
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 6
Digestive foreign bodies in children in the pediatric emergency department of the Mohammed VI university hospital, Morocco
Mghazli H*; Elmassi M; Assem O; El Moussaoui S; Lahmini W; Bourrous M
Faculty of Medicine and Pharmacy, Mohammed VI University Hospital, Morocco.
*Corresponding Author : Hajar Mghazli
Faculty of Medicine and Pharmacy, Mohammed VI University Hospital, Morocco.
Email: drmghazlihajar@gmail.com
Received : Apr 27, 2025
Accepted : May 22, 2025
Published : May 29, 2025
Archived : www.jcimcr.org
Copyright : © Mghazli H (2025).
Abstract
Introduction: Foreign body (FB) ingestion is a common accident in children, especially during early childhood.
Objectives: To highlight the epidemiological and evolutionary aspects of foreign body ingestion in children.
Patients and methods: This is a retrospective study of a series of 289 cases collected at the Pediatric Emergency Department of the Mohammed VI University Hospital in Marrakech, over a period of 5 years (October 2014-December 2019).
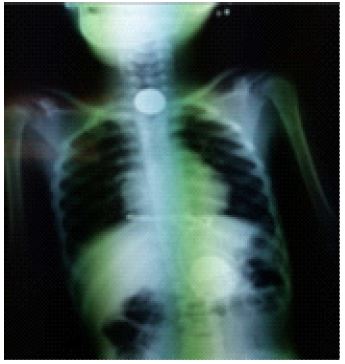
Results: The study involved 131 girls and 158 boys with an average age at diagnosis of 4 years (6 months-15 years), the most frequent age group was between two and three years (22%). The average consultation time was relatively long (19 hours and 10 minutes), 76% of our patients were admitted within the first 24 hours. Hypersalivation and dysphagia were the most frequent symptoms, described in 60.55% and 52.94% of cases respectively. The general examination was normal in 21% of patients who were completely asymptomatic at admission. Foreign bodies were radiopaque in 96% of cases. Extraction and exploration of the digestive tract by pharyngoscopy or esophagogastroduodenal fibroscopy were performed within 24 hours in 90% of cases with spontaneous elimination in 7% of cases which took place between 2 and 6 days,whereas surgery was only necessary in one case (1%) after failure of pharyngoscopy. The majority of foreign bodies were extracted from the proximal third of the esophagus (87.54%). The evolution was marked by the absence of occurrence of complications in the majority of cases (84.42%), without having noted any case of death.
Conclusion: Foreign body ingestion is a serious problem in early childhood. Multidisciplinary management is recommended due to its clinical polymorphism, which makes it a diagnostic challenge. Prevention requires parental education to ensure a significant reduction in morbidity and mortality from this condition.
Citation: Mghazli H, Elmassi M, Assem O, El Moussaoui S, Lahmini W, et al. Digestive foreign bodies in children in the pediatric emergency department of the Mohammed VI university hospital, Morocco. J Clin Images Med Case Rep. 2025; 6(5): 3611.
Introduction
Foreign body ingestion is a common reason for consultation in pediatric emergency rooms. It is among the most frequent domestic accidents that any doctor can face and may be due to voluntary or involuntary swallowing of a foreign body, requiring urgent treatment which varies depending on the nature and location of the foreign body [1,2]. The incidence is often underestimated, with spontaneous evacuation through the digestive tract without any clinical manifestation. In other cases, the symptomatology is very variable depending on the nature, type, size and location of the foreign body, which can lead to diagnostic difficulties. The evolution depends on the migration and then the spontaneous elimination or entrapment of the foreign body. The ingestion of foreign bodies occurs in 80% of cases in infants and young children, they most often occur between the ages of 6 months and 3 years [5,6]. This percentage is explained by the tendency of young children to explore their environment by placing objects in their mouths as well as by the organic immaturity of the hypopharyngeal region. Multidisciplinary collaboration (involving the general practitioner, pediatrician, ENT surgeon, pediatric surgeon, anesthesiologist, gastroenterologist and radiologist) is necessary for early and adequate management due to the complications caused [4].
Patients and methods
This was a retrospective study and description of the children admitted for ingestion of foreign body, collected at the service of EMERGENCIES Pediatricians at the Mohammed VI University Hospital in Marrakech over a period of 5 years between October 2014 and October 2019. All children under 15 years of age admitted for foreign body ingestion were included. Incomplete clinical records, foreign body inhalations, and children with caustic or peptic esophageal strictures were excluded from the study. Data were collected from medical records in the Pediatric Emergency Department using a pre-established operating sheet. This study consisted of analyzing epidemiological, clinical, paraclinical, therapeutic modalities, evolution, and complications of the patients included in the study.
