
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
An infant with unusual cause of hepatic portal venous gas: A case report
Pinki Alhyan1*; Subham Garg1; Mridu Jain Sehgal1; Jagpreet Singh Bhatia2; Saurabh Aggarwal2; Sidra Noor4
1Senior Resident, Department of Pediatrics, Sehgal Neo Hospital, Meera Bagh, Paschim Vihar, Delhi, India.
2Consultant, Department of Pediatrics, Sehgal Neo Hospital, Meera Bagh, Paschim Vihar, Delhi, India.
3Ist Year Resident, Department of Pediatrics, Sehgal Neo Hospital, Meera Bagh, Paschim Vihar, Delhi, India.
*Corresponding Author : Pinki Alhyan
Senior Resident, Department of Pediatrics Sehgal Neo Hospital, Meera Bagh, Paschim Vihar, Delhi 110063, India.
Tel: 8375838674;
Email: drpinkialhyan0604@gmail.com
Received : Apr 26, 2025
Accepted : May 19, 2025
Published : May 26, 2025
Archived : www.jcimcr.org
Copyright : © Alhyan P (2025).
Abstract
Hepatic Portal Venous Gas (HPVG) is an uncommon radiological finding in infants. Its identification may indicate the presence of serious underlying conditions, such as necrotizing enterocolitis, bowel ischemia, bowel wall rupture and infarction, which may require parenteral nutrition, antibiotics or surgery. Here, we are presenting a case of a 2-month-old male with an incidental ultrasonographic finding of HPVG, subsequent analysis revealed a milk protein allergy as the underlying cause. Although it is an infrequent etiology of HPVG, it should be kept in mind due to its benign course and for the prevention of unnecessary testing and interventions.
Keywords: HPVG; Milk protein allergy; Ultrasonographic finding; Infant.
Abbreviations: HPVG: Hepatic Portal Venous Gas; CMPA: Cow Milk Protein Allergy; USG: Ultrasound; CRP: C -reactive protein; CT: Computed Tomography.
Citation: Alhyan P, Garg S, Jain Sehgal M, Singh Bhatia J, Aggarwal S, et al. An infant with unusual cause of hepatic portal venous gas: A case report. J Clin Images Med Case Rep. 2025; 6(5): 3605.
Introduction
The presence of Hepatic Portal Venous Gas (HPVG) on radiologic imaging is a grave prognostic indicator, often associated with critical abdominal pathology necessitating immediate surgical intervention. Reports of HPVG in medical literature are rising, typically in conjunction with life threatening conditions [1]. A diagnosis of HPVG can indicate serious conditions like necrotizing enterocolitis, ischemic colitis, or bowel rupture. However, it is crucial to consider benign causes [2]. In this case report we present a frequently observed benign condition in infants that can also manifest as HVPG. Cow’s Milk Protein Allergy (CMPA) is a prevalent condition in infancy, affecting up to 15% of infants [3]. Studies indicate a CMPA prevalence of 2-3% in children from developed nations, ranking among the top five childhood food allergens in south east Asia [4]. Other studies report a prevalence ranging 2% to 7.5% [5]. CMPA should be considered in infants consuming formula or bovine milk, however it can also manifest in exclusively breastfeed infants. The incidence of CMPA in breastfeed infants is reported to range from 0.4% to 0.5%, with some studies indicating a prevalence as high as 2.1% [3]. The precise immunologic mechanisms underlying the pathogenesis of CMPA remain elusive. However, it is established that CMPA arises from both Ige-and non-Ige-mediated immune responses. Ige-mediated CMPA, characterized as an immediate type I hypersensitivity reaction, typically manifests within minutes to two hours post ingestion of cow’s milk. Conversely, non-Ige- mediated CMPA present as a delayed type IV hypersensitivity reaction. In individuals exhibiting non-Ige-mediated responses, the presence of CD8+ and CD4+ lymphocytes, along with eosinophils, has been observed throughout all three layers of the colonic mucosa. Lymphocyte transformation assays in these infants have revealed circulating memory cells, indicative of T-cell involvement in CMPA pathogenesis [6].
