
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Eruptive xanthomas revealing severe hypertriglyceridemia: A dermatologic window into metabolic crisis
Gastélum-Ibarra AE1*; Aviña-Padilla N1; Aguirre-Sánchez JR2
1Sinaloa Dermatological Center, Dr. Jesús Rodolfo Acedo Cárdenas, Culiacán, Sinaloa, Mexico.
2Center for Research in Food and Development (CIAD), Culiacán, Sinaloa, Mexico.
*Corresponding Author : Gastelum-Ibarra AE
Sinaloa Dermatological Center, Dr. Jesús Rodolfo Acedo Cárdenas, Culiacán, Sinaloa, Mexico.
Email: ana.derma@outlook.com
Received : Apr 21, 2025
Accepted : May 07, 2025
Published : May 14, 2025
Archived : www.jcimcr.org
Copyright : © Gastelum-Ibarra AE (2025).
Abstract
Eruptive xanthomas are rare cutaneous manifestations characterized by lipid deposition in the skin. They are often underrecognized but may represent the first clinical sign of an underlying lipid metabolism disorder, such as severe hypertriglyceridemia. Clinically, they appear as yellowish papules or nodules, frequently surrounded by an erythematous halo, and are predominantly located in areas of friction, extensor surfaces, the back, and the gluteal region. Histopathological examination reveals numerous foamy histiocytes within the dermis. Management is centered on metabolic control through a multidisciplinary approach. We report the case of a 40-year-old male who presented to the dermatology clinic with yellowish papuloid lesions. Laboratory findings revealed marked hypertriglyceridemia (7450 mg/dL), and the diagnosis of eruptive xanthomas was confirmed via histopathological analysis. The patient was treated with subcutaneous insulin and lifestyle modifications, leading to clinical improvement.
Keywords: Dermatological manifestations; Lipid-laden foamy Histiocytes; Hyperlipidemia; Disorder of lipid metabolism.
Citation: Gastélum-Ibarra AE, Aviña-Padilla N, Aguirre-Sánchez JR. Eruptive xanthomas revealing severe hypertriglyceridemia: A dermatologic window into metabolic crisis. J Clin Images Med Case Rep. 2025; 6(5): 3590.
Introduction
Eruptive xanthomas are uncommon dermatological manifestations caused by dermal deposition of lipids, primarily triglycerides, in the context of severe dyslipidemia [1]. The pathophysiology of this condition involves a marked elevation of chylomicrons and plasma lipoproteins, influenced by genetic factors that are classified into various subtypes (Table 1) [2-4]. Lipoproteins, responsible for lipid transport throughout the body, are classified into five types based on their density and follow two main metabolic pathways. The exogenous pathway begins in the intestine with the formation of chylomicrons, which are processed by the enzyme Lipoprotein Lipase (LPL) to release free fatty acids. The remnants are subsequently taken up by the liver. In the endogenous pathway, the liver synthesizes Very-Low-Density Lipoproteins (VLDL), which are hydrolyzed by LPL to produce Intermediate-Density Lipoproteins (IDL), and eventually Low-Density Lipoproteins (LDL). These particles may be cleared or deposited in various tissues, including the dermis, where they are phagocytosed by cutaneous macrophages that transform into foamy cells [5]. The localized accumulation of these cells in the superficial dermis gives rise to sudden-onset, yellowish papular lesions, typically surrounded by an erythematous halo and associated with local inflammation [6]. This condition may coexist with poorly controlled diabetes mellitus, metabolic syndrome, and familial dyslipidemias [7]. Due to its rarity, eruptive xanthomatosis is often underrecognized in clinical practice, potentially delaying the diagnosis of primary or secondary dyslipidemias [8]. Under this background, the presentation of clinical cases is essential to promote early recognition and comprehensive management through a multidisciplinary approach involving internal medicine, endocrinology, nutrition, and dermatology [9].