Results
There were 289 cases of foreign body ingestion in children under 15 years of age over a period of 5 years. The average age was approximately 4 years, with extremes ranging from 6 months to 15 years. The age group [2-3 years] represented the predominant group. We also observed a predominance in preschool children (under 5 years) with a number of 204 cases (71%); a male predominance with 158 cases and a sex ratio of 1.2. Most of the children were from rural areas (56%), including a male predominance both in urban areas with 86 boys (53%) and in rural areas 72 boys (56%). In our study, the majority of cases came from the Marrakech Safi region (85%). In the medical history, 3 patients (1%) had a foreign body ingestion (coin), 4 children (2%) had a surgical history (3 cases of tonsillectomies, 1 case with a pacemaker (Trisomy 21)) and the rest of the children had no particular pathological history (97%). More than three-quarters (76%) of patients consulted within the first 24 hours. The time between foreign body ingestion and consultation varied from 30 minutes to 30 days, with a mean time of 19 hours and 10 minutes. The majority of foreign body ingesingestion accidents occurred during play (96%) compared to 4% accidentally during meals. The nature of the foreign bodies was classified into 3 groups: metallic (276 children: 95%), organic (11 children: 4%) and plastic (2 children: 1%). The majority of foreign bodies were of a soft nature, with a clear predominance of coins found in 240 cases (83%). The clinical picture on admission was extremely variable. With (21.1%) cases completely asymptomatic. In symptomatic patients, the main symptoms were hypersalivation and dysphagia, described in 60.55% and 52.94% of cases respectively.
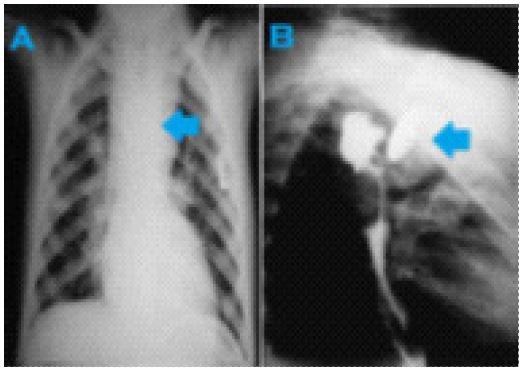
Furthermore, the clinical picture was alarming in one patient upon admission: this was a child admitted in an altered general condition, with a picture of digestive hemorrhage consisting of hematemesis and melena with obvious cutaneous and mucosal pallor. In 6 children, penetration syndrome (cough, cyanosis, suffocation) was the reason for the parents to consult. Food refusal was the mode of revelation in a 1-year-old infant following the ingestion of a coin 12 hours earlier. Fever was found in 6 of our patients (2.07%), with a temperature taken in the emergency room greater than or equal to 38°C. Respiratory signs (dyspnea, cough) were present in 6.22% of patients in association with digestive signs. Standard radiography (thoracic and thoracoabdominal radiography) was performed in all our patients, it allowed to objectify the radiopaque foreign body in 96% of cases. The combination of thoracic and thoracoabdominal radiography was performed in 58% of patients in our series to confirm the diagnosis and guide the localization. Furthermore, it did not objectify any complications. The most frequent location on the initial standard radiography was at the level of the upper third of the esophagus (92%). Abdominal ultrasound was performed and was normal in a 4-year-old girl admitted for ingestion of a coin for 10 days with notion of abdominal pain.Chest CT scanwas carried out in 2 patients: in the first case showed at the height of D2 a metallic foreign body (piece of metallic toy) with esophageal projection generating an artifact which prevents determining the exact location of the latter and In the second case showed the presence of a well-defined oval metallic foreign body of 5 cm × 2 cm (button cell) in the intra-esophageal at the junction of the upper and middle esophagus responsible for compression with repression of the trachea forward but with preservation of its permeability without evidence of pneumothorax. Upon admission, the patients’ general condition and vital signs were assessed, with a search for signs of severity and complications, followed by a conditioning exercise based on their condition and a physical examination. All patients were kept fasting with glucose and electrolyte infusions while awaiting treatment. The average time between admission and extraction was 22 hours and 30 minutes, with 90% of extractions performed within the first 24 hours after admission. Spontaneous elimination without intervention was noted in 21 patients (7%). The time to spontaneous elimination with detection of the foreign body in the stool was between 2 and 6 days. Pharyngoscopy, which has diagnostic and therapeutic purposes, allows to assess the state of the esophageal mucosa and the search for complications (ulceration, perforation, etc.) was performed in 273 patients under sedation (90%), including in 12 patients with extraction of the radiolucent foreign body and In 13 of our patients, pharyngoscopy did not result in the extraction of the foreign body following the progression of the latter in the digestive tract compared to its initial location on the admission radiograph. In the 4 cases where FOGD was performed, the extraction of 3 foreign bodies was without problem. In only one case, the extraction failed and the patient was put under surveillance with spontaneous elimination of the foreign body. Extraction using a Foley catheter was performed in 3 patients initially in good general condition and without complications, with a foreign body located in the upper third of the esophagus and a priori extirpable. Surgery was only necessary in one child after failure of extraction by pharyngoscopy, following the careless ingestion of an esophageal foreign body (button battery), complicatedesophageal stenosis. The patient’s postoperative course was normal without any notable complications. In our series, 22 patients (7%) were placed under clinical-radiological surveillance pendingexpulsionspontaneous.