Case presentation
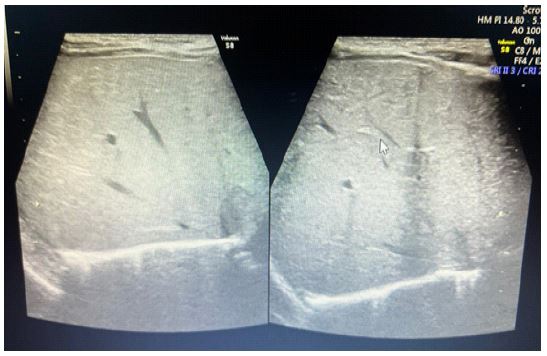
A 2-month-old full term male infant, delivered via LSCS, a follow up case of our OPD, who could not be breastfeed, started on formula feed but showed signs of intolerance since 10th day of life, then started on soy based, milk free, lactose free formula milk. Still signs of intolerance persist. Hence changed to Extensively Hydrolyzed Formula milk. But now admitted with two days history of vomiting and one day history of multiple episodes of loose stool, fever, lethargy along with decreased oral acceptance. Child had a reported birth weight of 3.007 kg and the most recent weight following admission was 3.3 kg. At the time of admission, the child was lethargic, dehydrated and had acidotic breathing. Cardiopulmonary and Neurological examination showed no abnormal features. He presented with soft, mildly distended abdomen with normoactive bowel sounds and no abdominal tenderness to palpation on physical examination. Laboratory analysis showed that white blood cell counts was 29500 thou/mmᶟ (5-15/mmᶟ). The proportion of neutrophils was 47.40% (11-44%), the proportion of lymphocytes was 35.70% (40-80%) and the red blood cell count was 3.46 mill/mmᶟ (3.00-4.50). The hemoglobin level was 10.70 g/dl (9.40-13.00), platelet count was 7.90 thou/mmᶟ (210-650), and the C-Reactive Protein (CRP) level was 178 mg/l (0-5). Serum sodium and potassium levels were 128.20 (139-146) / 2.68 (4.1-5.3) mg/dl. Stool examination showed the absence of reducing substances. Liver and kidney function, TORCH screening and urine routine analysis, lumbar puncture revealed no significant abnormality. X – ray abdomen erect view showed multiple dilated air-filled bowel loops s/o Subacute Intestinal Obstruction (Figure 1). Mildly prominent content filled peristaltic bowel loops seen in central and lower abdomen on Ultrasound (USG) Whole Abdomen. The child was managed conservatively with fluid resuscitation and intravenous antibiotics (Injection Pipas and Amikacin). On the 2nd day of admission antibiotics upgraded to Inj. Meropenem in view of worsening, received sodium bicarbonate correction as metabolic acidosis persist (pH was 7.25, Bicarbonate was 11.40, Base Excess was -17.3) even after fluid resuscitation and Stocks solution given for potassium correction as hypokalemia (serum potassium-2.49) persist even double potassium correction given via maintenance IV Fluid. Gradually, the child was improved symptomatically, abdominal distension settled. Minimal feed started with extensively hydrolyzed formula milk followed by gradually increased. Following this on day of admission – 5th, developed bloody mucoid stool with increased abdominal distension. Repeat investigations done. White blood cell count was 22000, platelet count was 7.69, CRP – 105, serum sodium and serum potassium was 132/2.9, and serum procalcitonin was 57.46. USG Whole Abdomen shows small bowel obstruction with suspicious air within the bowel wall with portal venous gas – possibility of Necrotizing Enterocolitis (Figure 2). No pathogens detected on stool multiplex PCR. Managed with fluid resuscitation, Antibiotics upgraded to injection colistin, sodium bicarbonate correction given in view of persistent metabolic acidosis (pH was 7.15, Bicarbonate was 12.20, Base Excess was -14.10) and potassium corrected by double potassium given via maintenance intravenous fluid. Pediatric gastroenterologist opinion taken. Advised for X – ray abdomen erect view, s/o distended bowel loops (Figure 3) and start Amino Acid based hypoallergenic formula milk once child was improved clinically. Child gradually improved with the given treatment. Minimal feed started with the amino acid-based formula milk, tolerated well then feed increased gradually. After giving 10 days of antibiotics. Investigations repeated. White blood cell count was 11600, CRP was 8.35, serum procalcitonin was 0.32, serum sodium and serum potassium was 140 / 3.63 and blood gas normalized. Repeat USG Whole Abdomen done s/o normal study and no portal venous gas seen (Figure 4). The child was stable, tolerated oral feed without any complications and was discharged after proper counseling of parents. The child’s condition remained stable with normal weight gain on follow up after one week.



