
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
An aggressive infiltrative follicular variant of papillary thyroid carcinoma
Liara Freitas Cavalcanti1; João Pedro Kurtz Gritti2; Alessandra Lourenço Cecchini1*; Rubens Cecchini1; André Armani2
1State University of Londrina, Department of General Pathology, Laboratory of Molecular Pathology, Londrina, Paraná, Brazil.
2University Hospital of Londrina, Health Sciences Center, Department of Clinical Surgery, Londrina, Paraná, Brazil.
*Corresponding Author : Lourenço Cecchini A
State University of Londrina, Department of General Pathology, Laboratory of Molecular Pathology. Londrina, Paraná, Brazil.
Tel: +55 43999121992;
Email: alcecchini@uel.br
Received : Apr 17, 2025
Accepted : May 06, 2025
Published : May 13, 2025
Archived : www.jcimcr.org
Copyright : © Lourenço Cecchini A (2025).
Abstract
Papillary Thyroid Carcinoma (PTC) is the most common neoplasia of the thyroid gland and has several variants, being the infiltrative follicular variant rare and with variable prognosis. In this study, we reported the case of a 71-year-old male patient with hypertension and hypothyroidism, who initially presented complaints of pharyngeal discomfort after ingestion of fishbone. In two weeks, the patient develops respiratory failure and cardiac arrest, both reversed. In complementary examinations, a cervical neoplastic mass was detected with suspicion of anaplastic carcinoma. The biopsy revealed an infiltrative follicular variant of PTC, which was stadified as cT4bcN1b. Due to the extent and invasion of the neoplasm, only radiotherapy was chosen. After treatment, primary tumor reduction and lymph node stability were observed, with no evidence of disease progression.
Keywords: Cardiorespiratory arrest; Hypothyroidism; Larynx invasion; Respiratory failure.
Citation: Lourenço Cecchini A, Freitas Cavalcanti L, Pedro Kurtz Gritti J, Cecchini R, Armani A. An Aggressive Infiltrative Follicular Variant of Papillary Thyroid Carcinoma. J Clin Images Med Case Rep. 2025; 6(5): 3587.
Introduction
Thyroid cancer, the most common malignant neoplasm of the endocrine system, occupies the seventh position among the most incident cancers [1], being the fifth most common malignant neoplasm in women in Brazil [2]. In 2022, 821,000 cases and 47,507 deaths were recorded worldwide [3]. The World Health Organization (WHO) classifies thyroid neoplasms into three groups according to cell origin, biological behavior and pathological and molecular characteristics: benign lesions, low-risk neoplasms, and malignant neoplasms [4]. Among the malignant neoplasms, Papillary Thyroid Carcinoma (PTC) is the most common, corresponding to 87% of cases [5]. This neoplasm presents different subtypes, among them the follicular subtype, the second most common [6]. This follicular subtype still has two variants: encapsulated and infiltrative [7]. The infiltrative variant does not have the typical papillary architecture of PTC and often invades nerves and lymphatic vessels, being associated with a higher risk of metastasis and worse prognosis [8]. Although survival rates are above 90% [9], the prognosis is worse when present in men, in patients with advanced age or when the tumor mass is very large [10]. Treatment consists of total thyroidectomy, with lymphadenectomy in cases of metastasis or possible metastases [11]. In addition, radioiodine therapy is recommended to promote ablation of possible remaining neoplastic cells after surgery [10]. The present study aimed to present an atypical case of infiltrative follicular variant PTC, contributing with new information about the disease.
