
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Antenatal diagnosis of cranio-thoraco-ophiophagus in ultrasound: A very rare case report of conjoined twins
*Corresponding Author : Lovely Jain
Department of Community Medicine and School of Public Health, Post Graduate Institute of Medical Education & Research (PGIMER), Chandigarh, India.
Email: lavijain001@gmail.com
Received : Apr 21, 2025
Accepted : May 08, 2025
Published : May 15, 2025
Archived : www.jcimcr.org
Copyright : © Jain L (2025).
Abstract
The occurrence of conjoined twins is a rare event, with cranio-thoraco-omphalopagus being the rarest form. In this article, we report the case of a 30-year-old primigravida at 18 weeks gestation who was referred to our centre for a second opinion following an abnormal antenatal report from another clinic. We performed a Mi trimester Anomalies Scan, which confirmed the presence of cranio-thoraco-Ophiophagus conjoined twins.
Keywords: Antenatal diagnosis; Conjoined twins; Ultrasound; Cranio-thoraco-ophiophagus.
Citation: Jain L. Antenatal diagnosis of cranio-thoraco-ophiophagus in ultrasound: A very rare case report of conjoined twins. J Clin Images Med Case Rep. 2025; 6(5): 3592.
Background
Conjoined Twins (CT), one of the rarest congenital anomalies, has long fascinated clinicians. Conjoined Twins (CT), commonly referred to as Siamese twins, are defined as monochorionic monoamniotic twins that are anatomically fused at one or more sites in utero due to abnormal zygote division during embryological development. The reported incidence of conjoined twins is 1 in 50,000; however, due to the high rate of stillbirth, the true incidence is estimated to be approximately 1 in 200,000 live births [1]. Females are three times more likely to be affected than males [2]. Various types of conjoined twins have been classified based on the primary site of union, with thoracophagus being the most common and omophagous the least common. Union at multiple sites, as in our case of cranio-thoraco-Ophiophagus [3], is the rarest of rare occurrences. Imaging, primarily ultrasound, is of utmost importance in both prenatal diagnosis and planning of further management of conjoined twins, followed by CT and MRI if needed [1].
Case report
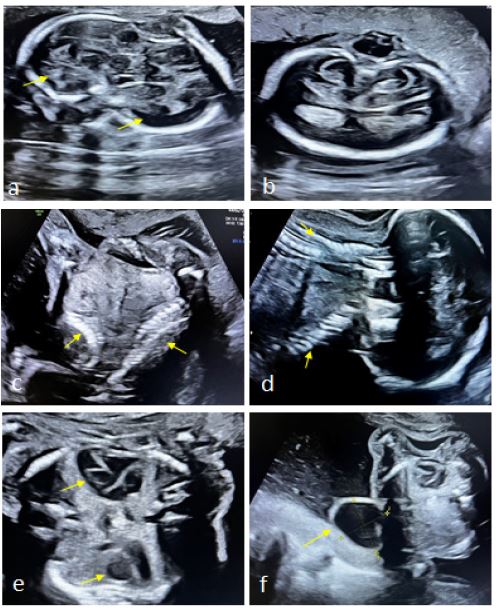
A 30-year-old primigravida female, at 18 weeks gestation, was referred to our center for a second opinion following an abnormal antenatal scan from another clinic, which noted a large head size and meningocele. The patient had no family history of twins or consanguinity. There was no history of any exposure to teratogenic agents, infections, fever, radiation, or other medical conditions during pre-conceptional and early antenatal periods. She did not have any antenatal checkups previously or take folic acid supplementation during that period. The Mi trimester Anomalies Scan performed at our center at 18 weeks 5 days revealed a plethora of findings, leading to the very rare diagnosis of monochorionic monoamniotic conjoint twin (cranio-thoraco-omphalopagus). The examination revealed two faces fused laterally, each with one pair of eyes, one nose, one mouth, and two ears (Figure 1). The two brains were fused along temporal region, with obliteration of the posterior fossa in one fetus. Further findings included partial fusion of the thoracic and abdominal regions, with two normal-looking hearts, two livers, four kidneys, and two urinary bladders. The spines were separate, though both the fetuses exhibited kyphoscoliosis with evidence of lumbosacral spina bifida and meningomyelocele in one of the fetuses (which also had obliteration of the posterior fossa) (Figure 2). All the four upper limbs and lower limbs were separately visualized. Placenta was single, anterior, and located in upper uterine segment. Amniotic fluid was adequate. Cervical length was 4.2 cm at the time of scan with closed internal os (internal orifice of the cervix). The patient was counseled about Medical Termination of Pregnancy (MTP) due to the grave outcomes associated with such malformations. The sex of the fetuses was neither detected nor disclosed to anyone in any manner. The abortus was closely examined, confirming the gross findings, as shown in Figure 3. No autopsy or post-mortem imaging was performed.


