
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Giant subcapsular hepatic biloma from gallbladder perforation due to blunt abdominal trauma: An inn-usual case report
Alejandro Gónzález-Muñoz1; Daniela Ayala2*; Valentina Amador2; Sebastián Diaz Macias2; Nestor Pedraza3; Juan Carlos Sabogal Olarte1,2
1School of Medicine, Universidad del Rosario, Bogotá, Colombia.
2Hepatobiliary and Pancreatic Surgery Department, Hospital Universitario Mayor, Méderi, Bogotá, Colombia.
3Transplant Department, Hospital Universitario Mayor, Méderi, Bogotá, Colombia.
*Corresponding Author : Daniela Ayala Olaya
Hepatobiliary and Pancreatic Surgery Department, Hospital Universitario Mayor, Méderi, Bogotá, Colombia.
Tel: +57-3134132853;
Email: daoti77@gmail.com
Received : Apr 29, 2025
Accepted : May 20, 2025
Published : May 27, 2025
Archived : www.jcimcr.org
Copyright : © Olaya DA (2025).
Abstract
Introduction: Biliomas are usually collections contained by lesions of intra- or extrahepatic bile ducts and are much less frequently associated with gallbladder perforation, generally related to blunt trauma.
Case report: We present the case of a 53-year-old man with a history of kidney transplantation, who sustained blunt abdominal trauma. Eight days post-trauma, a cystic lesion occupying the patient’s right hemiabdomen was documented, leading to clinical deterioration and an urgent indication for surgical management. Intraoperatively, a bilioma approximately 40 x 30 cm in size was identified, channeling a gallbladder perforation at the fundus, requiring de-roofing of the bilioma and open cholecystectomy.
Conclusions: Although gallbladder trauma is rare, it can present with contained cystic lesions. Rapid diagnosis and differentiation from a hematoma lead to appropriate management and good postoperative outcomes.
Keywords: Bilioma; Abdominal blunt trauma; Gallbladder trauma.
Citation: Gónzález-Muñoz A, Ayala D, Amador V, Macias SD, Pedraza N et.al. Giant subcapsular hepatic biloma from gallbladder perforation due to blunt abdominal trauma: An inn-usual case report. J Clin Images Med Case Rep. 2025; 6(5): 3607.
Introduction
Biliomas are collections of bile usually associated with disruption due to injury of the intra- or extrahepatic bile ducts, covered by hepatic parenchyma, capsule, or other structures adjacent to the site of bile duct disruption [1,2]. The association of biliomas with gallbladder injury is very rare, with few reports in the literature [1], as gallbladder injury in blunt abdominal trauma is uncommon due to its subhepatic location [3].
The most frequently identified clinical sign of gallbladder injury is abdominal pain that increases in intensity, indicating the possibility of perforation and progression to biliary peritonitis [3,4]. However, the association of a bilioma with an independent gallbladder injury may present as a sensation of a mass, abdominal distension, mild pain, nausea, or vomiting, related to the involvement of adjacent structures [1]. We report the case of a 53-year-old patient who, after a blunt abdominal trauma, presented late with a giant bilioma that required surgical management due to peritoneal irritation. This was identified as being associated with a perforation of the gallbladder fundus extending to Glisson’s capsule without adjacent liver injury.
Case report
A 53-year-old male patient with a history of a living-donor kidney transplant in 2012, followed up for graft dysfunction managed with mycophenolate mofetil and tacrolimus. In April 2024, the patient presented to the emergency department due to polytrauma secondary to a fall from a motorized vehicle (electric scooter) at approximately 15 km/h. Initial consultation documented no significant abnormalities on physical examination or ancillary tests.
The patient reconsulted the emergency department due to persistent pain, 8 days post-trauma, presenting with abdominal distension without signs of peritoneal irritation and admission labs showing hemoglobin at 10.5 mg/dl without additional abnormal findings. Considering the described clinical scenario, a contrast-enhanced abdominal CT scan was indicated, documenting a subcapsular lesion with internal content, likely corresponding to a subcapsular hematoma with dimensions of 298 x 103 x 228 millimeters, in contact with hepatic segments 2 and 4, extending to the right iliac fossa and pelvic cavity (Figure 1). Suspecting a hepatic hematoma, given the described history, follow-up was decided in conjunction with the transplant surgery service. During initial follow-up, pain was adequately managed, but laboratory controls showed a progressive decrease in hemoglobin to 7.4 mg/dl, concluding a hepatic hematoma secondary to blunt abdominal trauma.
