
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Atypical imaging findings of “uterine smooth muscle tumor of uncertain malignant potential (stump)”: A case report
Rodríguez de Trujillo Campo-Cossio Marta1*; Mesa Quesada Juan1; Gómez Serrano Jose Angel2; Caro Cuenca María Teresa2; López Ruiz Daniel José1
1Section of Diagnostic and Therapeutic Neuroradiology, UGC of Radiodiagnosis, Reina Sofía University Hospital, Córdoba, Spain.
2Pathological Anatomy Service, Reina Sofía University Hospital, Córdoba, Spain.
*Corresponding Author : Rodríguez de Trujillo Campo-Cossio Marta
Section of Diagnostic and Therapeutic Neuroradiology, UGC of Radiodiagnosis, Reina Sofía University Hospital, Córdoba, Spain.
Email: martarodriguezdetrujillo@gmail.com
Received : Apr 22, 2025
Accepted : May 13, 2025
Published : May 20, 2025
Archived : www.jcimcr.org
Copyright : © Campo-Cossio Marta RdT (2025).
Abstract
Background: Uterine Smooth Muscle Tumors of Uncertain Malignant Potential (STUMPs) are rare neoplasms with characteristics that lie between benign and malignant tumors. They often present as uterine masses causing symptoms such as abnormal bleeding, pelvic pain, or mass effect. Differentiating STUMPs from leiomyomas or leiomyosarcomas can be challenging due to overlapping features. Imaging, particularly Magnetic Resonance Imaging (MRI), can identify features distinct from those of leiomyomas, although it is not always specific.
Case report: A 45-year-old woman presented with right iliac fossa pain.
Imaging through ultrasonography and MRI initially suggested an ovarian solid-cystic lesion. Surgical intervention revealed a 16 cm mass arising from the uterine fundus. Histopathological examination identified the lesion as a uterine STUMP. This case highlights atypical imaging features that significantly complicated the preoperative diagnosis.
Conclusion: The differentiation of STUMPs from other uterine tumors remains a diagnostic challenge. While imaging findings can suggest the diagnosis, histopathological confirmation is essential. Patients require close surveillance due to the potential risk of recurrence or metastasis.
Keywords: Uterine Smooth Muscle Tumor of Uncertain Malignant Potential (STUMP); Smooth muscle tumor; Diagnostic imaging; Histology.
Citation: Campo-Cossio Marta RdT, Quesada Juan M, Jose Angel GS, María Teresa CC, Daniel José LR. Atypical imaging findings of “uterine smooth muscle tumor of uncertain malignant potential (stump)”: A case report. J Clin Images Med Case Rep. 2025; 6(5): 3597.
Introduction
The 2014 World Health Organization (WHO) classification identifies several types of uterine smooth muscle tumors, including leiomyomas, leiomyosarcomas, uterine smooth muscle tumors of uncertain malignant potential (STUMP), benign metastasizing leiomyomas, and intravenous leiomyomata. This classification identifies STUMPs as smooth muscle tumors with uncertain biological behavior. While they are neither benign nor malignant, they are potentially associated with recurrence or metastasis [1]. Recognizing and differentiating these tumors from benign smooth muscle conditions is crucial. STUMPs are exceptionally rare, and their imaging findings are primarily documented in case reports and small case series. Clinically, they often present with non-specific symptoms such as abnormal uterine bleeding, pelvic pain, or a palpable mass, which further complicate the diagnostic process.
Radiologically, differentiating STUMPs from leiomyomas and leiomyosarcomas is challenging. Ultrasonography is usually the initial diagnostic modality, where STUMPs frequently appear as well-circumscribed lesions with mixed echogenicity and absent posterior acoustic shadowing, which can mimic benign findings [2]. Advanced imaging techniques like contrast-enhanced MRI (CE-MRI) and diffusion-weighted imaging (DWI) are frequently employed but often lack diagnostic specificity [3,4]. Notably, contrast-enhanced MRI has demonstrated superior diagnostic accuracy over DWI in differentiating STUMP from leiomyomas [5]. The role of 18F-fluorodeoxyglucose Positron Emission Tomography (PET) combined with Computed Tomography (CT) remains unclear [6]. Histologically, STUMPs are characterized by features such as mild to moderate cellular atypia, the presence of tumor cell necrosis, and mitotic activity that does not meet the criteria for overt malignancy or benignity. This report presents a case of STUMP with atypical imaging findings that deviated from commonly reported descriptions, emphasizing the importance of a multidisciplinary diagnostic approach. It also contributes valuable insights to the limited body of literature on this rare tumor type.
