez-Dueñas LE1; Gastelum-Ibarra AE2; Iribe-Martínez JP2; Aguirre-Sánchez JR3; Aviña-Padilla N2*
1Centro de Restauración Capilar DERMIKA, Guadalajara, Jalisco, México.
2Centro Dermatológico de Sinaloa Dr. Jesús Rodolfo Acedo Cárdenas, Culiacán, Sinaloa, México.
3Centro de Investigación en Alimentación y Desarrollo (CIAD), Culiacán, Sinaloa, México.
*Corresponding Author : Aviña-Padilla N
Centro Dermatológico de Sinaloa Dr. Jesús Rodolfo Acedo Cárdenas, Culiacán, Sinaloa, México.
Email: nayra_av@hotmail.com
Received : Apr 15, 2025
Accepted : May 05, 2025
Published : May 12, 2025
Archived : www.jcimcr.org
Copyright : © Aviña-Padilla N (2025).
Abstract
Patterned fibrosing alopecia is a form of scarring alopecia that shares clinical, tracheoscopy, and histopathological features with lichen panoplies and androgenetic alopecia. Its onset has been observed in patients following procedures such as hair transplants, facelifts, and other medical-surgical interventions. The Koebner phenomenon, along with alterations in the peripheral follicular immune response, is thought to trigger this condition. Literature reports a highly variable post-transplant evolution time, ranging from 3 months to 9 years. Clinically, it presents with hair loss in areas sensitive to androgens, and tracheoscopy reveals findings such as erythema, peripolar scales, reduced follicular openings, and follicular miniaturization. The therapeutic approach remains undefined, with various strategies being employed, including immunomodulators, anti-inflammatory steroids, antiandrogens, and hair growth promoters. New technologies are also currently under investigation. In this context, we present the case of a 28-year-old male diagnosed with patterned fibrosing alopecia following a Follicular Unit Extraction (FUE) hair transplant, confirmed through tracheoscopy and histopathology. The patient was treated with immunomodulatory therapy, intralesional steroids, antiandrogens, hair growth promoters, and 675 nm laser therapy, resulting in modest clinical improvement.
Keywords: Fibrosing alopecia; Scarring; Idiopathic; Hair transplant; Laser.
Citation: Sánchez-Dueñas LE, Gastelum-Ibarra AE, Iribe-Martínez JP, Aguirre-Sánchez JR, Aviña-Padilla N. Fibrosing alopecia in a pattern distribution after hair transplantation: A case report and literature review. J Clin Images Med Case Rep. 2025; 6(5): 3585.
Introduction
Patterned fibrosing alopecia was first described in 2000 by Trueb and Zinkernagel as a scarring alopecia that shares characteristics of lichen panoplies and androgenetic alopecia [1]. It is characterized by chronic inflammation that leads to perifollicular fibrosis and follicular destruction [2]. Although the pathophysiological mechanism is not yet fully understood, autoimmune factors have been implicated, including the activation of T lymphocytes and apoptosis of follicular epithelial cells [3]. In some cases, an inflammatory response may be triggered by external insults such as hair transplants and other surgical procedures, suggesting a possible link to the Koebner phenomenon [4]. Due to the rarity of this condition and the potential for misdiagnosis with other forms of scarring alopecia, it is critical to consider it in patients with alopecia after a hair transplant, particularly those with a history of suspected scalp psoriasis or seborrheic dermatitis [5]. In this context, we present a clinical case of a 28-year-old male diagnosed with patterned fibrosing alopecia following a Follicular Unit Extraction (FUE) hair transplant, providing further insight into the diagnostic process and management challenges of this condition.
