
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 6
Post-traumatic false aneurysm of the thoracic aortic isthmus: Rare location not to be overlooked!
Badr El kassimi*; Abdelkarim Kharroubi
Department of Vascular and Endovascular Surgery, Souss Massa University Hospital Center, Faculty of Medicine and Pharmacy of Agadir, Ibn Zohr University Agadir, Morocco.
*Corresponding Author : El Kassimi Badr
Department of Vascular and Endovascular Surgery, Souss Massa University Hospital Center, Tilila District PC 80060 Agadir, Morocco.
Tel: +212669995681;
Email: Dr.badrelkassimi@gmail.com
Received : Apr 05, 2025
Accepted : May 14, 2025
Published : May 21, 2025
Archived : www.jcimcr.org
Copyright : © Kassimi BE (2025).
Citation: Kassimi BE, Kharroubi A. Post-traumatic false aneurysm of the thoracic aortic isthmus: Rare location not to be overlooked!. J Clin Images Med Case Rep. 2025; 6(5): 3599.
Description
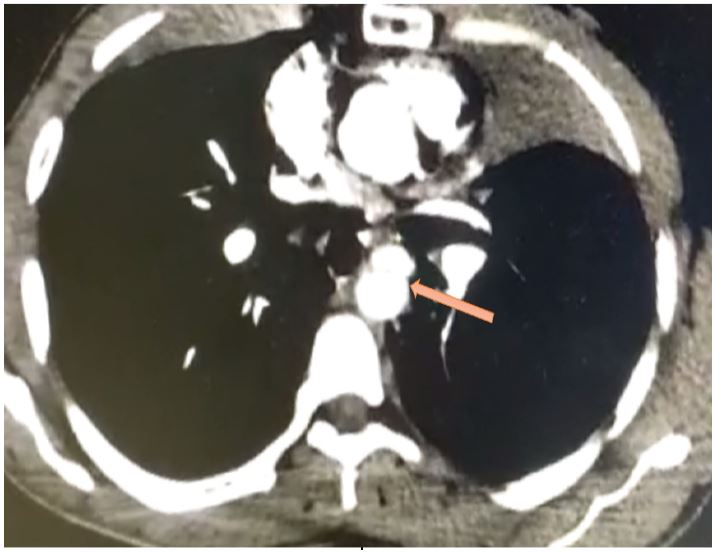
40-year-old patient with no particular history, victim of a free fall from a significant height, with a point of impact on the cranium, thorax, abdomen, right upper limb and pelvis. Thoracic abdominopelvic CT scan (TAP) revealed a grade III post-traumatic false aneurysm with saccular addiction image and regular contours of the aortic isthmus (Figure 1), a pelvic fracture and thrombosis of the right brachial artery due to arterial spasm.
Discussion
Post-traumatic false aneurysm of the thoracic aortic isthmus is rare, it represents 2% of traumatic aortic ruptures [1] and is accompanied by an increased risk of rupture requiring emergency surgery [2]. The isthmus is the most common site of traumatic injuries and accounts for nearly 90% of cases following thoracic trauma [3]. Its relatively immobile position in the thorax explains the percentage of injuries at this level. Angioscanner is the examination of choice with a sensitivity of 98% and a specificity of 100% [4]. It allows us to dare the diagnosis, the evaluation and the staging of the lesions. Grade 3 lesions correspond to a rupture of the three tunics. The interest of our clinical case is to recall the importance of including the false aneurysm of the thoracic isthmus in the attitudes of conducting emergency research in the face of severe trauma patients.
References
- S Bruls, P Goffin, E Creemers, G Trotteur, J Joskin, P Bonnet, J. Defraigne Incidental discovery of a post-traumatic pseudoaneurysm of the aortic isthmus after 15 years of latency. Rev Med Liège. 2010; 65: 11: 603-605.
- Bendjaballah S, Lakehal R, Aimer F, Bouharagua R, Boukarroucha R, Brahami A. Fistulized Aortic Arch Aneurysm in the Left Lung: About a Case. Batna Journal of Medical Sciences. 2018; 5(1): 82-83.
- D Ait Ali Yahia, A Bouvier, C Nedelcu, M Urdulashvili, F Thouveny, C. Ridereau-Zins, et al. Imaging of thoracic aortic trauma. Journal of Diagnostic and Interventional Radiology. 2015; 96: S29-S38,doi.org/10.1016/j.jradio.2013.12.019.
- JE Fishman, D Nunez Jr, A Kane, LA Rivas, WE Jacobs. Direct versus indirect signs of traumatic aortic injury revealed by helical CT: performance characteristics and interobserver agreement. AJR Am J Roentgenol. 1999; 1724: 1027-1031.