Case presentation
case involves a 45-year-old woman with no relevant personal or family history who presented to the gynecology emergency department with continuous, stabbing pain in the right iliac fossa for three days, without additional symptoms. The physical examination revealed a soft, depressible abdomen with no signs of peritoneal irritation. Laboratory blood tests showed no significant abnormalities. The initial diagnostic test was a transvaginal and transabdominal ultrasound, which revealed an anteverted uterus with a linear endometrium and a 24 mm subserosa myoma on the posterior wall. In the left para-adnexal area, a bilobed mass measuring 16.3 x 10.4 cm was observed, with one anechoic lobe (7.2 x 8.2 cm) and another with a “ground- glass” appearance containing thin septations (9 x 8.5 cm). No Dppler color flow was detected in either lobe, separated by a 7.8 mm septum. These findings were atypical for a uterine STUMP. Tumor markers and MRI were ordered for further evaluation. The tumor markers were negative, with the following values: (CA125 27.4 U/mL [0-35]; CA19.9 6.1 U/mL [0-37]; LDH 244 U/L [120-246]; Alpha-FP 0.3 ng/mL [0-8.1]; BHCG 1 U/L [0-6]). MRI revealed an 18.3 cm solid-cystic mass in the left ovarian region with heterogeneous contrast enhancement in solid areas; cystic regions showed hemorrhagic content. These findings, along with intra-abdominal fluid, were highly atypical for a benign myoma and did not align with the classic criteria for leiomyosarcoma or STUMP [3]. The tumor displayed well-defined margins, large cystic areas, and significant hemorrhagic content, contrasting with the typical STUMP features of irregular borders and heterogeneous necrosis (Figure 1) [7]. A total hysterectomy with bilateral salpingectomy was performed, which revealed a 16 cm mass adhered to pedicles of approximately 2.5 cm, originating from the uterine fundus and the right cornual region. The fallopian tubes and ovaries appeared normal. The tumor was densely adherent to the inframesocolic omentum and mesenteric root, with looser adhesions to the anterior surface of the rectum and the left pelvic wall. Adhesiolysis and complete tumor removal were achieved. Histopathological examination showed irregular mitotic activity and multifocal atypia characterized by enlarged nuclei and irregular chromatin patterns. These histopathological features confirmed the diagnosis of STUMP, with focal infiltration into the omentum (Figure 2). Given postoperative findings, a post-surgical Ct evaluation was decided, and depending on the results, close follow-up will be considered. Postoperative CT scan was performed two months later, describing postsurgical changes in the pelvis, including a nodular image measuring approximately 25 mm in the left hemipelvis. This finding could not exclude the possibility of an underlying or residual lesion. Subsequently, a PET-CT scan performed one month later showed no metabolic activity suggestive of malignancy associated with this nodular image (Figure 3). The patient was advised to undergo follow-up under gynecologic oncology with quarterly evaluations and regular control CT scans.