All our patients were put on an absolute diet with glucose serum and electrolyte infusion while awaiting the therapeutic approach with monitoring of the general condition and physical and functional signs.
This treatment was associated with:
• Antibiotic treatment based on amoxicillin-clavulanic acid 100 mg/kg/day in 3 doses maintained for 7 to 10 days post-endoscopy: 58%
• Oral corticosteroid therapy for 5 days post-endoscopy: 60%
• Analgesic treatment (Paracetamol 60 mg/kg/day): 51%
• Temporary dietary restriction with postoperative placement of a nasogastric tube in patients with esophageal mucosal lesions: 16%
• Treatment with antisecretory drugs (PPIs) in patients with minimal lesions of the esophageal mucosa post-endoscopy: 3%
The average length of hospital stay was 1 day and 13 hours. The majority of our patients (84%) were hospitalized for less than 2 days. In our series, 15.57% of patients presented with minimal to moderate complications on endoscopic exploration, including superficial erosions of the esophageal or oral mucosa without bleeding on endoscopic examination in 40 patients (13.84%) and pressure necrosis at the level of the esophageal mucosa (with necrosectomy during extraction), an esophagotracheal fistula, ulceration and minimal bleeding following a neglected button battery requiring surgical intervention, episodes of large hematemesis associated with melena on admission, and requiring transfusion of packed red blood cells in 4 patients (1.41%). In a single case, an iatrogenic esophageal perforation occurred following an attempt at fiberscopic extraction of the foreign body (extraction failure) with apneumomediastinumon the control chest X-ray taken after the extraction attempt. The evolution was favorable in the majority ofour patients (84.42%) without any complications. No cases of death were reported in our series.
Discussion
Foreign body ingestion is a more common accident in children than in adults. According to the Susy Safe Project, accidental ingestion of an EC most often occurs before the age of 3 years, with a peak incidence between the ages of 6 months and 3 years [3,7,8]. In our series, the average age was 4 years, this result is similar to the study of Lakhdar-Idrissi in Fez [9]. The predominance in the male sex, with a sex ratio of 1.2 while in the Sidibé study in 2019, the male sex (40%) with a sex ratio of 1.2 [14] and in that of Fujisawa in 2020 the male sex (55.5%) with a sex ratio of 1.24 [10]. The male predominance observed in the majority of series finds no satisfactory hypothesis, and can be partly explained by the impulsive and adventurous character of young boys and the nature of their games [9]. “The Annual Report of the American Association of Poison Control Centers” reports 1,810,030 incidents of foreign body ingestion in a year, of which more than 90% are accidental [15], most often at playtime, and involve common objects found in the home environment such as coins, toy pieces, jewelry, magnets, and batteries [16]. Because children who have ingested a foreign body are often asymptomatic, the true incidence probably remains higher [8]. In our series, the time between foreign body ingestion and admission to the pediatric emergency department ranged from 30 minutes to 30 days with a mean time of 19 hours and 10 minutes. In the series extending between 2010 and 2013 (published in 2017) at the Pediatric Emergency Department at the Cruces University Hospital in Bilbao (Spain), the time between foreign body ingestion and admission to the Pediatric Emergency Department was between 15 minutes and 30 days [17]. These data are consistent with those described in our study. However, according to the study by Cevik et al: 93% of patients consulted during the first 24 hours after the incident [18]. The same observation is reported in the series by Chun Woo et al: carried out between 1999 and 2012 (published in 2016) in South Korea, with 96.5% of consultations during the first 24 hours following the incident [19]. In our series, only 76% of consultations took place during the first 24 hours after the incident, this can be explained by the geographical origin of our patients, sometimes making access to care difficult. Remember that ingestion without witness leads to late consultation, especially in patients under two years old, which can lead to serious complications, including death [18,22]. Symptoms of foreign body ingestion vary greatly and depend largely on the size and shape of the object, its location, and the length of time it was retained [23]. Presentation of ingestion can range from asymptomatic to respiratory distress or acute abdomen. Up to 50% of children with known foreign body ingestion are asymptomatic [16]. It is estimated that 40% of foreign body ingestions in children go unnoticed, and in many cases the child never develops symptoms [24]. Since many foreign body ingestions by children are unwitnessed [22], the possibility that nonspecific symptoms are caused by the ingestion of foreign bodies should always be considered [25]. Naidoo and Reddi reported a case of a 3-year-old child who presented with dysphagia to solids for two months with cough, anorexia, and weight loss. Chest radiography revealed a coin-shaped foreign body in the upper mediastinum, outside the esophageal lumen on the esophagogram [27].