Discussion
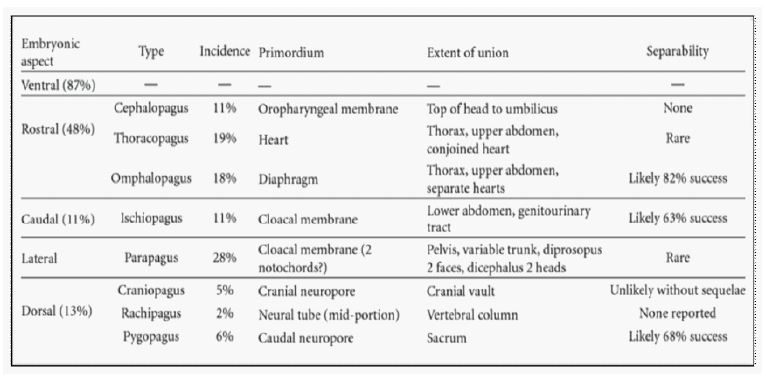
Conjoined twins are often considered an ‘extraordinary accident of nature.’ The exact cause of conjoined twinning remains unknown. In the 18th century, it was thought that conjoined twins resulted from one ovum being fertilized by two sperms, a concept known as the collision theory. Today, two primary theories have been proposed to explain the formation of conjoined twins: The fission theory and the fusion theory, with the latter gaining more acceptance [4]. According to the fission theory, the embryonic disc undergoes incomplete separation around 13-15 days post-fertilization, typically indicating the day of splitting. In contrast, the fusion theory suggests that two separate mono-ovular embryonic discs undergo secondary association [1]. Different classification systems exist for conjoined twins. Spencer et al. (1996) classified them into eight main types based on the degree and site of fusion (Figure 4). In most cases, fusion occurs at a single site, while in rare instances, two sites can be fused, such as in acephalothoracias or thoracoomphalopagus [4]. Our case is exceptionally unique as it involves fusion at multiple sites including head, face, thorax, and abdomen which is a very rare occurrence in literature so far to the best of our knowledge. The outcome and survival rate of conjoined twins is primarily influenced by the site of fusion and the specific organs affected. In a study involving 14 prenatally diagnosed cases of conjoined twins, 28% resulted in intrauterine death, 54% died shortly after birth, and only 18% survived [1]. Ultrasound is the safest and most reliable method for diagnosing such conditions in utero. Prenatal diagnosis of conjoined twins, which has become more common since the late 1970s (after advent of antenatal ultrasound), can be made as early as the first trimester. Indicators include fetuses in the same position, inseparable body contours, facing each other with hyper flexed cervical spines, fewer limbs, shared organs, and a single umbilical cord with more than three vessels, depending on site of fusion [4]. Due to high post-natal morbidity and mortality of conjoined twins, early prenatal diagnosis is crucial for planning appropriate action. Antenatal ultrasound can diagnose conjoined twin pregnancies as early as 12 weeks gestation [5]. This diagnosis largely depends on the radiologist’s skills and awareness of this condition. Conjoined twins can be easily missed if not carefully examined as they may resemble normal twins in certain fetal positions. Poor ultrasound quality, maternal obesity and less amniotic fluid can also hinder accurate detection. To date, only a few case reports are available where conjoined twins were diagnosed prenatally at 24, 28, and 29 weeks of gestation. This case was diagnosed even earlier i.e., at 18 weeks of gestation following an abnormal antenatal ultrasound report from another clinic, which noted a large head size and meningocele [6-9]. This is similar to a case reported by Alansari B et al., [6] which was also diagnosed upon seeking a second opinion. Most conjoined twins are diagnosed before birth and are usually delivered by cesarean section. Surgical separation of conjoined twins can only be successful if vital organs are not shared [6]. In addition to 2D imaging, Color Doppler and 3D ultrasound can confirm the diagnosis and assess the extent of organ sharing, which is crucial for assisting parents in making informed decisions. Color Doppler ultrasound is crucial for visualizing blood flow, helping to identify shared vascular structures between the twins, which is essential for evaluating the risks associated with separation [4]. Additionally, 3D ultrasound enhances the assessment by providing a three-dimensional view of the anatomy, allowing for a detailed examination of the twins’ organs and their connections, thereby further aiding parents in making appropriate decisions. Pregnancies between 18-24 weeks can be legally terminated medically [4]. In our case, after counseling of the patient on the risks and benefits, she was taken for an elective hysterotomy at 18 weeks. The procedure was completed without complications and fetuses were scrutinized and ultrasound findings were confirmed.
Conclusion
Conjoined twins are a rare and complex phenomenon with origins largely attributed to the fusion theory. Early prenatal diagnosis is critical due to their high morbidity and mortality rates. Surgical options for separation depend on the extent of organ sharing, as determined by advanced imaging techniques such as Color Doppler, 3D ultrasound, and 2D scan. Our case at 18 weeks highlights the importance of accurate antenatal diagnosis, appropriate patient counselling and timely careful management for preventing morbid outcomes of such pregnancies.
References
- Mathew RP, Francis S, Basti RS, et al. Conjoined twins-role of imaging and recent advances. J Ultrason. 2017; 17(71): 259-66.
- Saxena R, Sinha A, Pathak M, et al. Conjoined Thoracopagus Twins: A Systematic Review of the Anomalies and Outcome of Surgical Separation. African J Paediatr Surg. 2023; 20(3): 157-65.
- Spencer R. Anatomic description of conjoined twins: A plea for standardized terminology. J Pediatr Surg. 1996; 31(7): 941-4.
- Kokcu A, Cetinkaya MB, Aydin O, et al. Conjoined twins: Historical perspective and report of a case. J Matern Neonatal Med. 2007; 20(4): 349-56.
- Pajkrt E, Jauniaux E. First‐trimester diagnosis of conjoined twins. Prenat Diagn. 2005; 25(9): 820-6.
- Alansari B, Wassan BAO, B MB, et al. Conjoined Twins- Cephalo-Thoraco-Omphalopagus : A Case Report. 2021; 43(2): 531-3.
- Abdullah H, Abdul Wahab N, Abu Bakar K. Fetal MRI of thoraco-omphalopagus conjoined twins. BMJ Case Rep. 2017; 2017-219793.
- Sabih D, Ahmad E, Sabih A, et al. Ultrasound diagnosis of cephalopagus conjoined twin pregnancy at 29 weeks. Biomed Imaging Interv J. 2010; 6(4).
- Vegar-Zubović S, Prevljak S, Behmen A, Bektešević H, Zubović D, et al. Conjoined twins-A case report of prenatal diagnosis of cephalothoracoomphalopagus. Radiography. 2020; 26(2): 126-8.