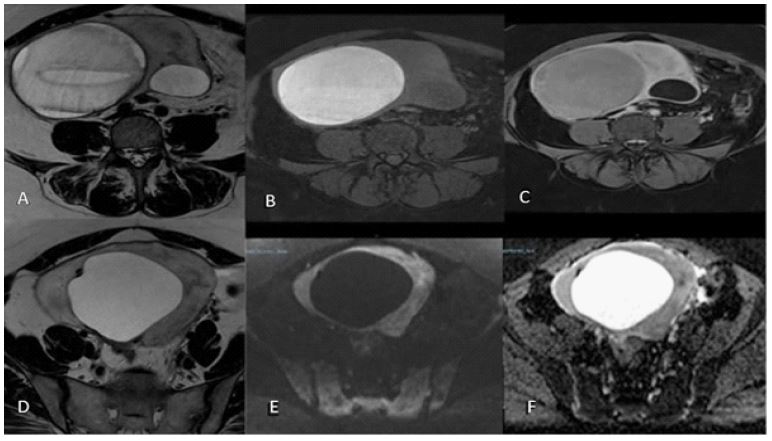
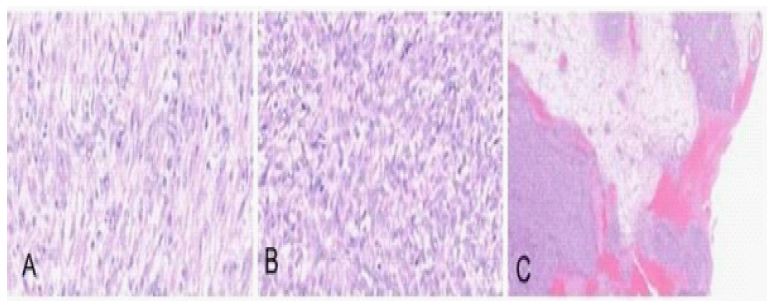
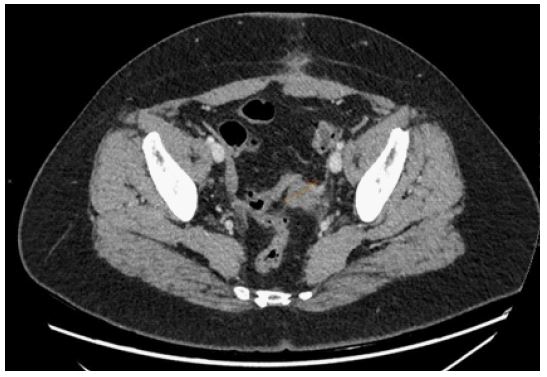
Table 1: Comparison of the histopathological characteristics of leiomyomas, STUMPs, and leiomyosarcomas.
| Histologicalcharacteristics | Leiomyoma | STUMP | Leiomyosarcoma |
|---|---|---|---|
| Mitotic index | Low or absent(typically <5 mitoses/10 HPF) | Low to moderate (5-10 mitoses/10 HPF) | High (≥10mitoses/10 HPF) |
| Cytologic atypia | Absent or minimal | Mild to moderate | Severe, markedatypia |
| Necrosis | Absent | Incomplete coagulative tumor cellnecrosis (CTCN) | Extensive, complete coagulative necrosis |
Table 2: Comparison of the histopathological characteristics of leiomyomas, STUMPs, and leiomyosarcomas.
| Characteristics | Uterine Leiomyoma | STUMP (Smooth MuscleTumor of Uncertain Malignant Potential) | Uterine Leiomyosarcoma |
|---|---|---|---|
| Clinical | Often asymptomatic or presents with mild symptoms such as abnormal uterine bleeding, pelvicpain, or pressure | Variable symptoms: uterine bleeding, pelvic pain, or palpable mass | Pelvic pain, heavyuterine bleeding, systemic symptoms in advanced cases |
| Incidence | Common | Very rareapproximately 0.01% ofhysterectomies or myomectomies | Rare, lessthan 1% of uterine neoplasms |
| Common age of presentation | 30-50 years | 40-50 years | Typically in postmenopausal women,average 50-60 years |
| Radiological (MRI) | Well-defined mass, homogeneous T2 signal, no necrosis; no diffusion restriction | Irregular or well- defined borders, heterogeneous T2 signal, sometimes partial necrosis | Poorlydefined borders, heterogeneous T2 signal, extensive necrosis, significantdiffusion restriction on DWI, highperfusion on CE- MRI |
| DWI/ADCcharacteristics | No diffusion restriction on DWI,high ADC | May showmild to moderate restriction on DWI,variable ADC | Significant restriction on DWI, low ADC |
| Contrast enhancement (CE-MRI) | Homogeneous or mild peripheral enhancement | Irregular or heterogeneous enhancement in solid areas | Intense and heterogeneous enhancement in solid areas, central necrosis |
| Histopathological | Rare or absent mitoses, no cellular atypia, absent necrosis | Low mitotic index(<10 mitoses/10 HPF),mild to moderate atypia, partial non-coagulative necrosis | High mitotic index(>10 mitoses/10 HPF),significant cellular atypia, extensive coagulative tumor necrosis |
| Prognosis | Benign, no risk of recurrence aftercomplete resection | Low to moderate riskof recurrence, rarelymetastatic | Highly aggressive, high risk of recurrence and metastasis |
| Clinical management | Observation or surgery if symptomatic | Surgical resection with strict follow-up | Total hysterectomy, often followed by chemotherapy or radiotherapy dueto high recurrence rate |
Discussion
Uterine STUMPs are rare, comprising approximately 0.01% of all myomectomies and hysterectomies [7]. Differentiating STUMPs from other uterine tumors, such as leiomyomas and leiomyosarcomas, remains challenging from both radiological and histological perspectives [8].