In our series, hypersalivation was the main symptom, present in 60.55% of patients, followed by dysphagia in 52.94% of cases. According to a study conducted in India by Mahajan and Prashanth, published in 2019 [28], throat discomfort was observed in 85% of patients, followed by dysphagia in 70% of cases. According to Delport et al, only 10% of patients were symptomatic upon arrival at the hospital. Delport et al. also reported that hypersalivation was the most common presentation of EC ingestion upon arrival at the hospital (43%), followed by dysphagia (21%) in symptomatic children [21]. In our series, penetration syndrome was reported by parents in 2% of cases (6 children), of which 2 patients received bronchoscopy. According to the retrospective study carried out at Itabashi Nihon University Hospital in Tokyo, Japan, between April 2013 and June 2018, and published in 2020, Fujisawa et al [10] reported that 18% of patients had a cough on admission, with respiratory distress in 1% of cases. In our series, only 2.42% of patients had a cough on admission, with dyspnea in 3.8% of cases. A retrospective study conducted between 2008 and 2013 and published in 2015 by Sink et al [12], summarized the sensitivity and specificity of functional and physical signs and child/parent interviewing. The primary imaging tool for assessing foreign body ingestions is standard radiography. Radiographs play an important role because most ingested foreign body s (83%) are radiopaque [12]. Views obtained should include the neck AP and lateral, the chest AP and lateral, and a standing AP abdominal radiograph which is useful in excluding the presence of pneumoperitoneum after ingestion of sharps [29]. According to Sink et al [12]: The presence of a radiopaque object on the chest X-ray was the most predictive finding of a foreign body overall. There were 45 false-negative chest X-rays and no false-positive ones, giving a sensitivity of 83% and a specificity of 100%. Sink et al also reported that of the 543 X-rays taken, 75.87% were radiopaque compared to 96% in our series. Delport et al [21] reported that standard radiography was indicated in 94% of patients, 63% of whom were chest radiographs. In our series, standard radiography was systematically performed in all our patients, 11% of whom were frontal and lateral views, and 27.33% were chest radiographs. Ultrasound can be used if the foreign body is located in the stomach, although it is less sensitive than CT. A retrospective series by Jecković et al [31], reported 18 children with gastric foreign bodies (aged 8 months to 7 years). Jecković et al reported that the majority of ingested foreign bodies were radiopaque and easily identifiable on abdominal radiography. However, three of the foreign bodies, a lollipop stick, a domino, and pieces of plastic toys, were radiolucent and were not detected on radiographs. All foreign bodies, including radiolucent ones, were identified in the stomach using ultrasound examination. CT is superior to standard radiography and can identify foreign bodies in 70-100% of affected patients [30]. The scanner is also useful for detecting complications such as perforation, fistula or abscess. Samujh et al [32] reported a case of appendicitis due to a screw in the appendix in a 4-year-old boy, who presented to the emergency department with acute abdominal pain in the right iliac fossa. There was no clear history of foreign body ingestion. However, there was a history of recurrent abdominal pain for 4 months. Flexible tube endoscopy is preferable in most cases because the foreign body can be directly visualized and manipulated (diagnostic and therapeutic value), and the surrounding gastrointestinal tract can be examined for possible complications (value in establishing the lesion assessment) [26,33]. In our series, diagnostic endoscopy was performed in 12 patients (4%) with extraction of the CE while in the study of Diaconescu et al in 14 patients (23%) [20] and Wai Pak et al in 41 patients (13%) [36]. The nature of ingested foreign bodies depends on the population studied, and therefore on geographical, economic, and sociocultural factors. They are often inorganic (metallic) in nature, and occasionally plastic or organic.
In Bangladesh, according to Chowdhury et al, ingested foreign bodies were inorganic in nature in 91.21% of cases distributed as follows: coins (26.37%), pins (20.88%), nails (6.59%) and batteries (5.49%). However, 31.86% of patients ingested different types of sharp objects and 23.08% of patients ingested different blunt metal objects. In addition, sharp object ingestion is higher in the older age group (>5 years) [37].
In Saudi Arabia, according to Khurshid et al, the nature of foreign bodies was as follows: Button batteries (49%), coins (21%), magnet (7%). Sharp objects such as nails, screws, pins and complex foreign bodies such as earrings, plastic parts were present in 14 (23%) patients. All foreign body s were inorganic in nature[38]. In Romania, according to Diaconescu et al, the most frequently ingested objects were coins (26.23%), unidentified metallic objects (13.11%), bones (8.19%) and button batteries (6.55%). Inorganic foreign body s represented 82% [20].
In the United States, in a 21-year study, Orsagh-Yentis et al reported that the most frequently ingested foreign bodies were coins (61.7%), followed by toy parts (10.3%), jewelry (7%), and batteries (6.8%), including 85.9% button batteries [39]. In our series, as in other studies, inorganic foreign body s were observed in 96% of our patients, of which only 1% were of plastic origin. The majority of foreign bodies were of a foam nature, with a clear predominance of coins found in 83% of patients. In our series, the location in the esophagus was the most frequent 91.69% of which 87.54% in the upper part of the esophagus. This is consistent with the various literature reviews such as that of Delport et al the location was 44% and of Lobeiras et al was 54%.