A complementary abdominal angiography was performed, showing no evidence of contrast medium extravasation in the described lesion, no free fluid in the abdominal cavity, nor an increase in its dimensions. Despite this, during in-hospital follow-up, clinical deterioration was documented due to increased abdominal pain and signs suggestive of peritoneal irritation. The case was discussed with the transplant surgery service, recognizing the possibility of transfusion sensitization due to immunosuppression. Given the clinical deterioration and persistent anemia, transfusion of 2 units of red blood cells was indicated, and surgical management via open approach was decided.
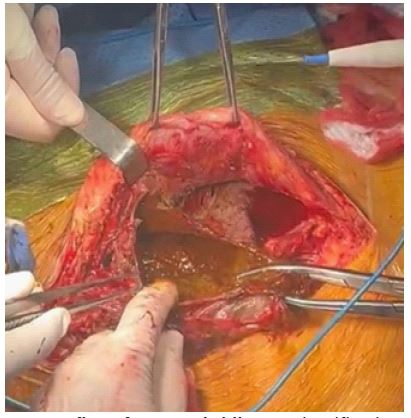
A supra- and infraumbilical exploratory laparotomy was performed, immediately identifying upon opening the posterior rectus sheath a large lesion occupying the entire right hemiabdomen, with thick walls (Figure 2). Initial puncture returned bile, indicating the presence of a traumatic biloma. De-roofing of the biloma was initiated (Figure 3), demonstrating bile conduction through a fistulous orifice from a gallbladder perforation at the fundus directed to the cystic lesion, requiring completion of cyst wall resection and open cholecystectomy, with no documented bleeding or other complications. During postoperative surveillance, a postoperative ileus was documented, with progressive improvement. The patient is currently under a two-month postoperative follow-up with adequate clinical evolution
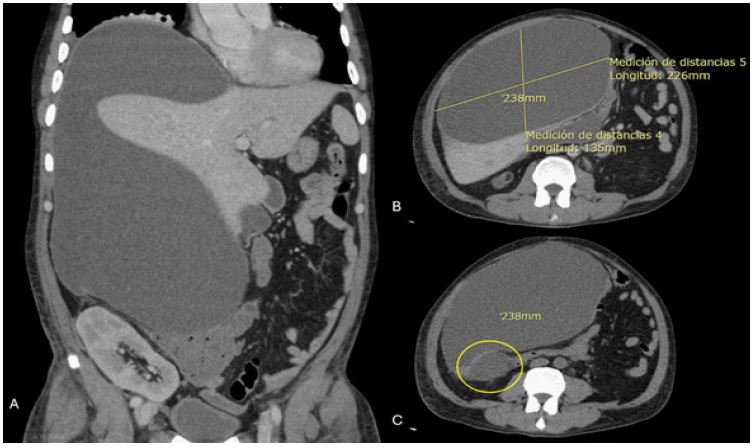
(A) Coronal slice showing hepatic lesion with cystic characteristics, extending to the right iliac fossa and pelvis, with extrinsic compression of the renal graft and the liver.
(B) Transverse slice visualizing the lesion with cystic characteristics and a diameter of 238 mm.
(C) Gallbladder in contact with the described cystic lesion.

Discussion
The literature reports an approximately 2-3% rate of independent gallbladder injury in blunt abdominal trauma [1,3]. Its association with contained collections is very rare, more frequently linked to postoperative complications of cholecystectomy (approximately 7%) and less commonly to bile duct instrumentation and neoplastic lesions [5]. In the context of trauma, as presented in our case, the appearance of a bilioma and its progression occurs within 48 hours post-injury, with a progressive course [2,5,6].
The symptoms usually associated with the presence of biliomas include abdominal pain. Given the coexistence of the bilioma, additional symptoms may appear depending on its size, though jaundice is rarely seen [7]. It may also present without associated symptoms [5]. Elevated transaminase levels have been documented; however, 40% of patients with biliomas may not show any alteration in liver function tests [5]. Biliomas are characterized as cystic images in relation to the liver in various diagnostic studies such as ultrasound, CT scan, and MRI. Independently characterizing gallbladder perforation using diagnostic imaging like CT scan is complex [3,5]. On CT scan, the density of bilioma content can be characterized as less than 20 Hounsfield units (HU), compared to hemorrhagic content which is usually greater than 30 HU [5].