Case history
A 28-year-old male from Michoacán, Mexico, with no relevant medical history, was referred to our clinic by his private dermatologist with a diagnosis of seborrheic dermatitis and acne vulgaris. He had been treated with isotretinoin for one year. During the initial consultation, a localized dermatosis on the scalp was observed, affecting the frontal and vertex regions. The lesions presented as pseudo alopecic areas accompanied by erythema and scaling (Figure 1A, 1B). Tracheoscopy examination revealed perifollicular and interfollicular scaling, erythema, brown peripolar halos, and the presence of pinpoint and glomerular vessels (Figure 2A). Based on these findings, the coexistence of seborrheic dermatitis, telogen effluvium, and androgenetic alopecia was suspected. Initial management included anti-inflammatory agents, antiandrogens, and hair growth stimulants. At follow-up, the patient reported having undergone a follicular unit extraction (FUE) hair transplant in January 2023, after which he experienced significant hair shedding. A Trichogramma demonstrated a predominance of hairs in the anagen phase (Figure 2B). Due to the clinical suspicion of scalp psoriasis, a skin biopsy was performed. Histopathological analysis revealed focal hypogranulosis of the epidermis, mild and irregular acanthosis, a perifollicular lymph histiocytic infiltrate around the upper isthmus, perifollicular fibrosis, and sebaceous gland hypoplasia (Figures 3 and 4). Laboratory evaluations to rule out thyroid dysfunction and insulin resistance were within normal limits. Considering the clinical presentation, tracheoscopy findings, and histopathology, a diagnosis of patterned fibrosing alopecia following hair transplantation was established. Treatment was initiated with hydroxychloroquine (400 mg daily for 2 months, then 200 mg daily for 4 months), dutasteride (0.5 mg daily for 6 months), oral minoxidil (5 mg daily for 6 months), topical calcipotriol/betamethasone (twice weekly), intralesional triamcinolone injections (12 mg monthly for 3 sessions), exosome therapy, and monthly sessions of 675 nm laser therapy. Despite treatment, the patient continued to experience substantial hair loss with only moderate clinical improvement. Consequently, second-line immunomodulatory therapy with methotrexate was initiated.



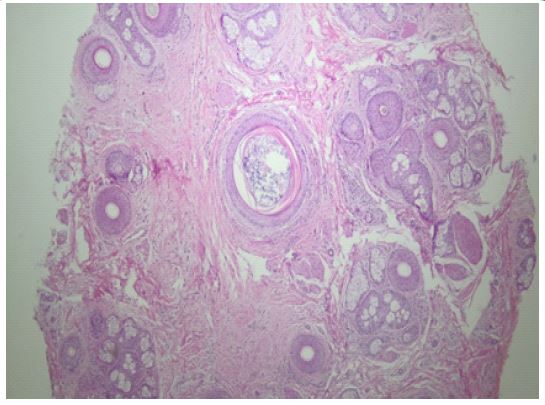
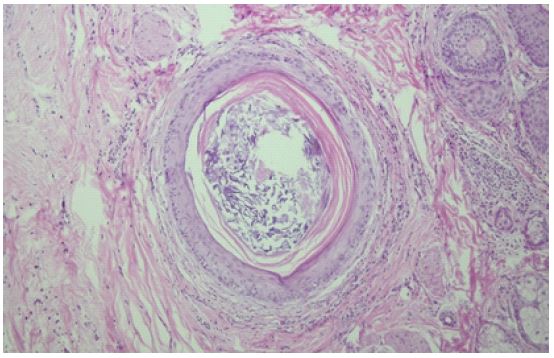
Table 1: Comparative summary of case series described in literature.
| Summary of reported casesof post-transplant patterned scarring alopecia | |||||
|---|---|---|---|---|---|
| Study | Number of patients | Age | Symptom onsetpost- transplant | Symptoms | Clinical and trichoscopic findings |
| Donovan et al20129 [8] | 17 patients(15 M, 2 F) | 30-67years | 4 a36 months | Pruritus andasymptomatic | Erythema, peripilar scaling, loss of follicular openings. LPP 70%[U3] |
| Banka et al 2014 [13] | 26 patients(17 M, 9 F) | 22-65years | History of seborrheicdermatitis | Asymptomatic ormild pruritus | >20% variability in frontal, parietal or vertex regions, erythema, 2–4 hairs emerging fromfollicular opening, peripilar and interfollicular scaling, absence of follicular openings |
| Chiang et al 2012[9] | 10 patients(4 M, 3 F) | 34-63years | 3 months to 9 years/ 2 (face lift) AFF | Pruritus | Diffuse hairloss, erythema, scaling, and loss offollicularopenings |
| Rocha Crisostomoet als 2009 [14] | 2 patients(2 M) | 50 years,46 years | 6years, 2 years | Asymptomatic | Diffuse hairloss in recipient area, erythema andperifollicular scaling |
Discussion
Fibrosing Alopecia in a Pattern Distribution (FAPD) is a form of scarring alopecia that remains underrecognized within the medical community. Its distribution pattern often mimics that of androgenetic alopecia [6]. Several reports have described its onset following hair transplantation and facial surgery, suggesting that the Koebner phenomenon and an autoimmune response targeting hair follicles-characterized by perifollicular lichenoid inflammation and progressive fibrosis—may contribute to its pathogenesis [7]. Donovan et al. (2012) documented 17 cases of lichen panoplies following hair transplantation, with a mean onset of 11 months post-procedure [8]. Similarly, Chiang et al. [9] reported the development of lichen panoplies between 3 months and 9 years after surgery (Table 1). In line with existing literature, our patient, who had a history of seborrheic dermatitis and androgenetic alopecia, developed scarring alopecia one year after undergoing FUE. The tracheoscopy findings observed-erythema, peripolar scaling, follicular miniaturization, and loss of follicular openings—were consistent with those described by Griggs et al. in cases of FAPD [10]. There is currently no standardized treatment for this condition. Therapeutic goals focus on reducing inflammation, halting follicular miniaturization, and promoting hair regrowth. The literature describes the use of immunomodulators such as hydroxychloroquine and JAK inhibitors, as noted by Tekin et al [11]. In our patient, antianantiandrogen therapy (finasteride, dutasteride) was combined with complementary approaches, including 675 nm laser therapy, to target the androgenetic component [12]. Further studies are required to clarify the pathogenesis, define clinical and tracheoscopy features, and establish comparative trials that may optimize therapeutic strategies and improve patient outcomes [9].
