
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Synergy between electrophysiologist and interventional cardiologist: The success of teamwork for cardiac resynchronization therapy in a complex coronary sinus case
Anna Sirignano1*; Rita Di Rosa1; Marco Petrassi1; Iginio Colaiori1; Roberto Zinicola1; Massimo Mastroluca1; Giuseppe Biondi-Zoccai2,3; Francesco Versaci1
1Division of Cardiology, Santa Maria Goretti Hospital, Latina, Italy.
2Department of Medical-Surgical Sciences and Biotechnologies, Sapienza University of Rome, Latina, Italy.
3Maria Cecilia Hospital, GVM Care & Research, Cotignola, Italy.
*Corresponding Author : Anna Sirignano
Division of Cardiology, Santa Maria Goretti Hospital, Latina, Italy.
Email: an.sirignano@gmail.com
Received : Apr 26, 2025
Accepted : May 19, 2025
Published : May 26, 2025
Archived : www.jcimcr.org
Copyright : © Sirignano A (2025).
Abstract
A complex Coronary Sinus (CS) anatomy can significantly hinder successful cannulation and Left Ventricular (LV) lead placement, potentially resulting in the failure of Cardiac Resynchronization Therapy (CRT). We report the case of a 67-year-old man referred for biventricular pacemaker implantation, in whom the procedure was technically challenging due to an unfavorable CS origin and marked tortuosity along its proximal course. Initial attempts at CS cannulation using conventional diagnostic and electrophysiology catheters proved unsuccessful, despite repeated guidewire manipulation and contrast-guided localization. Recognizing the anatomical complexity, a collaborative approach was adopted involving both the electrophysiology and interventional cardiology teams. This interdisciplinary effort facilitated the adoption of advanced tools beyond standard practice. In particular, a guide extension catheter provided enhanced backup support and distal reach, enabling sub-selective engagement of the posterior CS branch. Further, balloon-assisted tracking/anchoring using a non-compliant percutaneous transluminal coronary angioplasty balloon allowed successful advancement of the delivery system through the tortuous segment. Following these maneuvers, the quadripolar LV lead was successfully advanced and positioned with stable electrical parameters and no diaphragmatic stimulation. CRT system was implanted without further complications. Post-procedural electrocardiogram demonstrated QRS narrowing, and at follow-up, the patient exhibited marked clinical improvement. This case illustrates the importance of flexibility in technique and the value of cross-specialty collaboration in overcoming challenging venous anatomy.
Keywords: Balloon-assisted tracking; Cardiac resynchronization therapy; Coronary sinus abnormalities; Guide extension catheter; Left ventricular lead placement.
Citation: Sirignano A, Di Rosa R, Petrassi M, Colaiori I, Zinicola R, et al. Synergy between electrophysiologist and interventional cardiologist: The success of teamwork for cardiac resynchronization therapy in a complex coronary sinus case. J Clin Images Med Case Rep. 2025; 6(5): 3606.
Introduction
Cardiac Resynchronization Therapy (CRT) is a well-established therapeutic strategy for patients with symptomatic heart failure with reduced ejection fraction (HFrEF) and ventricular dyssynchrony, as endorsed by international guidelines and supported by robust clinical evidence. Through biventricular pacing, CRT can improve symptoms, enhance functional capacity, and reduce both morbidity and mortality [1,2]. However, 10% to 30% of patients fail to respond to CRT, with anatomical and technical challenges often underlying these suboptimal outcomes [3]. Successful implantation of the Left Ventricular (LV) lead-a cornerstone for CRT efficacy-requires a sequence of technically demanding steps, including Coronary Sinus (CS) localization and cannulation, selective engagement of a suitable venous branch, and stable LV lead placement. Each of these steps can be complicated by unfavorable CS anatomy, such as tortuosity, angulation, or anomalous branching patterns [4]. Standard delivery systems may be insufficient in such cases, necessitating the adoption of advanced techniques or devices. Several studies have explored variations in the coronary venous anatomy and proposed alternative strategies to facilitate LV lead placement in difficult CRT candidates. While some of these methods are derived from experiences in congenital heart disease or rare anatomical variants [5-8], their broader applicability remains limited due to the inherent variability of the CS anatomy in the general heart failure population [9,10]. In this context, we report a case of successful CRT implantation in a patient with highly complex CS anatomy, where close collaboration between the electrophysiology and interventional cardiology teams proved essential. This interdisciplinary approach enabled the use of adjunctive imaging and advanced device-based techniques to overcome procedural hurdles and achieve optimal left ventricular lead placement.