Case description
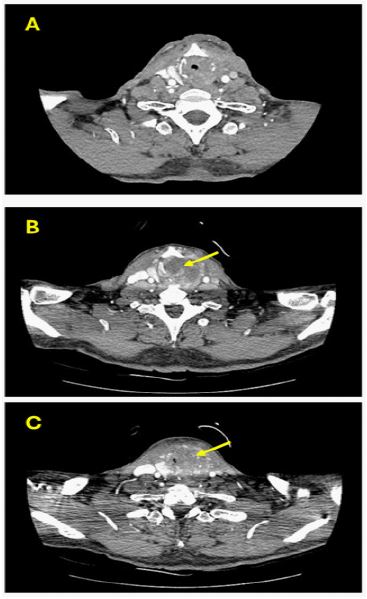
The case report was approved by the research ethics committee of the State University of Londrina (CAAE: 86096625.0.0000.5231) and the patients signed the informed consent form. Patient 71 years old, male, hypertensive, with hypothyroidism, without other comorbidities, entered the emergency room of the University Hospital (HU) of Londrina with complaints of cervical pain and odynophagia after ingestion of a fish spine. The patient was in good general condition, showing no abnormalities in the Upper Digestive Endoscopy (UDE), and was discharged without any treatment. Two weeks after initial care, he was treated in another hospital with a severe and sudden dry cough. On the previous day, reported throat stridor and dyspnea. The cough rapidly evolved into respiratory failure and required orotracheal intubation and mechanical ventilation. Soon after, it evolves to Cardiorespiratory Arrest (CRA), reversed after five cycles of measures for CPR. Subsequently, he was transferred to HU, in mechanical ventilation and need for vasoactive drugs. Clinical treatment for probable pulmonary sepsis was instituted and after one week, a tracheostomy was performed and a pulmonary thromboembolism was diagnosed. The patient evolved with bulging, hyperemia, and pain in the left lateral neck. On the tenth day of hospitalization, an exploratory cervicectomy was performed to drain the infection of the neck in the visceral space, being found, in addition to pus, a necrotic tumor of the left thyroid lobe with invasion of adjacent structures (musculature, thyroid cartilage, esophagus and trachea) suggesting anaplastic carcinoma of the thyroid. During the surgery, the cervical collection was drained, and an incisional biopsy of the left thyroid lobe was performed. The histological examination of the surgical specimen showed a PTC of infiltrative follicular variant, in addition to evidencing areas of necrosis and fibrosis. Samples of the piriformis sinus and trachea were also analyzed, and despite the discreet chronic inflammatory infiltrate observed, the malignancy in these regions was discarded. The neoplasia was staged as cT4bcN1b. Ten days after cervicectomy, magnetic resonance imaging was performed, where a tumor mass was observed in the left thyroid lobe, measuring 5.0 x 4.1 x 3.9 cm, and an estimated volume of 41.86 cm3. In addition, it showed signs of invasion to the larynx and thyroid, cricoid cartilage, and the prevertebral fascia. The involvement of the left internal jugular vein and lymph node involvement was also observed. After a few days, a neck tomography (Figure 1) and two nasofibrolaryngoscopies were performed. The tomography ruled out the presence of neoplasia in the light of the larynx and esophagus, although it showed a thickening of the mucous and submucosa layers. Also, a suspicion of lymph node spread and necrosis was evidenced, in addition to the involvement of the left internal jugular vein due to the presence of the tumor mass. The nasofibrolaryngoscopies showed supra-glottic edema, reduction of the antero-posterior diameter, salivary stasis in the valvular and left piriformis sinus, and bilateral vocal fold immobility. A month later, a laryngoscopy was performed, and a new tissue sample was obtained for histopathological analysis. The first diagnosis was then confirmed as an infiltrative follicular variant of PTC.
The yellow arrow points to the location of the tumor, measuring 5.0 x 4.1 x 3.9 cm, and estimated volume of 41.86 cm3. Expansive lesion in the left thyroid lobe, with signs of invasion of adjacent moles in the visceral space, including larynx on the left, with signs of obliteration of airspace. The images show signs of invasion of thyroid and cricoid cartilage and probable necrotic areas. A heterogeneity of the anterior adipose and cervical muscular planes was also evidenced, in addition to the liphonodomegalia in the left IIb level, and possibly a calcified lesion measuring 2.5 cm. Due to the impossibility of surgery, external beam radiotherapy in thyroid bed and neck lymph nodes was carried out six months after the first visit. The follow-up showed a decrease in primary tumor and stability of neck lymph nodes. Clinically, the patient presented improvement of symptoms, being able to occlude the tracheostomy; however, it maintained the need for the cannula. The patient can feed orally, not being necessary supplementation and does not report pain. He was in outpatient follow-up for nine months without evidence of disease progression.
