
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 6
Facial cellulitis as the presentation of acute maxillary sinusitis
Smadar Goldfarb1; Fadi Abdinnour1; Elchanan Parnasa1; Aviv Talmon1,2; Limor Rubin1,2*
1Department of Medicine, Hadassah Medical Organization, Faculty of Medicine, Hebrew University of Jerusalem, Israel.
2Allergy and Clinical Immunology Unit, Department of Medicine, Hadassah Medical Organization, Faculty of Medicine, Hebrew University of Jerusalem, Israel.
*Corresponding Author : Limor Rubin, MD
Allergy and Clinical Immunology Unit, Department of Medicine, Hadassah-Hebrew University Medical Center, Jerusalem, Israel.
Tel: 972-054-7585029;
Email: limorlaz@gmail.com
Received : Apr 25, 2025
Accepted : May 16, 2025
Published : May 23, 2025
Archived : www.jcimcr.org
Copyright : © Rubin L (2025).
Keywords: Sinusitis; Cellulitis; Angioedema.
Abbreviations: ER: Emergency room; CRP: C reactive protein.
Citation: Goldfarb S, Abdinnour F, Parnasa E, Talmon A, Rubin L. Facial cellulitis as the presentation of acute maxillary sinusitis. J Clin Images Med Case Rep. 2025; 6(5): 3604.
Description
A healthy 50-year-old man was admitted to the emergency room (ER) with a history of 38 ͦC fever and a painful forehead, cheek, and lips edema that started several hours before his admission. Two weeks preceding his admission, the patient suffered from a flu-like illness with symptoms of fatigue, myalgia, and shortness of breath. The patient tested negative for Coronavirus disease-2019 (COVID-19) by polymerase chain reaction test. The patient denied any itchiness or allergic medical background and ruled out any contact with a new or potentially allergenic substances. His vital signs were normal, with no respiratory distress. Physical examination revealed angioedema of his right forehead and cheek, nose, and upper lip. No rash was observed, and no swelling of the larynx. His C reactive protein (CRP) level was 12 mg/dl (normal value <5 mg/dl), on complete blood count (CBC) he had mild leukocytosis with neutrophilia (leukocytosis of 18 x 109/L with 83.2% neutrophils). All other laboratory results were within normal limits. The patient was discharged after a short observation with a working diagnosis of allergic reaction and oral antihistamine treatment (loratadine 10 mg once daily, for 5 days) was initiated.
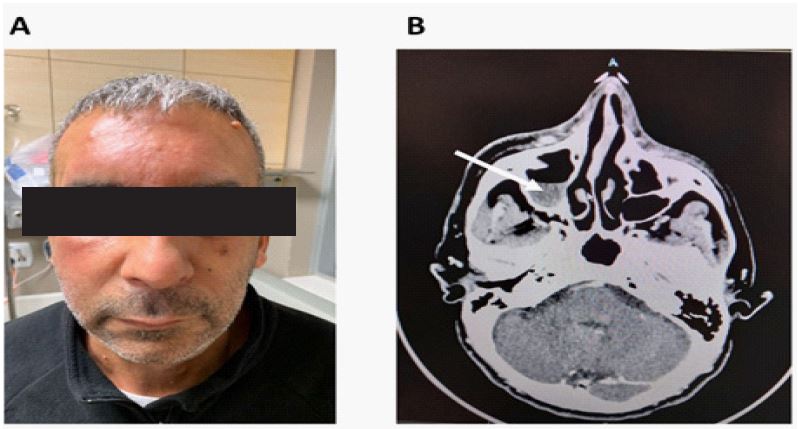
24 hours later, the patient returned to the ER due to persistent fever and deterioration in facial swelling. The patient presented with a sub-febrile fever (37.2oC), and tachycardia (130 BPM), blood pressure and saturation were within normal limits. Physical examination was prominent for significant angioedema of his forehead, cheeks, lips, and upper neck (Figure 1A), accompanied by skin erythema, warmness, and tenderness. His laboratory results revealed an elevation in CRP marker to 16 mg/dl and leukocytosis to 19 x 109/L and therefore, cellulitis diagnosis was made. To assess the degree of underlying tissue involvement and to rule out superior vena cava syndrome an iodine contrast head, neck, and chest computerized tomography (CT) scan was performed. There was no evidence of deep tissue involvement or venues occlusion, however opacification of the right maxillary sinus was observed, consistent with maxillary sinusitis (Figure 1B). Intravenous Cefazolin treatment was initiated with significant rapid clinical and laboratory improvement within 48 hours. Hence, the patient was discharged to complete the antibiotic course orally. Upon one-week follow up the patient had complete clinical and laboratory resolution with no further complications.
Orbital and pre-orbital cellulitis are known and well-described complications of paranasal sinusitis [1]. In some cases, osteomyelitis of the frontal bone associated with a subperiosteal abscess, deep tissue and skin involvement known as a ‘pott puffy tumor’ occurs - a serious condition with a risk above 70% for intracranial complications [2]. However mild facial cellulitis (not involving the orbit area) in healthy adults as a manifestation of maxillary sinusitis is rare [3,4], but since sinusitis can easily be diagnosed and treated, clinicians should search for it in the case of non-allergic angioedema or facial cellulitis.
Author contributions: SG: Investigation, Writing - Original Draft; FA: Investigation, Writing - Original Draft; AT: Investigation, Writing - Original Draft; LR: Investigation, Writing - Review & Editing.
References
- Chaiyasate S, Fooanant S, Navacharoen N, Roongrotwattanasiri K, Tantilipikorn P, Patumanond J. The complications of sinusitis in a tertiary care hospital: types, patient characteristics, and outcomes. Int J Otolaryngol. 2015; 2015: 709302. DOI: 10.1155/2015/709302
- Koltsidopoulos P, Papageorgiou E, Skoulakis C. Pott’s puffy tumor in children: A review of the literature. Laryngoscope. 2020; 130(1): 225-231. DOI: 10.1002/lary.27757
- Yemisen M, Sagit M, Karakas O. Facial bullous cellulitis caused by acute sinusitis. Int J Infect Dis. 2009; 13(6): e525-6. DOI: 10.1016/j.ijid.2009.02.010
- Lin IH, Huang IS. Nasal septal abscess complicated with acute sinusitis and facial cellulitis in a child. Auris Nasus Larynx. 2007; 34(2): 241-243. DOI: 10.1016/j.anl.2006.07.006