
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 6
MRI diagnosis of lipomyelocele in a child with Tethered Cord syndrome
Tlaite Oubaddi*; Zineb Izi; Siham El Haddad; Nazik Allali; Latifa Chat
Pediatric Radiology Department, Ibn Sina University Hospital Center, Faculty of Medicine and Pharmacy of Rabat, Mohammed V University, Rabat, Morocco.
*Corresponding Author : Tlaite Oubaddi
Pediatric Radiology Department, Ibn Sina University Hospital Center, Faculty of Medicine and Pharmacy of Rabat, Mohammed V University, Rabat, Morocco.
Email: tlaite.oubaddi@gmail.com
Received : Apr 22, 2025
Accepted : May 12, 2025
Published : May 19, 2025
Archived : www.jcimcr.org
Copyright : © Oubaddi T (2025).
Citation: Obada T, Izi Z, El Haddad S, Allali N, Chat L. MRI diagnosis of lipomyelocele in a child with Tethered Cord syndrome. J Clin Images Med Case Rep. 2025; 6(5): 3595.
Introduction
A 5-year-old boy, presenting with fecal incontinence, had a subcutaneous swelling in the sacral region since birth. Lumbo-sacral MRI revealed a posterior neural arch defect through which a lipomatous subcutaneous mass penetrated the spinal canal and attached to the tethered cord (Figure 1). The spinal cord-lipoma junction was located within the spinal canal, consistent with a diagnosis of lipomyelocele. Lipomyelocele is a subtype of closed spinal dysraphism characterized by a subcutaneous lipomatous mass that herniates through a defect in the posterior neural arch, penetrating the spinal canal and attaching to the tethered spinal cord. Unlike lip myelomeningocele, there is no meningeal herniation, and the subarachnoid space remains intact. The lipoma is typically located within or at the margin of the spinal canal, without expansion of the surrounding cerebrospinal fluid spaces. Clinically, patients may present with a sacral mass and neurological symptoms, such as urinary and fecal incontinence, depending on the level of the tethered cord. MRI plays a crucial role in diagnosing lipomyelocele by providing detailed imaging of the spinal cord, lipoma, and associated anatomical anomalies [1,2].
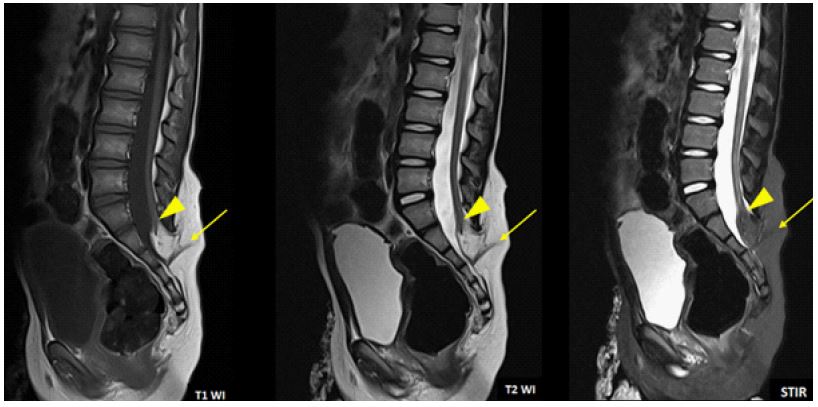
Note that the spinal cord–lipoma junction is located within the spinal canal.
References
- Rossi Andrea et al. Imaging in spine and spinal cord malformations. European Journal of Radiologie. 2004; (50(2): 177-200.
- Rudenter Stéphanie L et al. Congenital spine and spinal cord malformations-pictorial review. American Journal of Roentgenology. 194.3_supplement. 2010; 26-37.