Case presentation
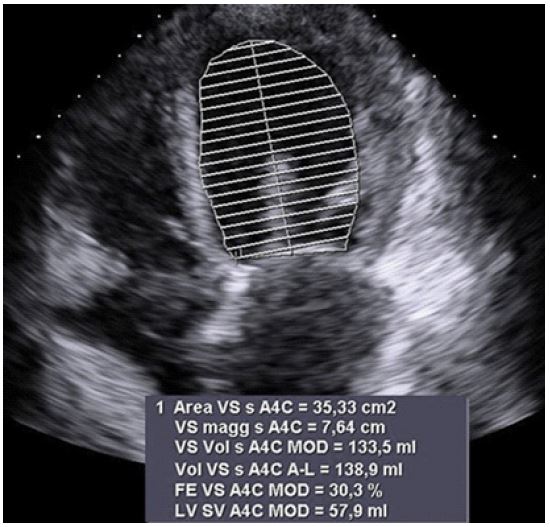
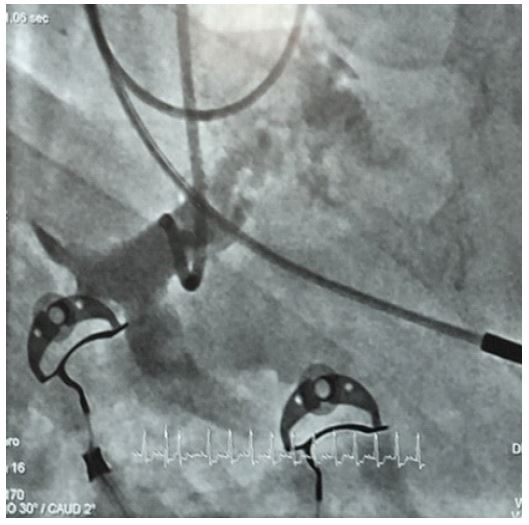
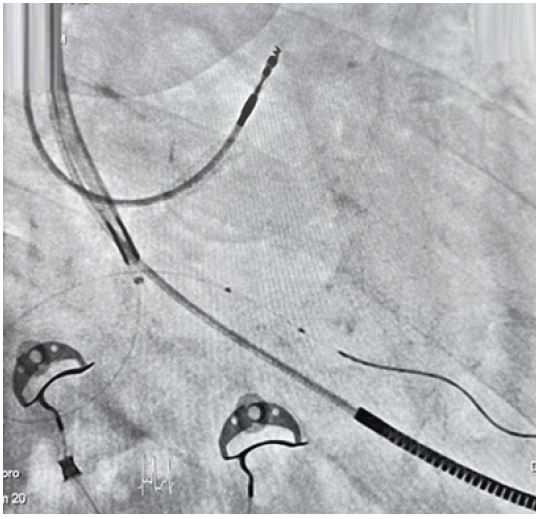
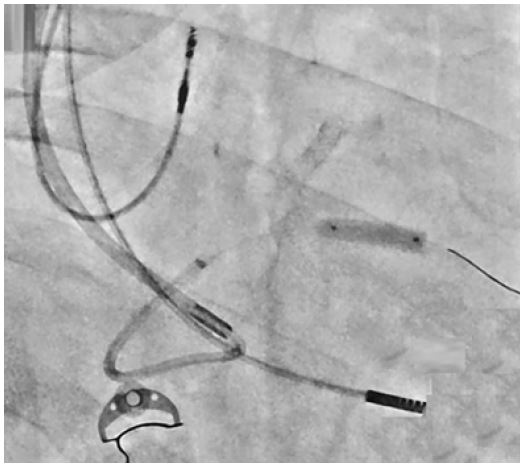
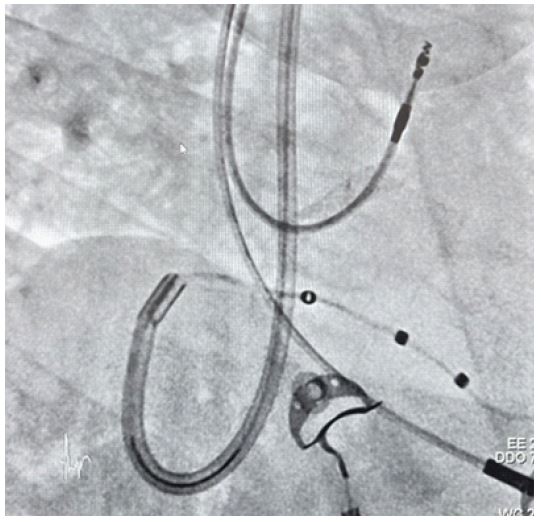
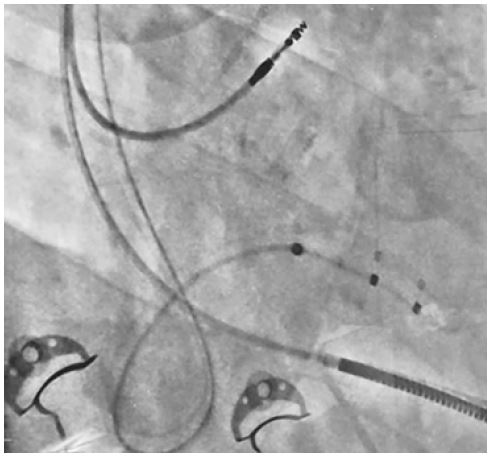
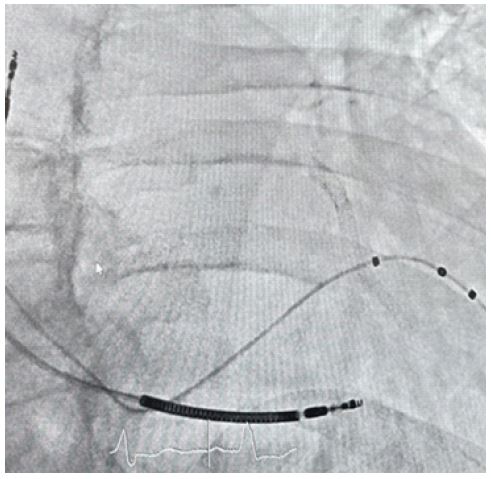
A 67-year-old man with a history of ischemic cardiomyopathy and no other significant comorbidities presented with New York Heart Association (NYHA) class III dyspnea despite being on optimized heart failure therapy. Electrocardiography (ECG) revealed a left bundle branch block (LBBB) with a QRS duration of 150 ms, while transthoracic echocardiography demonstrated a dilated left ventricle with an ejection fraction (EF) of 30% (Figure 1). The patient met thus criteria for CRT. The CRT procedure was conducted by two experienced electrophysiologists, with technical support provided by a field engineer from Abbott, Rome, Italy. The Right Ventricular (RV) and Right Atrial (RA) leads (Abbott Duarte 58 cm and Abbott Tendril STS 52 cm, respectively) were uneventfully placed via the left cephalic vein using conventional techniques. Subsequent access was obtained via the left subclavian vein, and a 9 F sheath was introduced to allow advancement of a standard delivery system for CS cannulation. Multiple attempts to cannulate the CS using a Josephson catheter and a deflectable diagnostic catheter (Abbott Livewire Deca polar) were however unsuccessful. An Implats Left 2 (AL2) diagnostic catheter (Medtronic, Santa Clara, CA, USA) was then positioned in the RA for support, and power injection of contrast identified a likely posterior wall coronary vein (Figure 2). However, repeated attempts to cannulate the CS using the AL2 catheter and a 0.014” workhorse guidewire were unsuccessful. The catheter was then exchanged again for the standard delivery system, through which the 0.014” guidewire