Only 1% of ingested foreign bodies are treated surgically due to a major complication (obstruction, perforation, abscess). The initial approach, therefore, in non-critical cases, is to monitor and wait for the object to pass on its own [38,39].
According to Ahmet Dursun, Tülin Öztaş [56], The most common type of EC was a coin (47%). The first pediatric cases reported in the literature involved a clothespin discovered in the stomach and a Meckel’s diverticulum perforated by a sunflower seed shell. Management included spontaneous passage (89%), endoscopy (7%), and open surgery (4%).
Clinical or clinico-radiological observation is generally indicated for asymptomatic patients with a history of non-threatening foreign body ingestion over periods of less than 24 hours and without any respiratory symptoms or history of esophageal disease or surgery. However, it is recommended to perform a remote etiological assessment in the event of a second episode of food blockage, even if spontaneously resolved [35]. Direct pharyngoscopy allows visualization of the hypopharynx, the regions between the base of the tongue and the mouth of the esophagus, and the larynx. It also facilitates the assessment of the mucosa covering these regions and the removal of any CE [42]. Fibroscopy allows the diagnosis of the esophageal foreign body, its extraction in most cases, and also constitutes an assessment of associated comorbidities. It has a major diagnostic interest, because it highlights a foreign body in 44% of cases where the X-ray fails despite strong clinical and anamnestic suspicion [34]. The Foley catheter or balloon catheter under X-ray guidance has a 98% success rate, but it can only be applied to blunt foreign bodies. Its use has the advantage of being significantly less expensive and faster than endoscopy [43]. In Chad, a study by Lamblin et al [13] in 2018, 37 cases of extraction in children aged 0 to 15 years were analyzed. These involved coins and button batteries in 92% and 8% of cases respectively in the upper third of the esophagus. All patients were under general anesthesia, including 23 patients under general anesthesia with spontaneous ventilation (62.2%) and 14 under general anesthesia with orotracheal intubation (37.8%). The Foley catheter was the method used in 43.2%. According to Lamblin et al [13], the use of the Foley catheter for the extraction of foreign bodies from the upper third of the esophagus is a reliable method in case of unavailability of endoscopy, the systematic use of fluoroscopy could limit the risk of failure and the presence of a visceral surgeon is necessary in case of failure or complication related to the procedure. Surgery is rarely performed, but is relatively successful. It is indicated in cases of perforation, other complications, and failure of foreign body extraction by other previous techniques [13]. The North American Society of Pediatric Gastroenterology, Hepatology, and Nutrition (NASPGHAN) Endoscopy Committee has revised recommendations regarding the timing of endoscopic intervention. The presence of esophageal button batteries requires emergency removal within 2 hours, regardless of the presence of symptoms [44]. Long foreign bodies lodged in the esophagus require removal within 24 hours, regardless of the presence of symptoms. Most foreign body’s in the small intestine are evacuated spontaneously without complications. Therefore, physicians should reassure children and/or parents and advise them to check the child’s stool. Coins are the most commonly ingested foreign body’s by children. More than 250,000 cases of coin ingestion by children were reported in the United States between 1994 and 2003 [47]. Factors influencing the spontaneous passage of a coin are its location in the esophagus, the child’s age, and the size of the coin. Typically, the spontaneous passage rate of swallowed coins in children is about 30% [48]. Conners et al suggested that coins lodged in the upper and middle esophagus require endoscopic extraction, although it has been observed that 60% of coins lodged in the lower esophagus passed spontaneously [46, 48]. In our series, coins accounted for 83% of the foreign bodies found. The study by Lee et al [11] showed that all 7 children who ingested button batteries less than 15 mm were asymptomatic without any complications, while the 5 children who swallowed batteries larger than 15 mm had moderate (n=3) to severe (n=2) complications while in our series of studies, patients who ingested button batteries were 9 (3.11%). According to Amani Mubarak et al, all patients with mucosal injury after battery removal should be hospitalized and monitored closely. In such patients, re-examination within 2-4 days after removal may be considered as it may provide useful prognostic information. A clear liquid diet may be started if there is no evidence of perforation on esophagography. Esophagography may be performed 1-2 days after removal. In complex cases, this period should be extended until the patient’s condition stabilizes [58].