Regarding the diagnoses: Transvaginal ultrasound is the primary imaging modality for evaluating uterine masses, offering details on size, vascularity, and echotexture. Leiomyomas typically appear as well-circumscribed, hypoechoic masses with posterior acoustic shadowing, while STUMPs may exhibit atypical findings, including heterogeneous echogenicity, cystic degeneration, and irregular margins [2]. However, these findings are non-specific and overlap with those of leiomyosarcomas [9]. MRI is the imaging modality of choice for evaluating uterine smooth muscle tumors due to its superior soft-tissue contrast and ability to assess disease extent. A comprehensive MRI protocol should include T1-weighted images (with and without fat suppression) and T2-weighted sequences [4]. These sequences enable the detection of masses and the evaluation of anatomy, mass composition and internal structure. Diffusion-weighted imaging (DWI) assesses the movement of water molecules giving information about cellularity of lesions. High b-value DWI can reveal areas of restricted diffusion, which are more commonly associated with malignancy, while apparent diffusion coefficient (ADC) values provide quantitative data that can help in differentiating between benign and malignant lesions [3]. Contrast-enhanced sequences highlight vascular characteristics, such as increased permeability and irregular neovascularization, which are commonly associated with malignancy. If contrast is contraindicated, T2-weighted sequences combined with high b-value DWI and ADC mapping are essential [10]. Leiomyomas typically appear as well- circumscribed masses with homogeneous T2 signal and uniform enhancement, lacking significant necrosis or restricted diffusion. In contrast, STUMPs and leiomyosarcomas typically exhibit irregular borders, heterogeneous T2 signal intensity, and irregular enhancement patterns, which distinguish them from benign leiomyomas. The presence of coagulative necrosis or scattered necrotic areas can further suggest malignancy [10-12]. Nevertheless, this case showed a number of atypical findings:
-Well-defined margins: Unlike the typical presentation of STUMP with irregular borders, this tumor exhibited well-defined margins.
-Large cystic areas and hemorrhagic content: While T2 signal heterogeneity has been described in STUMPs, the presence of unusually large and well- defined cystic areas with hemorrhagic content is uncommon and more typical of other types of cystic tumors, complicating preoperative diagnosis [4]. Although not performed in this case, PET-CT may provide additional insights. STUMPs often show heterogeneous and moderate FDG uptake, reflecting intermediate metabolic activity. While this uptake is generally lower than in leiomyosarcomas, its variability complicates differentiation from malignant tumors [13]. Pathological definition of STUMP requires at least one of the following: low mitotic index, mild to moderate cytologic atypia, and incomplete coagulative tumor cell necrosis (CTCN) [14,1,15] (Table 1).
Diagnostic challenges and considerations
These findings highlight the variable radiologic presentations of STUMPs and the importance of a multidisciplinary approach for diagnosis and management. A multiparametric MRI approach focusing on features such as necrosis, hemorrhage, and cellularity is crucial for improving diagnostic accuracy [5] (Table 2).
Close histopathologic correlation and rigorous postoperative follow-up are recommended due to the risk of recurrence, especially in tumors with atypical characteristics [16].
Management and monitoring
At present, there are no standardized protocols for the management and monitoring of STUMP patients. It is recommended that post-hysterectomy or myomectomy follow-up occur at least every six months during the first five years, and then annually. Follow-up should include pelvic examination and imaging studies, such as pelvic ultrasound, computed tomography or MRI, along with chest radiography to exclude metastasis [17]. Recurrence has been reported in up to 28% of cases. Identified risk factors for recurrence include prior myomectomy, younger age, atypical mitotic figures, subserosal location, epithelioid differentiation, vascular involvement, and irregular margins [18,19].
Conclusion
This case highlights an atypical radiologic presentation of a uterine STUMP, with imaging findings that did not conform to the classic pattern described in the literature. It emphasizes the importance of considering STUMPs in the differential diagnosis of uterine masses, even when imaging features are not entirely indicative. While MRI is crucial, its diagnostic limitations require confirmation through histopathology, and vigilant follow-up is necessary [16].
Declarations
Inform consent: Written informed consent was obtained from the patient for the publication of this case report and its associated images. Confidentiality of her identity was assured. This process was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki.
Additional information: Nothing to disclose.
References
- Kurman RJ, Carangid ML, Herrington CS, Young RH. WHO classification of tumors of female reproductive organs. 4th ed. Lyon: IARC Press. 2014.
