
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 6
Rare unusual case of spontaneous OHSS in a young unmarried girl
Krishna Pratap Singh1*; Saurabh K Varma2; K Uday Bhanu3
1Department of Radiodiagnosis and Imaging, Command Hospital (Eastern Command) Kolkata, India.
2Resident Radiology, Command Hospital (Eastern Command) Kolkata, India.
3HOD Radiology, Command Hospital (Eastern Command) Kolkata, India.
*Corresponding Author : Krishna Pratap Singh
Department of Radiodiagnosis and Imaging, Command Hospital (Eastern Command) Kolkata, India.
Email: drkpss009@gmail.com
Received : Apr 30, 2025
Accepted : May 21, 2025
Published : May 28, 2025
Archived : www.jcimcr.org
Copyright : © Singh KP (2025).
Citation: Singh KP, Varma SK, Bhanu KU. Rare unusual case of spontaneous OHSS in a young unmarried girl. J Clin Images Med Case Rep. 2025; 6(5): 3609.
Description
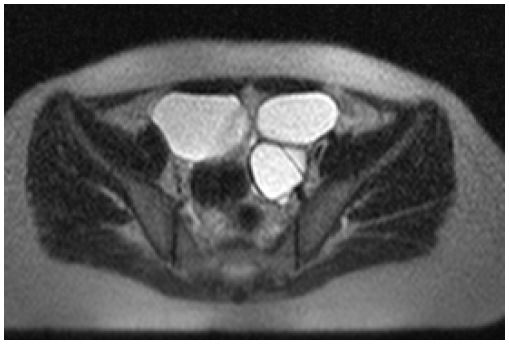
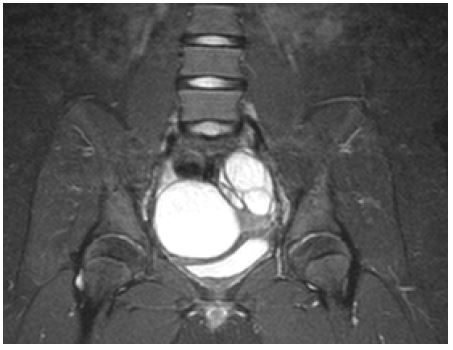
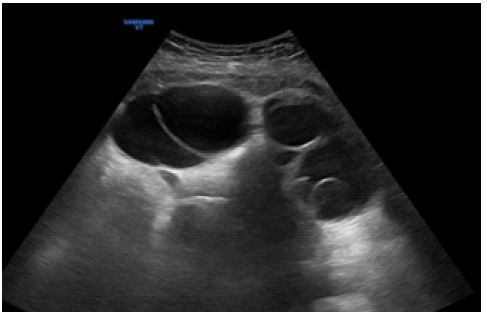
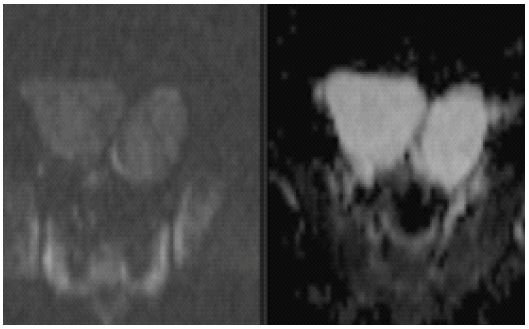
A 12-year-old female child attained menarche at 10 years of age with and presented with complaints of lower abdominal pain and irregular menses. The child was diagnosed with hypothyroidism at the age of 8 years and was put on thyroxine and is currently on 75 mcg thyroxine for the past 1 year with normal thyroid parameters. The child while being evaluated for pain abdoment and irregular periods underwent ultrasonography and MRI examination of the abdomen and pelvis which showed bilateral bulky adnexal with bilateral multiloculate T2/STIR hyperintense cystic lesions measuring ~6 x 7 x 8 cm on right side and ~7 x 4 x 9 cm on the left side (AP x TR xCC) [1]. These cysts do not restriction of diffucion on DWI or blooming on GRE ruling out presence of solid tissue or bleed. Uterus is normal with endometrial thickness of 8 mm. Urine pregnancy test was negative. The patients CA-125, LDH, AMH, progesterone, estrogen, testosterone and prolaction levels were all normal. Patients hCG, LH, FSH values were also within normal limits. Viral markers were also normal [2].
Discussion
Ovarian hyperstimulation syndrome (OHSS) is a severe disease with significant morbidity and mortality associated with it. It is usually caused by hyperstimulation of ovaries secondary to controlled pharmacological induction of ovaries for patients undergoing infertility treatment. Rarely it can occur in pregnancy or due to genetic component. Few associations are also seen with early pubertal development and primary hypothyroidism (Van Grumbach syndrome) [3,4]. Though the exact cause is not known but it occurs due to complex interplay of hormones at multiple levels and altered hormonal regulation through feedback loops. It is proposed that hypothyroidism caused increased TSH which in fact can stimulate FSH receptors. Similar stimulation is also anticipated at pituitary level causing increased TRH production stimulating GnRH receptor leading to ovarian enlargement. Usually the ovarian enlargement resolves with thyroid hormone replacement but in this case the ovarian hyperstimulation continued thereby suggesting a missing link in hormonal regulation. Extensive work up showed normal levels of hormones thereby further puzzling our pediatric and endocrine team. This is the first case to the best of our knowledge ever reported in literature in a young unmarried girl without pregnancy.
Declarations
Conflicts of interest: Nil.
Informed consent: Informed consent taken from both the parents prior to submission for publication.
Funding: No funding received for this publication. The authors have no relevant financial or non financial interests to disclose.
References
- Nastri C, Teixeira D, Moroni R, Leitão V, Martins W. Ovarian Hyperstimulation Syndrome: Pathophysiology, Staging, Prediction and Prevention. Ultrasound Obstet Gynecol. 2015; 45(4): 377-93. doi:10.1002/uog.14684 - Pubmed
- Lovgren T, Tomich P, Smith C, Berg T, Maclin V. Spontaneous Severe Ovarian Hyperstimulation Syndrome in Successive Pregnancies with Successful Outcomes. Obstet Gynecol. 2009; 113(2 Pt 2): 493-5. doi:10.1097/AOG.0b013e318184182b - Pubmed
- Lovgren T, Tomich P, Smith C, Berg T, Maclin V. Spontaneous Severe Ovarian Hyperstimulation Syndrome in Successive Pregnancies with Successful Outcomes. Obstet Gynecol. 2009; 113(2 Pt 2): 493-5. doi:10.1097/AOG.0b013e318184182b - Pubmed.
- Sultan A, Velaga M, Fleet M, Cheetham T. Cullen’s Sign and Massive Ovarian Enlargement Secondary to Primary Hypothyroidism in a Patient with a Normal FSH Receptor. Arch Dis Child. 2006; 91(6): 509-10. doi:10.1136/adc.2005.088443 – Pubmed