However, if multiple magnets or a single magnet with a metal CE have been ingested, contact between these ingested magnets or the magnet and the metal CE and the mucosal surfaces of different parts of the body may cause pressure necrosis of the mucous membranes, as well as intestinal obstruction, fistula and/or perforation; therefore, surgery is necessary in these cases [49,50]. In our series, only one patient was admitted for ingestion of a magnet (0.34%). Sharp or pointed foreign body’s such as safety pins, nails, hairpins, screws, needles, thumbtacks can lead to serious complications such as ulceration and/or perforation of the esophagus, tracheal fistula and/or abscess formation, peritonitis, aortoesophageal fistula and even death [52]. In general, intestinal foreign body’s are known to cause perforation in <1% of patients; however, sharp or pointed FBs can cause perforation in 15-35% of patients. According to Qing-Jiang [57] Chen 44 patients presented with intestinal perforation complication and 10 with intestinal obstruction. Therefore, it is preferable to remove FBs from the esophagus or stomach whenever possible. In particular, in recent times, early diagnosis and rapid extraction by endoscopy have reduced the incidence of adverse effects related to the ingestion of sharp or pointed FBs [53]. In a Korean study by Lim et al.19]; the fish bones represent 50.1% of ingested CE against 0.34% in our series (Figure 12). Lim et al [19] reported that ingested fish bones in children were most often detected in the pharynx (57.7%). In our series, 15.57% of patients had minimal to moderate complications detected by X-ray or endoscopic exploration, whereas in studies done: In Taiwan the study of Lin et al presented with erosive esophagitis (2.6%) [54], Chinksi et al in Argentina an esophageal perforation (0.31%).
Outcomes and prognosis for pediatric foreign body ingestion are generally good, as most patients tolerate the passage of ingested objects without intervention. Even in scenarios where intervention is required, mortality and morbidity are low. High-risk ingestions (button batteries, magnets, sharp objects) can be associated with complications and, in rare cases, death [55].Foreign bodies in the esophagus can cause mediastinitis, perforation, and pneumomediastinum. Magnets are also known to cause damage to the mucous membranes of the small intestine, leading to perforation. Button batteries are the most morbid and should therefore be removed as soon as the diagnosis is made. Finally, foreign body removal procedures can also cause complications, whether due to anesthesia or the procedure.
The majority of FBs are accidentally ingested by children. Prevention therefore remains the best treatment for children and requires the intervention of all the structures concerned: the family unit, industrialists and public authorities, medical and paramedical staff. For primary prevention, parent education is of paramount importance and secondary prevention aims to reduce the consequences through faster, appropriate support.
Conclusion
Foreign body ingestion is a major problem in early childhood and poses a diagnostic and therapeutic challenge.
The vast majority of foreign bodies accidentally ingested by children migrate through the digestive tract without complications, and monitoring is generally sufficient. Therefore, certain situations present a significant risk of serious and sometimes fatal complications, such as necrotic perforations and gastrointestinal bleeding, the release of toxic substances, obstruction, and respiratory tract infections. Prevention is of great interest in reducing these accidents and their complications througheducation and information of parents on the dangers and risks of ingestion of foreign bodies.
References
- Maaloul S, Kmiha S, Yaich K, Thouraya J, Damak H, et Al. Epidémiologie des accidents domestiques de l’enfant: expérience d’un Service de Pédiatrie Générale du sud tunisien. Pan Afr. Med. J. 2019; 8688: 1–8.
- S Kim, B Park, I Kong, H Choi. Analysis of ingested foreign bodies according to age. type and location : a retrospective observational study. Clin. Otolaryngol. 2016; 1–6.
- R Wyllie. Foreign bodies in the gastrointestinal tract. Curr. Opin. Pediatr. 2006; 18: 563–564.
- D Passali, D Gregori, G Lorenzoni, S Cocca, M. Loglisci, et Al. Passali. Foreign body injuries in children : a review. ACTA Otorhinolaryngol. Ital. 2015; 35: 265–271.
- J Mihajlo, A. Sudha, B. Svetlana, L. Jovan. Is ultrasound useful in detection and follow-up of gastric foreign bodies in children?. Clin. Imaging. 2013; 37(6):1043–1047.
- T. Schuldt, W. Großmann, N. Weiss, A. Ovari, R. Mlynski, S. Schraven. Aural and nasal foreign bodies in children – Epidemiology and correlation with hyperkinetic disorders. developmental disorders and congenital malformations. Int. J. Pediatr. Otorhinolaryngol. 2018; 118(2018): 165–169.
- D. Gregori, F. Foltran, S. Ballali. P. Berchialla. H. Rodriguez, P. et Al. Zaupa. The Susy Safe project overview after the first four years of activity. Int. J. Pediatr. Otorhinolaryngol. 2012; 76: SUPPL1.
- S. Green. Ingested and aspirated foreign bodies. Pediatr. Rev. 2015; 36(10): 430–436.
- M. Lakdhar, Idrissi M, Hida L. ingestion de corps étrangers chez l ’enfant : à propos de 105 cas. Arch. Pediatr. 2011; 18(8): 856–862.
- F. Jumpei, M. Tomokazu, K. Kengo, Y. Ryuta. H. Maiko, I. Morioka. Medicina Age-Specific Differences in Foreign Bodies Ingested by Children : A Cohort Study of 252 Japanese Cases. Medicina (B. Aires). 2020; 56(39): 11–14.
- J. Lee, J. Lee, J. Shim, J. Lee, B. Eun, K Yoo. Foreign body ingestion in children: Should button batteries in the stomach be urgently removed?. Pediatr. Gastroenterol. Hepatol. 2016; 19(1): 20–18.