Case history
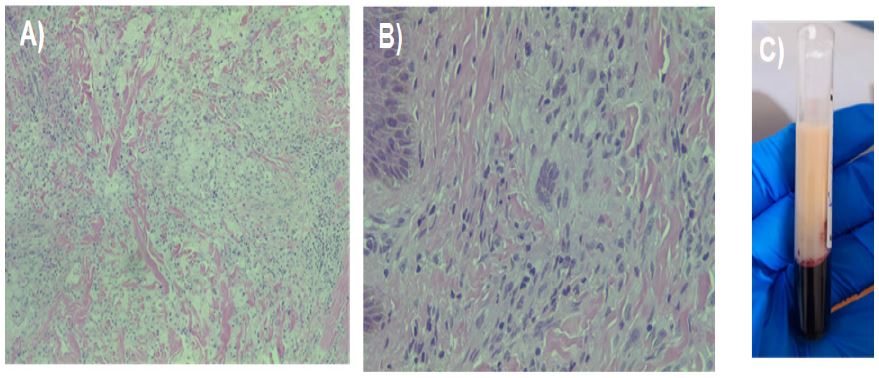
A 40-year-old male patient, with no known personal pathological history, presented with disseminated cutaneous lesions. Physical examination revealed a widespread dermatosis involving the trunk, shoulders, and extremities, with a bilateral distribution and predominance on extensor surfaces. The lesions consisted of multiple exophytic yellowish papular and nodular formations, set on an erythematous base, with regular borders, ranging in size from 0.2 to 1 cm in diameter. The Koebner phenomenon was observed. The lesions were asymptomatic (Figure 1). Based on the clinical presentation, differential diagnoses included eruptive histiocytosis, sarcoidosis, disseminated granuloma annulare, and eruptive xanthomas. Laboratory investigations were ordered, revealing: complete blood count within normal limits, serum glucose of 165 mg/dL, creatinine 0.95 mg/dL, uric acid 11.5 mg/dL, triglycerides 7450 mg/dL, and total cholesterol 658 mg/dL. An excisional biopsy of one nodular lesion was performed. Histopathological examination showed vacuolated histiocytes with a foamy appearance and multinucleated Touton giant cells in the superficial and mid-dermis (Figure 2). Based on clinical, biochemical, and histopathological findings, a diagnosis of eruptive xanthomas secondary to severe hypertriglyceridemia and hypercholesterolemia was confirmed. The patient was referred to the internal medicine department, where treatment was initiated with intravenous insulin infusion and a strict sugar-free diet. Subsequently, pharmacological therapy was instituted with bezafibrate (200 mg every 12 hours), subcutaneous insulin glargine (10 IU daily), and atorvastatin (80 mg daily), resulting in excellent therapeutic response. At the one-month follow-up, laboratory results showed: glucose 110 mg/dL, creatinine 0.96 mg/dL, uric acid 8.8 mg/dL, total cholesterol 366 mg/dL, and triglycerides 1870 mg/dL. After one year of treatment, triglyceride levels had decreased to 108 mg/dL (Table 2), with complete resolution of the cutaneous lesions.
Table 1: Classification of hyperlipidemias and association with Xanthomonas.
| Type | Name | Elevated lipoproteins | Main mechanism | Involved genes/causes | Association with xanthomas |
|---|---|---|---|---|---|
| Type I[16] | Hyperchylomicronemia | Chylomicrons | LPL deficiency or cofactors preventing triglyceride hydrolysis | LPL, APOC2, APOA5, LMF1,GPIHBP1 | Frequent eruptivexanthomas |
| Type IIa[17] | Familialhypercholesterolemia | LDL | Decreased LDL clearance due to receptor defects | LDLR, APOB,PCSK9 | Tendinous andtuberous xanthomas |
| Type IIb[18] | Familial combinedhyperlipidemia | LDL andVLDL | Overproduction ofapoB100 and VLDL | Multifactorial (genetic +lifestyle) | Occasional eruptivexanthomas |
| Type III[19] | Dysbetalipoproteinemia | Remnants of VLDL and chylomicrons | Defective ApoE binding toLDL receptor | APOE (homozygosity E2/E2) | Tuberous, palmar, anderuptive xanthomas |
| Type IV[20] | Endogenous hypertriglyceridemia | VLDL | Hepatic overproductionof VLDL | Obesity,diabetes, insulin resistance | Eruptive xanthomas insevere cases |
| Type V[21] | Mixed hyperlipidemia | Chylomicrons andVLDL | Combined alterations inexogenous and endogenous pathways | Genetic + secondary factors(alcohol, diet, diabetes) | Frequent eruptive xanthomas and pancreatitis |
LDL: Low-Density Lipoproteins; VLDL: Very-Low-Density Lipoproteins; LPL: Lipoprotein Lipase; Ape: Apolipoprotein E.