- Liu S, Chang J, Su W, Wang Y, Zhang F, Li H. Imaging characteristics of uterine smooth muscle tumors of uncertain malignant potential: A case report and literature review. J Int Med Res. 2024; 52(9): 1-7.
- Tanaka YO, Nishida M, Tsunoda H, Togashi K. Smooth muscle tumors of uncertain malignant potential and leiomyosarcomas of the uterus: MR findings. J Magn Reason Imaging. 2004; 20(6): 998-1007.
- Sala E, Rockall AG, Freeman SJ, Mitchell DG, Reinhold C. The added role of MR imaging in treatment stratification of patients with gynecologic malignancies: What the radiologist needs to know. Radiology. 2013; 266(3): 717-40.
- Aminzadeh P, Alibrahim E, Dobrotwir A, Foroozmehr F, Ryan J, et al. Multiparametric MR evaluation of uterine leiomyosarcoma and STUMP versus leiomyoma in symptomatic women. Br J Radiol. 2021; 94: 20200483.
- Zhang R, Tian X, Qin L, Lu D, Shen J. High 18F-FDG uptake for uterine smooth muscle tumor of uncertain malignant potential. Clin Nucl Med. 2015; 40: 349-51.
- Guntupalli SR, Ramirez PT, Anderson ML, Milam MR, Bodurka DC, et al. Uterine smooth muscle tumor of uncertain malignant potential: A retrospective analysis. Gynecol Oncol. 2009; 113(3): 324-326.
- Ng JS, Han A, Chew SH, Low JJ. Uterine smooth muscle tumors of uncertain malignant potential: A clinicopathologic review. Int J Gynecol Cancer. 2010; 20(2): 373-6.
- Russo C, Camilli S, Martire FG, Di Giovanni A, Lazzeri L, et al. Ultrasound features of highly vascularized uterine myomas (uterine smooth muscle tumors) and correlation with histopathology. Ultrasound Obstet Gynecol. 2022; 60(3): 269-276
- Lin G, Ng KK, Chang CJ, Wang JJ, Ho KC, et al. Imaging of uterine leiomyosarcomas and their differential diagnosis: Clinical, radiological and pathological correlation. Eur Radiol. 2010; 20(10): 2414-24.
- Yamashita Y, Torashima M, Takahashi M, et al. Hyperintense uterine leiomyoma at T2-weighted MR imaging: differentiation with dynamic enhanced MR imaging and clinical implications. Radiology. 1993; 189: 721-725.
- Cornfield DB, Roberts C, Christopher MJ. Uterine tumors: Comparative MR imaging features. J Magn Reson Imaging. 2018; 48: 1027-36.
- Nagai T, Takahashi K, Takehara K, Noda T, Hirakawa A, et al. Clinical significance of 18F-FDG PET in evaluating uterine smooth muscle tumors: Can it differentiate between leiomyosarcoma, STUMP, and leiomyoma? Eur J Nucl Med Mol Imaging. 2010; 37(4): 706-12.
- Travaglino A, Kurman RJ, Tanaka YO. Prognostic significance of atypical mitotic figures in smooth muscle tumors of uncertain malignant potential. APMIS. 2021;129(4):165- 9.
- Bucuri CE, Ciortea R, Malutan AM, Roman IM, Mocan-Hognogi R, Ferencz J. Smooth muscle tumor of uncertain malignant potential (STUMP): A systematic review of the literature in the last 20 years. Curr Oncol. 2024;31(9):5242–5254.
- Parker WH, Fu YS, Berek JS. Uterine smooth-muscle tumors of uncertain malignant potential. Obstet Gynecol. 1994;83(6):1015-20.
- Leibsohn S, d’Ablaing G, Mishell DR Jr, Schlaerth JB. Leiomyosarcoma in a series of hysterectomies performed for presumed uterine leiomyomas. Am J Obstet Gynecol. 1990; 162(4): 968-76.
- Shim JI, Han AK, Jeon HJ, Park HY, Kim YH, Lee JH, et al. Clinical experience of uterine smooth muscle tumor of uncertain malignant potential in two gynecological centers: Oncological and obstetrical aspects. Eur J Obstet Gynecol Reprod Biol. 2020; 246: 7-13.
- Lapresa-Alcalde MV, Ruiz-Navarro MJ, Sancho de Salas M, Cubo AM. A review and follow-up of uterine smooth muscle tumours of uncertain malignant potential (STUMP): A case series and literature review. Diseases. 2023; 11: 99.