- J. Sink, D. Kitsko, K. Deepak, W. Matthew, P. Jeffrey. Diagnosis of Pediatric Foreign Body Ingestion: Clinical Presentation. Physical Examination and Radiologic Findings. Ann. Otol. Rhinol. Laryngol. 2016; 125(4): 1–9.
- A. Lamblin, C. Derkenne, A. Schwartz, P. Pasquier, R. Gorioux, P. Wey. Case series. Pan Afr. Med. J. 2018; 8688: 1–7.
- R. SidibeCorps étrangers digestifs de l’enfant. 2019.
- D. Gummin, B. Mowry, A. Spyker, E. Brooks, O. Fraser, W. Banner. 2016 Annual Report of the American Association of Poison Control Centers’ National Poison Data System (NPDS): 34th Annual Report. Clin. Toxicol. 2017; 55(10): 1072–1252.
- A. Arana, B. Hauser, S Hachimi-Idrissi, Y. Vandenplas. Management of ingested foreign bodies in childhood and review of the literature. Eur. J. Pediatr. 2001; 160(8): 468–472.
- A. Lobeiras, A. Zugazabeitia, N. Uribarri, S. Mintegi. Emergency department consultations due toforeign body ingestion. An. Pediatría English Ed. vol.
- M. Cevik, M. Gókdemr, M. Boleken, O. Sogut, C. Kurkcuoglu. The characteristics and outcomes of foreign body ingestion and aspiration in children due to lodged foreign body in the aerodigestive tract. Pediatr. Emerg. Care. 2013; 29(1): 53–57.
- C. Lim, M. Park, H. Do, J. Yeom, J. Park, et Al. Park.Factors associated with removal of impactted fishbone in children. suspected ingestion. Pediatr. Gastroenterol. Hepatol. Nutr. 2016; 19(3): 168–174.
- S. Diaconescu, N. Gimiga, I. Sarbu, G. Stefanescu, C. Olaru, et Al. Ioniuc.Foreign Bodies Ingestion in Children : Experience of 61 Cases in a Pediatric Gastroenterology Unit from Romania. Gastroenterol. Res. Pract. 2016; 2016: 1–6.
- C. Delport ; P. Hodkinson, B. Cheema. Investigation and management of foreign body ingestion in children at a major paediatric trauma unit in South Africa. African J. Emerg. Med. vol. 5. no. 4:176–180. 2015.
- P. Louie, R. Alpern, M. Windreich. Witnessed and unwitnessed esophageal foreign bodies in children. Pediatr. Emerg. Care. 2005; 21(9): 582–585.
- K. Athanassiadi, M. Gerazounis, E. Metaxas, N. Kalantzi. Management of esophageal foreign bodies: a retrospective review of 400 cases. Eur. J. Cardio-Thoracic Surg. 2002; 21(4): 653–656.
- A. Dahshan. Management of ingested foreign bodies in children. J Okla State Med Assoc. 2001; 94(6): 183.
- G. Cesare, D. Gregori, A. Chinski, C. Tiscornia, H. Botto, et Al. Nieto. International Journal of Pediatric Otorhinolaryngology Management of foreign bodies in the airway and oesophagus. Int. J. Pediatr. Otorhinolaryngol. 2012: 84–91.
- NJ. Peters, JK. Mahajan, M. Bawa, A. Chabbra, R Garg, KLN Rao. Esophageal perforations due to foreign body impaction in children. J. Pediatr. Surg. 2015; 9417407077: 1–4.
- R Naidoo, A Reddi. Chronic Retained Foreign Bodies in the Esophagus. Ann Thorac Surg. 2004; 4975(3): 2218–2220.
- R Mahajan, V Prashanth. A retrospective review of complicated foreign bodies of upper aerodigestive tract. Int. J. Otorhinolaryngol. Head Neck Surg. 2019; 5(3): 734–738.
- A Pinto, C. Lanza, F. Pinto, R. Grassi, L. Romano, et Al Brunese. Role of plain radiography in the assessment of ingested foreign bodies in pediatric patients. Semin Ultrasound CT MR. 2015; 36: 21–7.
- C. Sugawa, H. Ono, M. Taleb, C. Lucas, C. Sugawa, et Al. Ono.Endoscopic management of foreign bodies in the upper gastrointestinal tract : A review. World J Gastrointest Endosc. 2014; 6(10): 475–481.
- M. Jeckovic, S. Anupindi, S. Barbir, J. Lovrenski. Is ultrasound useful in detection and follow up of gastric foreign bodies in children?. Clin Imaging. vol. 2013; 37: 1043–7.
- R. Samujh, K. Mansoor, I. Khan, A. Mannan. Case Reports. INDIAN Pediatr. 2007; 44: 611–612.
- A. Dahshan, G. Donovan Kevin. Bougienage versus endoscopy for esophageal coin removal in children. J Clin Gastroenterol. 2007; 41: 454.