Discussion
HVPG, while infrequently diagnosed in infants, is often associated with severe pathologies including necrotizing enterocolitis, bowel ischemia, bowel infarction and bowel wall rupture. Milder conditions such as hypertrophic pyloric stenosis and milk or food protein allergy can also cause HVPG [2,7]. The pathophysiology of HPVG remains incompletely understood. Several hypotheses exist, the most prominent being: a) Increased intra-intestinal pressure leading to portal capillary air bubble migration, b) Disruption of the intestinal mucosa, allowing gas produced by luminal microorganisms to enter the mesenteric and portal venous systems, c) Presence of gas producing bacteria within abdominal inflammatory processes, such as enteritis or acute appendicitis [8]. Following bacterial translocation, hydrogen gas accumulating within the intestinal wall causes pneumatosis intestinalis, radiographically appearing as bowel wall latencies [9]. Portal venous gas subsequently disseminates to intrahepatic branches and the peripheral liver parenchyma in a non-dependent fashion, predominantly in the left lobe and anterior right lobe [1,8]. Abdominal ultrasonography demonstrates high sensitivity and efficacy in identifying HPVG. Characteristic ultrasonographic findings include hyperechoic particles within the portal venous system and hyperechoic foci within the hepatic parenchyma. While abdominal radiography may reveal HVPG in advanced disease stages with significant gas accumulation, ultrasonography offers superior diagnostic capabilities in the early detection of this condition [7]. In adults Computed Tomography (CT) is the established benchmark for diagnosing HPVG. Its utility lies in facilitating early HPVG detection and potential etiology determination. Specific CT imaging parameters, such as employing the lung window setting, enhance the visualization of even small quantities of air within the hepatic parenchyma. In pediatric populations, CT is avoided due to significant radiation exposure. Consequently, ultrasound, a safe and readily repeatable modality, is preferred for both initial diagnosis and subsequent monitoring of HVPG [8]. In infants, consideration should be given to benign etiologies of HVPG, such as milk protein allergy [2]. Cow’s milk protein allergy (CMPA) is a prevalent condition in infancy, affecting up to 15% of infants [3]. Studies indicate a CMPA prevalence of 2-3% in children from developed nations, ranking among the top five childhood food allergens in southeast Asia [4]. Other studies report a prevalence ranging 2% to 7.5% [5]. Reports of milk allergy causing HPVG rare in literature. In our case diagnosis of milk protein induced HPVG was made through the exclusion of alternate etiologies. FollowFollowing the elimination of milk protein from the patient diet, both clinical symptoms and ultrasonographic findings consistent with HPVG resolved. Clinical presentation and symptom severity in CMPA are variable, yet prognosis is typically favorable following the elimination of cow’s milk protein. Although the majority of infants with CMPA tolerate extensively hydrolyzed formula. Approximately 10% require amino acid-based formula, particularly those exhibiting severe enteropathy [10], as illustrated in our case. The diagnosis of HPVG in neonates is typically a cause for concern due to associated morbidity, mortality and the often-urgent need for intervention. However, as illustrated in our case, HVPG can sometimes occur as an incidental finding from a benign etiology and may not require surgical evaluation and treatment [8]. Possibility of benign etiologies should be considered in the absence of serious bowel disease, to minimize unwarranted interventions [10]. In our case raised inflammatory markers in the form of increased TLC and raised CRP might be due to gut inflammation. Abdominal ultrasonography demonstrates high sensitivity and efficacy in identifying HPVG [7]. In the absence of surgical indications, abdominal ultrasound is recommended within 1-2 days after the diagnosis. Further imaging, such as abdominal radiography or CT, is not required, particularly if subsequent ultrasound examinations reveal resolution of abnormalities [8].
Conclusion
The presence of HPVG in radiologic imaging does not invariably signify a severe underlying condition, it may be observed in relatively benign cases, as in our case. HPVG itself does not warrant surgical intervention; treatment is primarily determined by the underlying disease. Prognosis is dictated by the underlying pathology and is not affected by the presence of HVPG.
References
- S1. Abboud B, El Hachem J, Yazbeck T, Doumit C. Hepatic portal venous gas: physiopathology, etiology, prognosis and treatment. World J Gastroenterol. 2009; 15(29): 3585-90. Doi: 10.3748/wjg.15.3585.
- Siddique Z, Thibodeau R, Jaromir A, Hananiah R. Pediatric milk protein allergy causing hepatic portal venous gas: Case report. Radial Case Rep. 2020; 16(2): 246-249. Doi: 10.1016/j.radcr.2020.11.002.
- Brill H. Approach to milk protein allergy in infants. Can Fam Physician. 2008; 54: 1258-64.
- Aw M. Cow’s milk protein allergy. Southeast Asian J Trop Med Pub Health. 2014; 45(1): 65-8.
- Vanderplas Y, Brueton M, Dupont C, Hill D, Isola Uri E, et al. Guidelines for the diagnosis and management of cow’s milk protein allergy in infants. Arch Dis Child. 2007; 92: 902-8.
- Mousam G, Kamat D. Cow’s Milk Protein Allergy. Clin Pediatr (Phila). 2016; 55(11): 1054-63. doi: 10.1177/0009922816664512.
- Yuan K, Chen QQ, Zhu YL, Luo F. Hepatic portal venous gas without definite clinical manifestations of necrotizing enterocolitis in a 3-day-old full-term neonate: A case report. World J Clin Cases. 2021; 9(30): 9269-9275. doi: 10.12998/wjcc.v9.i30.9269.
- Barczuk-Falęcka M, Bombiński P, Majkowska Z, Brzewski M, Warchoł S. Hepatic Portal Venous Gas in Children Younger Than 2 Years Old - Radiological and Clinical Characteristics in Diseases Other Than Necrotizing Enterocolitis. Pol J Radiol. 2017; 82: 275-278. doi: 10.12659/PJR.899995.
- Thompson AM, Bizzarro MJ. Necrotizing enterocolitis in newborns: pathogenesis, prevention and management. Drugs. 2008; 68(9): 1227-38. doi: 10.2165/00003495-200868090-00004.
- Carvalho AA, Faustino J, Bota S, Ferreira ST. Unusual presentation in cow’s milk protein allergy. BMJ Case Rep. 2021; 14(7): 242080. doi: 10.1136/bcr-2021-242080.