
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 6
Transcatheter endovascular covered stent placement for the management of patent ductus arteriosus and coarctation of aorta: An experience with Bentley BeGraft covered stent
Deepali Bangalia; Joshi Siddhartha*; Hemanta Kumar Nayak; Sudipta Bhattacharjya
Department of Pediatric Cardiology, The Mission Hospital, Durgapur, West Bengal, India.
*Corresponding Author : Joshi Siddhartha
Department of Pediatric Cardiology, The Mission Hospital, Durgapur, West Bengal, India.
Email: dr.siddharthajoshi@gmail.com
Received : Apr 21, 2025
Accepted : May 15, 2025
Published : May 22, 2025
Archived : www.jcimcr.org
Copyright : © Siddhartha J (2025).
Abstract
Co-existence of coarctation of aorta and patent ductus arteriosus is very rare (less than 1%). There are two approaches for intervention in CoA with PDA include surgical and transcatheter (TC). In TC single stage covered stent is emerging as newer modality over conventional approach in adult. Here we present one such case where we have used Bentley Begraft Aortic endovascular covered stent.
Citation: Bangalia D, Siddhartha J, Kumar Nayak H, Bhattacharjya S. Transcatheter endovascular covered stent placement for the management of patent ductus arteriosus and coarctation of aorta: An experience with Bentley BeGraft covered stent. J Clin Images Med Case Rep. 2025; 6(5): 3601.
Background
Co-existence of coarctation of aorta and patent ductus arteriosus is very rare (less than 1%) [1]. Surgical correction is the gold standard of treatment in infancy and childhood. But in adults and adolescents endovascular stenting has now emerged as a viable and less invasive alternative due to faster recovery and reduced trauma. This case study aims to describe the successful simultaneous closure of PDA and CoA using a Bentley BeGraft Aortic endovascular covered stent in an adult patient. However, use of interventional procedures in either sequential or simultaneous sessions has been reported in previous studies [2-5].
Case summary
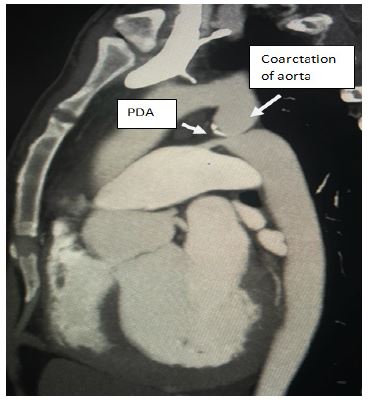
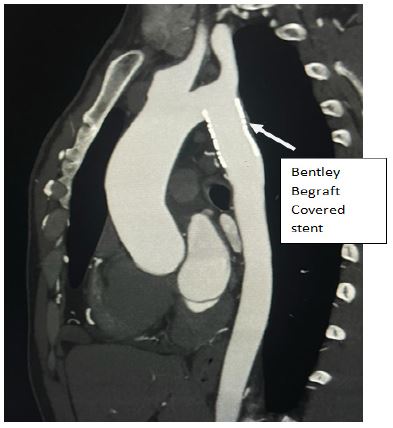
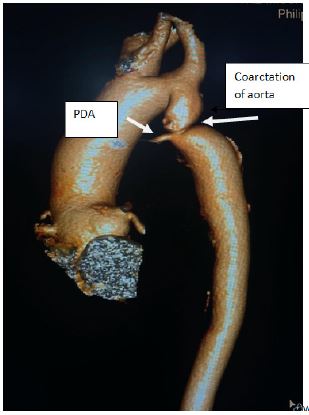
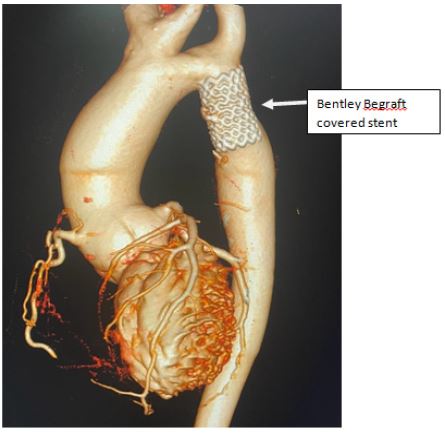
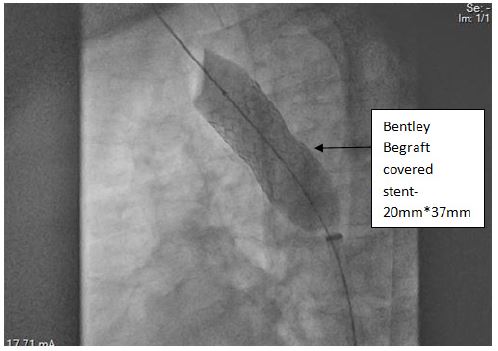
A 36 year old male patient presented with exertional dyspnea (NYHA class 2), headache and hypertension. Transthoracic echocardiography (TTE) showed Bicuspid aortic valve with mild AR, Severe post Subclavian Coarctation of Aorta, 4mm PDA with moderate Left ventricular systolic dysfunction. Computed Tomography (CT) imaging confirmed echocardiographic findings. Patient was taken for coarctation stenting with covered stent through right femoral artery. A Bentley BeGraft Aortic endovascular covered stent 20 mm x 37 mm was taken over the Amplatz wire through 14 F Lifetech ASD delivery sheath and angiogram was obtained through the side port of the sheath to confirm the stent position, then the balloon was inflated till the full disappearance of waist (upto 6 ATM pressure). Post procedure patient was shifted to Cardiac Care Unit, Milrinone and Lasix infusion was given for 48 hrs and discharged on fourth post operative day. The patient’s overall condition improved significantly post intervention, with enhanced exercise tolerance and reduced fatigue at 1 year of follow up.