Conclusion
Fibrosing alopecia in a pattern distribution is a scarcely recognized form of scarring alopecia that primarily affects androgen-dependent areas. Its potential association with medical-surgical procedures such as hair transplantation and facial lifting has been proposed, suggesting the involvement of the Koebner phenomenon and a perifollicular autoimmune response. Differential diagnoses for anagen effluvium should include scalp psoriasis, lichen planopilaris, and alopecia areata. Although there is no standardized treatment protocol, therapeutic approaches have included corticosteroids, immunomodulators, antiandrogens, and laser therapy. Further research is essential to better understand its pathogenesis and to develop more effective treatment strategies.
Declarations
Competing interests: The authors declare no competing interest.
References
- Miteva MI. Alopecia. Elsevier Editora Ltda. 2019; 115- 123.
- Kossard S. Postmenopausal frontal fibrosing alopecia: Scarring alopecia in a pattern distribution. Arch Dermatol. 1994; 130(6): 770-774.
- Assoil P, Rey Gagne P. Lichen panoplies: Update on diagnosis and treatment. Semin Cutan Mes Surge. 2009; 28(1): 3-10.
- Poblet E, Jiménez F, Pascual A, et al. Frontal fibrosing alopecia after hair transplantation: Clinicopathological findings in 6 cases. J Am Accad Dermatol. 2018; 79(5): 980-982.
- Dlova NC, Goh CL, Tosti A. Frontal fibrosing alopecia and lichen panoplies in women of African ancestry: A study of 20 patients. Br J Dermatol. 2017; 177(5): 184-e185.
- Fertig RM, Garet AC, Cervantes J, Tosti A. Frontal fibrosing alopecia: A review of clinical variations and treatment options. J Am Acad Dermal. 2017; 77(4): 790-800.
- Marcos-Pinto A, De Ciprio G, Oliveira Soares R. Alopecia Fibrosante em Pardo de Distribuida Androgénica: Patojéense, Diagnóstico e Tratamiento. Rev Soc Port Dermatol Venereal. 2020; 78(3): 245-9. doi:10.29021/spdv.78.3.1222.
- Donovan JC. Lichen panoplies following hair transplantation: Report of 17 cases. Br J Dermal. 2012; 166(6): 775-83.
- Chiang YZ, Tosti A, Chaudhry IH, Lyne L, Farjo B, et al. Lichen planopilaris following hair transplantation and face‐lift surgery. British Journal of Dermatology. 2012; 166(3): 666-370.
- Griggs J, Trüeb RM, Gavazzoni Dias MFR, Hordinsky M, Tosti A. Fibrosing alopecia in a pattern distribution. J Am Acad Dermatol. 2021; 85(6): 1557-64. doi: 10.1016/j.jaad.2019.12.056.
- Tekin B, Xie F, Lehman JS. Liquen plano: ¿Qué novedades hay en el diagnóstico y el tratamiento? Am J Clin Dermatol. 2024; 25: 735-64. doi:10.1007/s40257-024-00878-9.
- Rakowska A, Olszewska M, Rudnicka L. Efficacy of 675 nm laser therapy in androgenetic alopecia: A systematic review and meta-analysis. J Eur Acad Dermatol Venereol. 2023; 37(2): 196-8.
- Banka N, Mubki T, Bunagan MJ, McElwee K, Shapiro J. Frontal fibrosing alopecia: A retrospective clinical review of 62 patients with treatment outcome and long-term follow-up. Int J Dermatol. 2014; 53(11): 1324-30.
- Crisóstomo MR, Crisóstomo MCC, Crisóstomo MGR, Gondim VJT, Crisóstomo MR, et al. Hair loss due to lichen planopilaris after hair transplantation: a report of two cases and a literature review. Anais Brasileiros de Dermatologia. 2011; 86(2): 359-362. https://doi.org/10.1590/s0365-05962011000200024.