
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Exploring the fusion of acute limb ischemia, myocardial infarction & pulmonary embolism
Summaya Fatima; Sadaf Hanif Musani*
Department of Internal Medicine, The Aga Khan University Hospital, Karachi, Pakistan.
*Corresponding Author : Sadaf Hanif Musani
Department of Internal Medicine, The Aga Khan University Hospital, Karachi, Pakistan.
Email: sadaf.hanif@aku.edu
Received : Apr 10, 2025
Accepted : May 16, 2025
Published : May 23, 2025
Archived : www.jcimcr.org
Copyright : © Musani SH (2025).
Abstract
This case report describes the concurrent presentation of Acute Limb Ischemia (ALI), ST-Elevation Myocardial Infarction (STEMI), and pulmonary embolism in a 75-year-old male. This rare constellation of conditions highlights the diagnostic and therapeutic challenges encountered in managing such a complex clinical scenario. The patient was presented with left leg swelling, discoloration, and numbness, along with shortness of breath. ECG findings suggested a late anterior wall STEMI. Laboratory investigations confirmed elevated cardiac biomarkers. Transthoracic echocardiography demonstrated an ejection fraction of 25% and a right atrial thrombus, which subsequently embolized to the pulmonary circulation during the study. The patient was treated with vasopressors, anticoagulation, and intravenous tissue Plasminogen Activator (tPA). Despite treatment, the patient remained hemodynamically unstable. Limb amputation was planned but declined by the family. This case underscores the importance of considering a broad differential diagnosis in patients presenting with overlapping symptoms of these critical conditions and emphasizes the need for prompt and aggressive management.
Keywords: Acute limb ischemia; Pulmonary embolism; Stemi.
Citation: Fatima S, Musani SH. Exploring the fusion of acute limb ischemia, myocardial infarction & pulmonary embolism. J Clin Images Med Case Rep. 2025; 6(5): 3603.
Introduction
Acute Limb Ischemia (ALI) is a critical condition where blood flow to a limb is severely compromised, threatening its viability. This life-threatening situation can arise from various causes, including arterial embolism, where a blood clot travels from elsewhere in the body and blocks a limb’s artery, or in-situ thrombosis, where a clot forms within the artery itself. Other less common causes include vascular trauma and aneurysmal thrombosis. Despite advancements in reperfusion therapies aimed at restoring blood flow, ALI carries significant risks, including limb loss with amputation rates ranging from 10-30% and a 30-day mortality rate reaching up to 13.9% [1,2]. Pulmonary Embolism (PE), another critical condition, occurs when a blood clot, typically originating from a deep vein thrombosis in the legs, travels to the lungs and obstructs pulmonary arteries. PE can range from mild to life-threatening, with approximately 15% of in-hospital deaths attributed to this condition [3]. Both PE and ST-Elevation Myocardial Infarction (STEMI) can present with overlapping symptoms, such as shortness of breath and chest pain, making accurate diagnosis is crucial. Prompt recognition and immediate medical intervention are essential for both ALI and PE to minimize the risk of severe complications and improve patient outcomes [4,5].
Case presentation
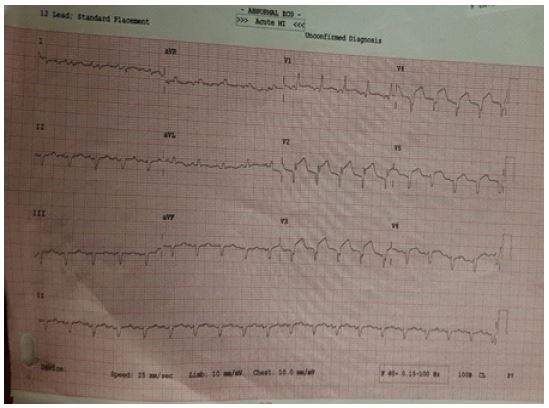
A 75-year-old male presented with a two-day history of left leg swelling, discoloration, numbness, accompanied by shortness of breath. Physical examination revealed a cold and mottled left lower limb with absent pulses except for the femoral pulse. Arterial Doppler ultrasound confirmed these findings, indicating significant arterial occlusion in the left leg. Electrocardiogram (ECG) showed ST-segment elevations in leads V1-V5, indicative of a late anterior wall myocardial infarction (STEMI). Laboratory investigations revealed elevated cardiac biomarkers, including troponin (6077 ng/L) and creatine phosphokinase (CPK) (9984 IU/L), along with an elevated creatinine level (1.8 mg/dL). Based on these findings, the patient was diagnosed with both STEMI and Acute Limb Ischemia (ALI). He was immediately initiated on nor-epinephrine on 0.18 mcg/kg/min and Vasopressin at 0.04 mic/kg/min to support low blood pressures and Enoxaparin subcutaneously in renally adjusted doses to prevent further clot formation. Supplemental oxygen (2 liters) was also administered. A bedside echocardiogram revealed a significantly reduced ejection fraction of 25% and the presence of a right atrial thrombus. During the echocardiogram, the thrombus was observed to embolize into the pulmonary circulation, resulting in a pulmonary embolism. No evidence of a right-to-left shunt was noted. Following the embolic event, the patient’s hemodynamic stability deteriorated. Intravenous tissue Plasminogen Activator (tPA) was administered to dissolve the clot in the pulmonary artery. Subsequently, the patient’s condition improved, and the requirement for vasopressors was reduced. Despite these interventions, limb amputation was considered necessary due to the severity of the limb ischemia. However, the patient’s family declined the procedure and left against medical advice. On follow up it was informed by the family that patient expired the next day due to worsening acidosis and shock.