Discussion
PTC is the most common thyroid neoplasm [5]. According to the WHO, this carcinoma has different subtypes [4]. In the present case, histopathological examination revealed an infiltrative follicular variant of PTC, where it is common the infiltration of neoplastic cells into the thyroid parenchyma and nearby structures such as lymphatic vessels and nerves [12]. In addition, the prognosis of the follicular subtype is worse when compared to other subtypes due to the greater chance of near and distant metastases [8]. In the present case, invasion of adjacent tissues was present, however, distant metastases were not observed. Also, lymph node metastases, destruction of the thyroid and cricoid cartilage and involvement of the left internal jugular vein were evidenced. The clinical presentation of this patient was atypical, with an initial framework of pharyngeal discomfort followed by intense cough and respiratory failure, culminating in a cardiac arrest. According to the literature, PTC usually manifests itself asymptomatically or as a palpable and painful mass in the neck, with or without involvement of the cervical lymph nodes; dysphagia and dysphonia may occur in some cases [13,14]. In this type of neoplasm, invasion to the trachea is rare and is associated with worse prognosis [15]. To date, the only reports of respiratory failure followed by mechanical ventilation in PTC have been in pediatric patients. Al-Tonbary, et al., 2009 reported the case of a pediatric patient, where the tumor invaded into the airways causing airway obstruction, respiratory failure, and metastases in the lungs [16]. In addition, Platzer et al., 2006 and Dujovne et al., 2021 presented pediatric cases similar to those mentioned above [17,18]. However, it is important to note that, in this case, the patient was an adult, and the invasion and distant metastasis were absent. Therefore, considering the rapid progression to respiratory failure and pulmonary thromboembolism, it is suggested the tumor mass was compressing the airway and adjacent vascular structures. In the present study, the patient presented thromboembolism even before surgeries. This should be pointed out since the surgical intervention is configured as a risk for pulmonary thromboembolism, as already reported in the literature [19], which was not the case. To date, the relationship between thromboembolism and PTC was not described in the literature. Ordookhani, Motazedi, Burman, 2018 evidenced a great divergence of information, being inconclusive this affirmation [20]. Therefore, the relationship between hypothyroidism (a disease that the patient had previously) and variations in hemostasis is still uncertain, transiting between states of hyper and hypocoagulability [21].
Another relevant aspect in this case was the signs of infection in the neck and the development of local hyperemia, which were initially not attributed to PTC. However, the cervicotomy revealed a necrotic tumor with adhesion in muscles, cartilage, and trachea, suggesting a potential mass effect with inflammation secondary to the invasive process. This initial manifestation highlights the more aggressive behavior of the follicular infiltrative variant that can mask the usual clinical presentation of PTC. In general, the first choice of treatment for thyroid cancer is total thyroidectomy [10]. In this case, only external beam radiotherapy was performed. Considering that the patient responded well to treatment, did not report pain, and fed well, the clinical outcome of this case was favorable considering the aggressiveness of the infiltrative follicular variant and the challenges encountered during the case.
Conclusion
This case report illustrates the complexity of the infiltrative follicular variant of PTC. The initial atypical presentation, with intense respiratory symptoms and signs of cervical invasion, demonstrated the infiltrative nature of this subtype, which differs significantly from the behavior of the most common PTC. Therefore, the events reported here will contribute to the literature for a greater understanding of this subtype.
References
- Bogović Crnčić T, Ilić Tomaš M, Girotto N, Grbac Ivanković S. Risk factors for thyroid cancer: What do we know so far? Acta Clin Croat. 2020; 59(1): 66-72.
- Instituto Nacional De Câncer (INCA). Cânceres de cabeça e pescoço. Rio de Janeiro: INCA. 2023 [cited 2024 Dec 13]. Available from: https://www.inca.gov.br/tipos-de-cancer/cabeca-e-pescoco.