Table 2: Monitoring of triglyceride and cholesterol levels at different time intervals.
| Clinical moment | Triglycerides (mg/dL) | Total, colesterol (mg/dL) |
|---|---|---|
| Beginning | 7450 | 658 |
| One month | 1870 | 366 |
| A year | 108 | 147 |
Discussion
In the case presented, a 40-year-old male patient exhibited characteristic cutaneous lesions and markedly elevated triglyceride levels of 7,450 mg/dL, placing him within the range associated with a high risk for pancreatitis and cardiovascular events. Numerous reports have highlighted the association between eruptive xanthomas and severe hypertriglyceridemia [10-13]. Tang et al. described a case involving a male patient with triglyceride levels of 6,697 mg/dL and total cholesterol of 943 mg/dL, where the lesions were distributed over extensor surfaces and showed resolution following intensive metabolic control [10]. Similarly, Muñoz et al. reported a patient with initial triglyceride levels of 6,284 mg/dL and extensive cutaneous manifestations, whose lesions resolved after treatment with insulin and fibrates [11]. Both cases are comparable to the present report in terms of laboratory findings and clinical presentation. Pierce et al. and Nayak et al. also documented cases involving young patients with yellowish-erythematous lesions affecting the trunk and extremities, associated with triglyceride levels exceeding 3,000 mg/dL. In both cases, favorable outcomes were achieved through lipid-lowering interventions [12]. Saoji et al., from India, reported a patient with lesions on the palms and elbows, and extremely elevated triglyceride levels (7,754 mg/dL), attributed to type V hyperlipidemia. Clinical remission was achieved with a combination of statins, omega-3 fatty acids, and cevoglitazar [13]. Although the histopathological characteristics of eruptive xanthomas (i.e., foamy histiocytes in the reticular dermis) and their anatomical distribution tend to be consistent, the precipitating factors may vary. Some authors have identified poorly controlled diabetes as the primary trigger [14], while others have reported associations with alcohol consumption [15], genetic predisposition, and the use of specific medications [16]. In the present case, an interdisciplinary approach resulted in a progressive reduction of lipid levels-from 7,450 mg/dL to 108 mg/dL within one year (Table 2) accompanied by complete resolution of the cutaneous lesions. This clinical course supports existing literature indicating that appropriate management of dyslipidemia, combined with nutritional and pharmacologic interventions, is crucial for the remission of eruptive xanthomas [8,13]. Despite being a rare condition, eruptive xanthomas should be recognized as important clinical indicators of potentially serious metabolic disorders.
Conclusion
Eruptive xanthomas, while infrequent, represent a critical dermatological sign that may be the first indication of severe underlying metabolic disorders. The dermatologist plays a pivotal role in recognizing these lesions and initiating a timely and comprehensive diagnostic approach. As demonstrated in this case, cutaneous manifestations can precede or coincide with life-threatening conditions such as acute pancreatitis, premature cardiovascular disease, and, in extreme cases, sudden death. Early identification and multidisciplinary management are essential to reduce morbidity and improve long-term outcomes. Therefore, awareness and prompt referral by dermatologists can significantly influence patient prognosis
Declarations
Competing interests: The authors declare no competing interest.
Acknowledgment: We would like to express our sincere gratitude to Dr. Juan Pedro Iribe, Director of the Dermatological Center of Sinaloa, for his mentorship, and to Dr. César García Niebla, our Head of Medical Education, for his support during the management of this clinical case.
References
- Nayak KR, Daly RG. Eruptive xanthomas associated with hypertriglyceridemia and new-onset diabetes mellitus. N Engl J Med. 2004; 350(12): 1235. doi:10.1056/NEJMicm031195.