Discussion/conclusion
Pulmonary Embolism (PE) is the blockage of the pulmonary artery, typically caused by a Deep Vein Thrombosis (DVT). While other causes exist, such as air embolism and amniotic fluid embolus, DVT remains the most common. The clinical presentation of PE varies widely depending on the size of the embolus. Small emboli may be asymptomatic or cause mild hypoxia, while larger emboli can lead to significant hypoxia, tachycardia, tachypnoea, and even hypotension. Other potential ECG findings include S1Q3T3 pattern, right bundle branch block (RBBB), and prominent pulmonary P waves. Massive PE, characterized by hemodynamic instability, is a medical emergency requiring immediate thrombolysis. Sub-massive PE is defined as pulmonary arterial occlusion without hemodynamic compromise. PE can mimic ST-elevation myocardial infarction (STEMI), a phenomenon described in multiple case reports [7,8]. A 2018 systemic review demonstrated that PE frequently mimics anterior wall MI. The review detailed potential mechanisms for myocardial ischemia in the presence of PE, including acute increases in right ventricular pressure, leading to right ventricular dilatation and subsequent myocardial ischemia. Additionally, hypoxia, hypotension, and catecholamine surges can contribute to myocardial ischemia [8]. This case report presents a unique clinical scenario of a patient with concurrent STEMI, acute limb ischemia, and pulmonary embolism. This rare combination likely reflects an underlying hypercoagulable state with grave potential outcomes. Acute limb ischemia is characterized by a sudden decrease in limb perfusion, threatening limb viability. It is primarily caused by arterial embolism or in-situ thrombus formation within an atherosclerotic artery. Chronic aortoiliac obliteration, also known as Leriche syndrome, is a severe form of atherosclerotic disease affecting the distal aorta, iliac, and femoropopliteal vessels. It is typically characterized by the triad of claudication, impotence, and absent femoral pulses. While Leriche syndrome is rarely caused by venous thromboembolism, a rare case report described a 58-year-old man presenting with bilateral lower limb pain and shortness of breath, attributed to bilateral pulmonary embolism and thrombotic occlusion at the aortoiliac bifurcation. Notably, this occurred in the absence of a right-to-left intracardiac shunt. In our case, the patient initially presented with shortness of breath and left lower limb pain. Subsequent investigations revealed STEMI and acute limb ischemia. An incidental finding of an atrial thrombus during echocardiography led to its embolization to the pulmonary circulation, resulting in acute PE. Although no right-to-left shunt was evident on transthoracic echocardiography, a bubble study should be considered to rule out this possibility. The case presents a highly unusual combination of STEMI, acute limb ischemia, and pulmonary embolism, a constellation of conditions not previously reported in the literature to our knowledge. Interestingly, the acute PE developed during the hospital stay, following the initial presentation of STEMI and limb ischemia.
References
- Li R, Ling S, Xu B, Wei W, Yu S, et al. Characteristics and clinical indicators of concomitant venous thromboembolism in acute limb ischemia. Int Angiol. 2021; 40(1): 9-17.
- Natarajan B, Patel P, Mukherjee A. Acute Lower Limb Ischemia-Etiology, Pathology, and Management. Int J Angiol. 2020; 29(3): 168-74.
- Hussain SMA. Lung cancer embolization causing acute limb ischemia: a case report. J Med Case Rep. 2023; 17(1): 56.
- Marginean A, Haines JF, Perez-Tamayo RA, Bechara C, Darki A. Pulmonary Embolism Complicated by Acute Limb Ischemia Managed by Surgical Pulmonary Embolectomy. Cureus. 2021; 13(4): 14598.
- Siddiqa A, Haider A, Jog A, Yue B, Krim NR. Pulmonary Embolism Presenting as ST-Elevation Myocardial Infarction: A Diagnostic Trap. Am J Case Rep. 2020; 21: 927923.
- Mohamed A, Mattsson G, Magnusson P. A case report of acute Leriche syndrome: aortoiliac occlusive disease due to embolization from left ventricular thrombus caused by myocarditis. BMC Cardiovascular Disorders. 2021; 21(1): 220.
- Livaditis IG, Paraschos M, Dimopoulos K. Massive pulmonary embolism with ST elevation in leads V1-V3 and successful thrombolysis with tenecteplase. Heart. 2004; 90(7): 41.
- Li YS, Li YC. Simultaneous acute limb ischemia related to acute Leriche syndrome and pulmonary embolism without existing patent foramen ovale: A case report. BMC Cardiovasc Disord. 2021; 21(1): 465.