was advanced and manipulated with care. This maneuver ultimately achieved successful CS cannulation, allowing the wire to track through the significantly tortuous proximal segment into a suitable posterior branch. Initial attempts to advance the CS delivery sheath over the guidewire were impeded by the vessel’s severe tortuosity. At this point, consultation with an interventional cardiologist was sought, enabled by the structural integration of adjacent electrophysiology and interventional suites within our hospital, facilitating real-time multidisciplinary collaboration. A decision was made to use a Guidiville II guide extension catheter (Boston Scientific, Milan, Italy) to provide coaxial support and improve push ability, owing to its robust proximal shaft and atraumatic soft distal tip (Figure 3). Thus, the Guidiville catheter was successfully advanced into the distal portion of the posterior branch (Figure 4). To overcome residual resistance, a semi-compliant percutaneous transluminal coronary angioplasty (PTCA) ballon (Emerge, 4.00x15 mm, Boston Scientific) was inflated up to 20 ATM to enable balloon-assisted tracking/anchoring of the delivery system across the tortuous segment (Figure 5). Following successful sheath advancement, the balloon and guidewire system were withdrawn. Subsequently, a quadripolar LV lead (Abbott Quartet, 86 cm) was smoothly advanced and deployed within the target vein (Figures 6,7,8), demonstrating excellent pacing and sensing thresholds without diaphragmatic stimulation. All leads were connected to a biventricular pacemaker generator (Abbott Quadra Assura MP), which was implanted in a subcutaneous pocket. The total skin-to-skin procedure time was 2 hours and 25 minutes. Post-procedural ECG demonstrated QRS narrowing, and at one-month follow-up, the patient reported significant symptomatic improvement, with NYHA class reduced from III to II.