- L. Michaud L. endoscopie digestive interventionnelle chez l’enfant. Arch Pédiatr. 2006; 13: 399–404.
- L. Zgarni, J. Letard, M. Happy Nono, M. BeauchantCorps étrangers de l’oesophage. EMC Gastro-entérol. 2009; 9: 1–6.
- M. Wai Pak, W. Chung Lee, H. Kwok Fung, C. van Hasselt. A prospective study of foreign-body ingestion in 311 children. Int. J. Pediatr. Otorhinolaryngol. 2001; 58(1): 37–45.
- T. Chowdhury, D. Sadab, M. Sajid, A. Farooq.Asian Journal of Medical and Biological Research Foreign body ingestion by children : an analysis of age and types at a tertiary hospital in Bangladesh. Asian J. Med. Biol. Res. 2017: 6: 299–304.
- Z. Khurshid, A. Ali, S. Abdul, A. Al, T. Alnafisah. Foreign Body Ingestion in Children : A Hospital Based Experience in Riyadh. ACTA Sci. Paediatr. 2019; 2(10): 13–19.
- D. Orsagh-yentis, R. Mcadams, K. Roberts, L. Mckenzie. Foreign-Body Ingestions of Young Children Treated in US Emergency Departments : 1995 – 2015. Pediatrics. 2019; 143( 5): 1–8.
- G. Sharieff, T. Brousseau, J. Bradshaw, J. Shad. Acute esophageal coin ingestions: is immediate removal necessary?. Pediatr Radiol. 2003; 33(1): 859–63.
- J. Soprano, G. Fleisher, K. Mandl. The spontaneous passage of esophageal coins in children. Arch Pediatr Adolesc Med. vol. 153. 1999; 10: 1073–6.
- A. Barros, D. Dehesdin. Corps étrangers de l’oesophage. EMC Oto-rhino-laryngo. 2000; 20: 835–40.
- S. Monat, J. Barouk, M. Le Rhun. Prise en charge des corps étrangers du tractus digestif supérieur. Hépato-gastro-entérologie. 2001; 8(1): 179–87.
- RE Kramer, et al. Management of ingested foreign bodies in children: A clinical report of the NASPGHAN endoscopy committee. J. Pediatr. Gastroenterol. Nutr. 2015; 60(4): 562–574.
- N. Lazar. La problématique posée par l’ingestion des piles boutons chez l’enfant (à propos de 12 cas). 2016.
- M. Waltzman. Management of esophageal coins. Curr Opin Pediatr. 2006; 18: 571–574.
- X. Chen, S. Milkovich, D. Stool, J. Reilly, G. Rider, A Van. As Pediatric coin ingestion and aspiration. Int J Pediatr Otorhinolaryngol. 2006; 70: 325–329.
- M. Waltzman, M. Baskin, D. Wypij, D. Mooney, D. Jones, G. Fleisher. A randomized clinical trial of the management of esophageal coins in children. Pediatrics. 2005; 116: 614–619.
- J. Lee, J. Lee, M. Kim, Y. Choe. Initial location determines spontaneous passage of foreign bodies from the gastrointestinal tract in children. Pediatr Emerg Care. 2011; 27: 284–289.
- J. Hwang, M. Park, S. Choi, W. Park. How strong construction toy magnets are! A gastro-gastro-duodenal fistula formation. J Pediatr Gastroenterol Nutr. 2007; 44: 291–292.
- SZ Hussain, A Bousvaros, M Gilger, P Mamula, S Gupta, et Al. Kramer.Management of Ingested Magnets in Children. J. Pediatr. Gastroenterol. Nutr. 2012; 55: 239–242.
- A Aktay, S Werlin. Penetration of the stomach by an accidentally ingested straight pin. J Pediatr Gastroenterol Nutr. 2002; 34: 81–82.
- R Palta, A Sahota, Bemarki P, Salama N, Simpson, L Laine. Foreign-body ingestion: characteristics and outcomes in a lower socioeconomic population with predominantly intentional ingestion. Gastrointest Endosc 2009; 69(3 Pt 1): 426-433.
- C Lin, A Chen, J Tsai, H Wei, K Hsueh, W Lin. Endoscopic removal of foreign bodies in children. Kaohsiung J. Med. Sci. 2007; 23(9): 447– 452.
- D Yardeni, A Coran, E Golladay, H Yardeni. Severe esophageal damage due to button battery ingestion : can it be prevented ?. Pediatr Surg Int. 2004; 20: 496–501.
- Ahmet Dursun. Tülin Öztaş Management of Foreign Bodies Crossing the Gastroesophageal Junction in Children. TurkArchPediatr. 2023.23023.
- Qing‑Jiang Chenzt, et al. Management of foreign bodies ingestion in children. World Journal of Pediatrics. 2022; 18: 854–860.
- Amani Mubarak. et al. Diagnosis.Management, Prevention of Button Battery Ingestion in Childhood: A European Society for pediatric Gastroenterology Hepatology and Nutrition Position Paper. JPGN. 2021; 73: 129–136.