Discussion
Earlier the preferred modality for a combination of Coarctation of Aorta and PDA in adults was surgery. Sequential interventional therapy has been reported in literature with coarctoplasty followed by PDA device closure. Use of covered stent in adults for this combination is gaining popularity due to being minimally invasive, reduced short and long term complications and can be accomplished in single sitting. Hekim et al has described the largest series of twelve such patients who had undergone successful simultaneous closure of CoA and PDA with the use of covered Cheatham Platinum stents [5]. In our case, we have used Bentley BeGraft PTFE (Polytetrafluoroetylene) covered stent. Age of patient, anatomy of Coarctation of Aorta, size and shape of PDA play a pivotal role in deciding the modality of treatment.
Conclusion
Endovascular covered stent placement can be a suitable alternative to surgery for simultaneous treatment of PDA & coarctation of aorta in adult population. However proper hardware and patient selection is the key to the procedural success. Though the morbidity, mortality and restenosis rates are negligible, stent embolization, fracture and aortic dissection can lead to catastrophic complications.
References
- Toro-Salazar OH, Steinberger J, Thomas W, Rocchini AP, Carpenter B, Moller JH. Long-term follow-up of patients after coarctation of the aorta repair. Am J Cardiol. 2002; 89(5): 541-7. doi: 10.1016/s0002-9149(01)02293-7. PMID: 11867038.
- Celebi A, Yalcin Y, Erdem A, Zeybek C, Akdeniz C, Polat TB. Successful transcatheter balloon dilatation of coarctation of aorta and coil occlusion of patent ductus arteriosus in a single catheterization procedure. Turk J Pediatr. 2007; 49: 94–7.
- Geggel RL, Hijazi ZM, Rhodes J. Interventional cardiac catheterization therapy for combined coarctation of the aorta and patent ductus arteriosus:successful outcome in two infants. Cathet Cardiovasc Diagn. 1996; 38: 67–70.
- Hakim F, Hawelleh AA, Goussous Y, Hijazi ZM. Simultaneous stent implantation for coarctation of the aorta and closure of patent ductus arteriosus using the Amplatzer duct occluder. Cathet Cardiovasc Interv. 1999; 47: 36–8.
- Hekim Yılmaz E, Bulut MO, Küçük M, Yücel İK, Erdem A, Çelebi A. Use of covered stents in simultaneous management of coarctation of the aorta and patent ductus arteriosus. Anatol J Cardiol. 2018; 19(4): 332-336. doi: 10.14744/AnatolJCardiol.2018.61257. Epub 2018 Mar 21. PMID: 29578201; PMCID: PMC5998845.