- Global Cancer Observatory. Thyroid cancer mortality. Lyon: International Agency for Research on Cancer; 2020. https://gco.iarc.fr/.
- World Health Organization. Cancer. Geneva: WHO. 2024. https://www.who.int/news-room/fact-sheets/detail/cancer.
- Chen W, Wei T, Li Z, Jiang D, Liu Y, et al. Association of the preoperative inflammation-based scores with TNM stage and recurrence in patients with papillary thyroid carcinoma: A retrospective, multicenter analysis. Cancer Manag Res. 2020; 12: 1809-18.
- Jung CK, Bychkov A, Kakudo K. Update from the 2022 World Health Organization Classification of Thyroid Tumors: A Standardized Diagnostic Approach. Endocrinol Metab (Seoul). 2022; 37(5): 703-718.
- Sohn SY, Lee JJ, Lee JH. Molecular profile and clinicopathologic features of follicular variant papillary thyroid carcinoma. Pathol Oncol Res. 2020; 26(2): 927-936.
- Baloch Z, Mete O, Asa SL. Immunohistochemical biomarkers in thyroid pathology. Endocr Pathol. 2018; 29(2): 91-112.
- Stergiou A, Pantelis E, Kormas T, Agrarianism G. Case report: skeletal muscle metastasis from follicular thyroid carcinoma presenting as synovial sarcoma. Front Oncol. 2023; 13: 994729.
- Abdullah MI, Junit SM, Ng KL, Jayapalan JJ, Karikalan B, et al. Papillary thyroid cancer: genetic alterations and molecular biomarker investigations. Int J Med Sci. 2019; 16(3): 450-460.
- American Cancer Society. Thyroid cancer. Atlanta: American Cancer Society. 2022. https://www.cancer.org/cancer/types/thyroid-cancer.
- J Juhlin CC, Mete O, Baloch ZW. The 2022 WHO classification of thyroid tumors: novel concepts in nomenclature and grading. Endocr Relat Cancer. 2022; 30(2): 220293.
- Hunsaker JC, Hoffman G. Papillary thyroid carcinoma: an autobiographical case report. Cureus. 2022; 14(2): 22559.
- Choi H, Kasabian K, Melick A, Ong K, Jones SJM, et al. Papillary thyroid carcinoma: prognostic significance of cancer presentation. Am J Surg. 2015; 210(2): 298-301.
- Ahmed M, Saleem M, Al-Arifi A, Al Mahfouz A, Mahasin Z, Al-Sobhi S, et al. Obstructive endotracheal lesions of thyroid cancer. J Laryngol Otol. 2002; 116(8): 613-621.
- Al-Tenbury Y, Salata K, El-Ashry R, Fouda A. Papillary thyroid carcinoma presenting with upper respiratory tract obstruction and pulmonary metastases. World J Pediatr. 2009; 5(3): 229-231.
- Platzer ML, Vega-Briceño LE, González DH, Iñiguez OF, Escobar FC, et al. Cáncer tiroideo: una causa infrecuente de obstrucción de vía aérea superior en niños. Caso clínico. Rev Med Chil. 2006; 134(6): 772-776.
- Dujovne N, Lucero MB, Gazek N, Pitoia F, Felipe L, Ayarzabal V, et al. Respuesta al lenvatinib en una paciente pediátrica con insuficiencia respiratoria asociada a carcinoma papilar de tiroides. Arch Argent Pediatr. 2021; 119(1): e70–e74.
- Reinke CE, Hadler RA, Karakousis GC, Fraker DL, Kelz RR. Does the presence of thyroid cancer increase the risk of venous thromboembolism in patients undergoing thyroidectomy? Surgery. 2011; 150(6): 1275–1285.
- Ordookhani A, Motazedi A, Burman KD. Thrombosis in thyroid cancer. Int J Endocrinol Metab. 2017; 16(1): e57897.
- Wei WT, Liu PP, Lin SM, Peng CCH, Wang JH, Huang HK, et al. Hypothyroidism and the risk of venous thromboembolism: a nationwide cohort study. Thromb Haemost. 2020; 120(3): 505–514.