Discussion/conclusion
Positioning the Left Ventricular (LV) lead remains the most technically challenging and prognostically significant step in Cardiac Resynchronization Therapy (CRT). Accurate placement is essential for achieving optimal electrical resynchronization and favorable clinical outcomes [7,11]. However, the complexity of the coronary venous anatomy-including variant ostial positions, sharply angulated or tortuous venous pathways, stenoses, and the presence of Thebesian valves-can significantly hinder LV lead delivery. These anatomical obstacles frequently account for CRT non-response, despite appropriate patient selection and device programming [6,12]. Thus, even in the era of advanced technologies, CRT implantation success remains highly anatomy-dependent. Traditional CRT implantation techniques may be insufficient in cases of complex CS morphology. In such settings, procedural failure can be avoided by incorporating non-conventional strategies and interventional tools borrowed from other fields, such as coronary interventions. Among these, the use of guide extension catheters like Guidiville II has shown promise in navigating tortuous anatomy by providing enhanced coaxial support and distal reach [10,13]. Balloon-assisted tracking, initially developed for percutaneous coronary interventions, can also play a pivotal role in facilitating sheath advancement [14]. These strategies, though not routinely employed in standard CRT practice, can be decisive in anatomically complex cases. The current case underscores the importance of multidisciplinary collaboration between electrophysiologists and interventional cardiologists in addressing such challenges. When standard delivery systems and techniques fail, the ability to seamlessly transition to advanced interventional maneuvers can markedly improve procedural outcomes [15]. In our institution, the proximity of electrophysiology and hemodynamics laboratories enables rapid, real-time collaboration. This structural and cultural integration allows for fluid teamwork and swift adaptation of interventional techniques when anatomical complexities arise. Such synergy ultimately benefits the patient by broadening the armamentarium available to the implanting team.
Importantly, this case also highlights the need for procedural flexibility and pre-emptive planning. Operators should be familiar with a range of bailout techniques and devices that can be employed when conventional strategies are not feasible. Rather than persisting with repeated unsuccessful attempts, early recrecognition of anatomic difficulty and timely escalation to hybrid solutions can reduce procedure time, minimize complications, and improve lead stability and performance. The presence of experienced operators and a well-organized environment for collaborative procedures is crucial to implementing these advanced techniques effectively. In this way, an individualized, anatomy-driven approach can replace the one-size-fits-all model traditionally used in CRT. Notably, this is the first case ever reporting on the use of Guidiville II for CRT, and the second ever showcasing the usefulness of balloon-assisted tracking in the same setting [16]. Ultimately, this case reinforces the concept that teamwork is not merely an adjunct to technical skill, but a central determinant of success in complex device therapy. When procedural complexity intersects with anatomical variability, interdisciplinary collaboration becomes essential. As CRT continues to evolve, embedding flexibility, innovation, and cooperation into clinical practice may help expand the boundaries of its effectiveness. This experience supports the broader integration of interventional expertise into electrophysiology workflows, particularly for anatomically challenging CRT candidates. Future studies may help standardize such hybrid approaches and define best practices for multidisciplinary CRT implantation.
Declarations
Disclosure: Giuseppe Biondi-Zoccai has consulted, lectured and/or served as advisory board member for Abiomed, Advanced Nanotherapies, Aleph, Amarin, AstraZeneca, Balmed, Cardionovum, Cepton, Crannmedical, Endocore Lab, Eukon, Guidotti, Innovheart, Meditrial, Menarini, Microport, Opsens Medical, Synthesa, Terumo, and Translumina, outside the present work. All other authors report no conflict of interest.
Acknowledgements: This manuscript was drafted with the assistance of artificial intelligence tools, such as ChatGPT 4 (OpenAI, San Francisco, CA, USA), Mage (Mage, New York, NY, USA), in keeping with established best practices (Biondi-Zoccali G, editor. ChatGPT for Medical Research. Torino: Edizioni Minerva Medica; 2024). The final content, including all conclusions and opinions, has been thoroughly revised, edited, and approved by the authors. The authors take full responsibility for the integrity and accuracy of the work and retain full credit for all intellectual contributions. Compliance with ethical standards and guidelines for the use of artificial intelligence in research has been ensured.
References
- McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, et al. Kathrine Skibelund A; ESC Scientific Document Group. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eury Heart J. 2021; 42(36): 3599-3726. doi: 10.1093/Earhart/ehab368.