- Koala C, Marais AD, Visserses FLJ. Familial dysbetalipoproteinemia: an underdiagnosed lipid disorder. Curr Opin Endocrinol Diabetes Obes. 2017; 24(2): 133-9. doi:10.1097/MED.0000000000000316.
- Abifadel M, Boileau C. Genetic and molecular architecture of familial hypercholesterolemia. J Intern Med. 2022; 292(4): 457-67. doi:10.1111/joim.13577.
- Quiroga-Padilla PJ, Gaete PV, Mendivil CO. Quilomicronemia familiar [Familial chylomicronemia]. Medicina (B Aires). 2020; 80(4): 348-58. PMID: 32841138.
- Renner R, Teuwen I, Harth W, Treudler R, Simon JC. Eruptive Xanthome bei Hypertriglyzeridämie. Hautarzt. 2008; 59(12): 995-9. doi:10.1007/s00105-008-1534-y.
- López Cepeda L, Ramos-Garibay JA, Petrocelli Calderón D, Manríquez Reyes A. Xantomas eruptivos como manifestación inicial de diabetes mellitus e hipertrigliceridemia severa. 2010.
- Stark M, Stuart J. Eruptive xanthoma in the setting of hypertriglyceridemia and pancreatitis. Am J Emerg Med. 2018; 36(10): 1925. 5-7. doi: 10.1016/j.ajem.2018.04.056.
- Rojas GA, Hernández DK, Espinoza W. Xantomatosis eruptiva: presentación de un caso y revisión de la literatura. Rev Colomb Endocrinol Diabetes Metab. 2018; 5(1): 44-6.
- Gaxiola-Álvarez EA, Manríquez-López CA. Eruptive xanthomas as initial manifestation of dyslipidemia: case report. 2019.
- Arenas R. Dermatología: Atlas, diagnóstico y tratamiento. 7.ª ed. México: McGraw-Hill; 2020.
- Pierce J, Patel T, Scott C. Eruptive xanthomas. Mayo Clin Proc. 2021; 96(12): 3097-8. doi: 10.1016/j.mayocp.2021.09.019
- Tang KY, Wu MY, Li J. Eruptive xanthomas. JAMA Dermatol. 2023;159(4):449. doi:10.1001/jamadermatol.2022.5834.
- Munoz NR, Agwuegbo CC, Gauhar F. Eruptive xanthomas precipitated by severe hypertriglyceridemia from diabetes and alcohol use. Cureus. 2023; 15(8): 43288. doi:10.7759/cureus.43288.
- Mathew S, Lobo C, Kaimal S, Raj S. Eruptive xanthomas. N Z Med J. 2024; 137(1601).
- Saoji V, Madke B, Shembalkar J, Rambhia K. Eruptive xanthomas. BMJ Case Rep. 2024; 17: 260230. doi:10.1136/bcr-2024-260230.
- Yamashita S. [Primary hyperchylomicronemia]. Nihon Rinsho. 2013; 71(9): 1578-83.
- Hershberger RE, Cuchel M, Bourbon M, Sijbrands EJ, Nordestgaard BG, et al. Clinical genetic testing for familial hypercholesterolemia: JACC Scientific Expert Panel. J Am Coll Cardiol. 2018; 72(6): 662-680. doi: 10.1016/j.jacc.2018.05.044.
- Padda IS, Fabian D, Johal GS. Familial Combined Hyperlipidemia. [Updated 2023 Jun 3]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025. https://www.ncbi.nlm.nih.gov/books/NBK592399.
- Koopal C, Marais AD, Visseren FL. Familial dysbetalipoproteinemia: an underdiagnosed lipid disorder. Curr Opin Endocrinol Diabetes Obes. 2017; 24(2): 133-139. doi: 10.1097/MED.0000000000000316.
- Malick WA, Do R, Rosenson RS. Severe hypertriglyceridemia: Existing and emerging therapies. Pharmacol Ther. 2023; 251: 108544. doi: 10.1016/j.pharmthera.2023.108544.
- Dron JS, Hegele RA. Genetics of Hypertriglyceridemia. Front Endocrinol (Lausanne). 2020; 11: 455. doi: 10.3389/fendo.2020.00455.