Initial therapeutic tools proposed include percutaneous aspiration or stent placement via endoscopic retrograde cholangiography [6]. However, in patients showing signs of peritoneal irritation, surgical management is indicated. This involves deroofing the cystic cavity and managing the biliary fistula if possible. In cases where the bilioma originates from gallbladder perforation, a cholecystectomy is performed [6,8,9].
The clinical course of a bilioma without perforation into the cavity is usually benign, with a high response rate to percutaneous and endoscopic management. However, effective diagnosis is crucial considering the potential for sepsis, hemorrhage, and peritonitis, which significantly increase patient morbidity [5,8].
Conclusion
Isolated gallbladder injury in blunt abdominal trauma is rare, and even rarer is the clinical presentation of a bilioma associated with gallbladder perforation. Rapid diagnosis allows for endoscopic and percutaneous management with a very good response. In the presented case, considering the course of peritoneal irritation, open surgery was performed with favorable clinical outcomes, including controlled management of the bilioma and cholecystectomy, resulting in a favorable postoperative recovery.
Declarations
Informed consent: Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available from the Editor-in-Chief of this journal upon request.
Ethical approval: Ethical approval was provided by the authors’ institution.
Funding: The authors declare no financial conflicts.
Declaration of conflict of interest: The authors declare no conflict of interest.
No use of artificial intelligence-assisted technologies was made.
Authors contribution according to COPE guidelines:
- Design, acquisition and conception of the study: Valentina Amador, Sebastián Díaz
- Data analysis and interpretation: Daniela Ayala, Alejandro Gonzalez
- Manuscript drafting: Daniela Ayala, Valentina Amador, Sebastian Diaz, Alejandro Gonzalez
- Critical revision: Juan Carlos Sabogal
References
- Ferrusquía-Acosta JA, Álvarez-Navascués C, Rodríguez-García M. Giant biloma as a result of a blunt abdominal trauma: A case report. Revista espanola de enfermedades digestivas. Spain; 2015; 107: 768-9.
- Guzmán Calderón E, Salazar Ventura S, Monge Salgado E. Sub-hepatic bilioma: report of a case and review of literature. Rev Gastroenterol del Peru organo Of la Soc Gastroenterol del Peru. 2008; 28(3): 282–5.
- Testini V, Tupputi U, Rutigliano C, Guerra FS, Mannatrizio D, Bellitti R, et al. A rare case of isolated gallbladder rupture following blunt abdominal trauma. Acta Biomed. 2023; 94(S1): e2023207.
- Al-Hassani A, Jabbour G, ElLabib M, Kanbar A, El-Menyar A, Al-Thani H. Delayed bile leak in a patient with grade IV blunt liver trauma: A case report and review of the literature. Int J Surg Case Rep. 2015; 14: 156–9.
- Copelan A, Bahoura L, Tardy F, Kirsch M, Sokhandon F, Kapoor B. Etiology, Diagnosis, and Management of Bilomas: A Current Update. Tech Vasc Interv Radiol. 2015; 18(4): 236–43.
- Ragavan M, Duraiprabhu A, Madan R, Murali K, Francis G, Subramanian M. Posttraumatic Intrahepatic Bilioma. Indian J Surg. 2015; 77(Suppl 3): 1399–400.
- Choudhary N, Duseja A, Kalra N, Chawla Y. Hepatobiliary and pancreatic: intrahepatic biloma after blunt abdominal trauma. J Gastroenterol Hepatol. 2011; 26(8): 1342.
- Limani N, Misimi S, Nikolovski A. Large biloma as the initial presentation of gallbladder perforation: a case report and literature review. Journal of surgical case reports. England. 2023; 2020: rjad669.
- Brillantino A, Iacobellis F, Festa P, Mottola A, Acampora C, Corvino F, et al. Non-Operative Management of Blunt Liver Trauma: Safety, Efficacy and Complications of a Standardized Treatment Protocol. Bull Emerg trauma. 2019; 7(1): 49–54.