- Abraham WT, Fisher WG, Smith AL, DeLario DB, Leon AR, et al. MIRACLE Study Group. Multicenter InSync Randomized Clinical Evaluation. Cardiac resynchronization in chronic heart failure. N Engl J Med. 2002; 346(24): 1845-53. doi: 10.1056/NEJMoa013168.
- Daubert C, Behar N, Martins RP, Mabo P, Leclercq C. Avoiding non-responders to cardiac resynchronization therapy: a practical guide. Eury Heart J. 2017; 38(19): 1463-1472. doi: 10.1093/Earhart/ehw270.
- Moss AJ, Hall WJ, Cannon DS, Klein H, Brown MW, et al. MADIT-CRT Trial Investigators. Cardiac-resynchronization therapy for the prevention of heart-failure events. N Engl J Med. 2009;361(14): 1329-38. Doi: 10.1056/NEJMoa0906431.
- Akhtar Z, Sohal M, Kontogiannis C, Harding I, Zuberi Z, et al. Anatomical variations in coronary venous drainage: Challenges and solutions in delivering cardiac resynchronization therapy. J Cardiovasc Electrophysiology. 2022; 33(6): 1262-1271. Doi: 10.1111/jce.15524.
- Barwa P, Kaur N, Sihag BK, Nagano SH. Long-term outcome of variety of techniques used to stabilize left ventricular lead in difficult coronary sinus anatomy-A single center experience. Indian Heart J. 2024; 76(5): 327-332. Doi: 10.1016/j.ihj.2024.10.001.
- Alves Silva LA, de Souza Meira EB, Cofimvaba J, Pimenta JA. Coronary Sinus Phlebography in Cardiac Resynchronization Therapy Patients: Identifying and Solving Demanding Cases. J Innov Card Rhythm Manag. 2020; 11(7): 4161-4170. Doi: 10.19102/icrm.2020.110703.
- Johansen JB, Nielsen JC, Kristensen J, Sandgaard NC. Troubleshooting the difficult left ventricular lead placement in cardiac resynchronization therapy: current status and future perspectives. Expert Rev Med Devices. 2022; 19(4): 341-352. Doi: 10.1080/17434440.2022.2075728.
- Manchanda M, McLeod CJ, Killum A, Asvathama SJ. Cardiac resynchronization therapy for patients with congenital heart disease: technical challenges. J Intern Card Electrophysiology. 2013; 36(1): 71-9. Doi: 10.1007/s10840-012-9726-x.
- Worley SJ, Gohn DC, Pulliam RW. Interventional approach to CRT in a patient with drainage of the superior vena cava into the coronary sinus. Pacing Clin Electrophysiology. 2008; 31(4): 506-8. Doi: 10.1111/j.1540-8159.2008.01023. x.
- Morgan JM, Delgado V. Lead positioning for cardiac resynchronization therapy: techniques and priorities. Euro pace. 2009; 11(5): 22-8. Doi: 10.1093/euro pace/eup306.
- Kim CH, Cho YD, Kang HS, Kim JE, Jung SC, et al. Anomalous External Carotid Artery-Internal Carotid Artery Anastomosis in Two Patients with Proximal Internal Carotid Arterial Remnants. Korean J Radial. 2015; 16(4): 914-8. Doi: 10.3348/kjr.2015.16.4.914.
- Nørregaard Jakobsen F, Sandgaard NCF, Olsen T, Brandes A, Djurhuus MS, et al. Is interventional technique better than the traditional over-the-wire method for left ventricular lead implantation in cardiac resynchronization therapy? Heart Rhythm O2. 2024; 5(5): 281-288. doi: 10.1016/j.hroo.2024.04.001.
- Ma J, Hou L, Qian J, Ge L, Zhang F, et al. The safety and feasibility of Godzilla catheter in complex coronary interventions and an observational study. Medicine (Baltimore). 2017; 96(40): 8172. Doi: 10.1097/MD.0000000000008172.
- Johansen JB, Nielsen JC, Kristensen J, Sandgaard NC. Troubleshooting the difficult left ventricular lead placement in cardiac resynchronization therapy: current status and future perspectives. Expert Rev Med Devices. 2022; 19(4): 341-352. doi: 10.1080/17434440.2022.2075728.
- Samy M, Hamdy RM. A case report of balloon-assisted tracking to overcome coronary sinus competent valve: A novel technique in left ventricular lead implantation. Eur Heart J Case Rep. 2022; 6(2): 056. doi: 10.1093/ehjcr/ytac056.