
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Cerebrospinal fluid lab analysis as a helper of meningeal carcinoma diagnostic: A case Report
*Corresponding Author : María Teresa Ramírez Sánchez
Professor, Universidad Nacional Autónoma de México UNAM, Mexico.
Email: marylupin1227@gmail.com
Received : May 01, 2025
Accepted : May 23, 2025
Published : May 30, 2025
Archived : www.jcimcr.org
Copyright : © Ramírez SMT (2025).
Abstract
In this research paper, we present a meningeal carcinoma clinical case in a 61 year old woman, as a result of a lung adenocarcinoma infiltration, with an emphasis on the importance of clinic laboratory analysis.
Citation: Ramírez SMT. Cerebrospinal fluid lab analysis as a helper of meningeal carcinoma diagnostic: A case report. J Clin Images Med Case Rep. 2025; 6(5): 3613.
Introduction
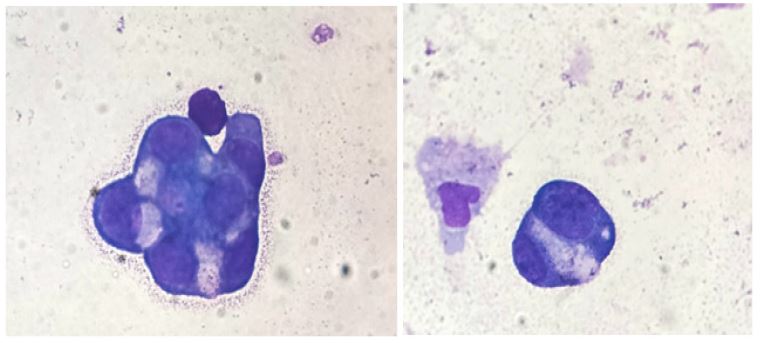
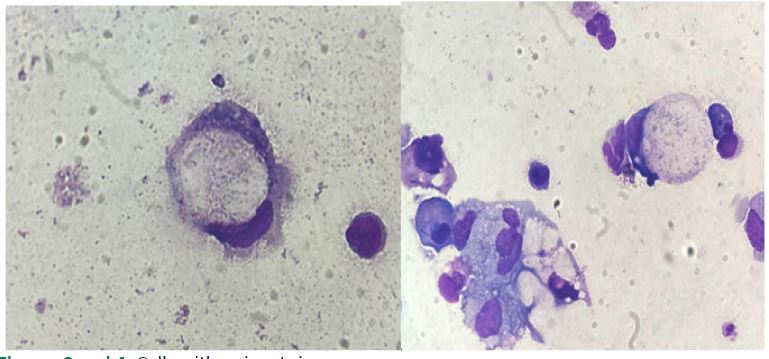
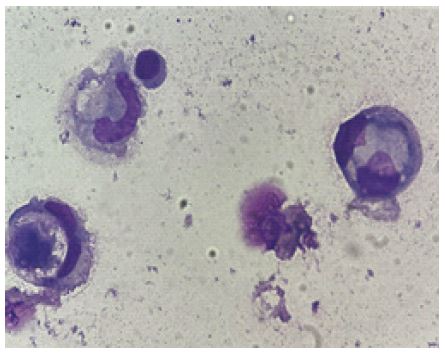
Meningeal carcinoma is defined as a dissemination of tumoral Cells In Cerebrospinal Fluid (CSF) and can manifest primarily in the brain or secondarily as a result of infiltration from another site. The tumoral cells travel from the primary site to the meninges. It is a risk of complication in 3 to 8% of all cancer patients [3]. Adenocarcinoma is the main cancer correlated with meningeal carcinoma [1]. Generally, the main organs from which a patient could acquire the secondary illness of meningeal carcinoma includes breasts, lungs and skin (melanoma) [2,5,8]. It is important to mention that usual treatment does not reach the blood-brain barrier [1,2,12,13]. Meningeal carcinoma is a fatal disease, with bad prognostics. The life expectancy can go from 3 to 6 weeks to 3 to 4 months with the correct treatment consistent in intrathecal chemotherapy, local radiotherapy, or systemic chemotherapy [3,4,7,8]. We present the case of a 61 year old female patient who was previously diagnosed with a non operable, left lung adenocarcinoma. The patient arrived for a routine revision by the oncology service at the INER (Instituto Nacional de Enfermedades Respiratorias) when she suffered a tonic-clonic seizure with a loss of sphincter control and postictal state. The patient was transported to the emergency hospital room and required a review by the neurology service and a tomography test. During the tomography, the patient went through non-voluntary movements on the extremities and pharyngeal reflex. After the seizure, the patient was disoriented and made indistinct noises. A gadolinium magnetic resonance was ordered and a lumbar puncture was made to the patient. The CSF was sent to the lab to run a meningitis panel, cytologic and cytochemistry test to discount suspicions of possible tuberculosis. A 2 milliliter sample of CSF was sent to the Organic Liquid area of the clinical laboratory with an order to discount infiltration. The sample received was translucent and colorless. The sample had to go through a chemical and microscopic analysis. This last analysis consisted of two different parts. The first one is the cellular counting in the Neubauer chamber (white and red blood cells) and the second one is cytocentrifugation, followed by the Wright stain and differential counting by a white light microscope. Microscopic stain observation was made in order to report a differential white blood cell counting. We observed a series of unusual cells that are not typical in cerebrospinal fluid. First, we observed the presence of a small amount of cell clusters in a three-dimensional disposal (Figures 1 and 2), cells with a signet ring appearance (Figures 3 and 4) and cells demonstrating cannibalism (Figure 5).
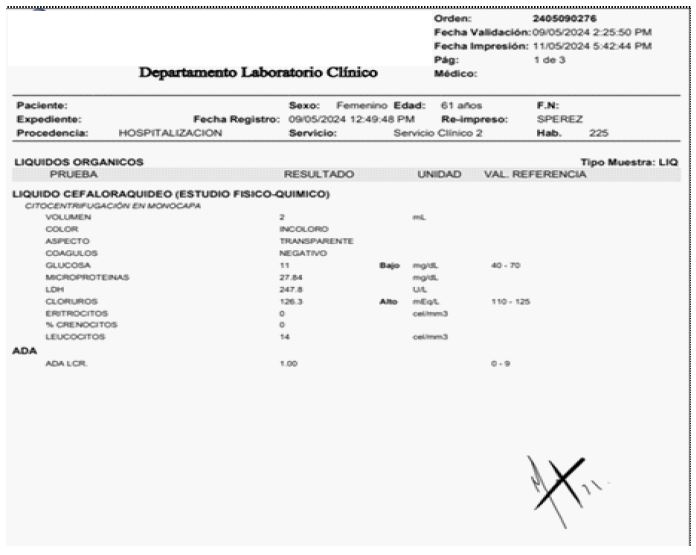

The CSF was analyzed to measure the various concentrations of glucose, LDH, ADA, chloride, proteins, white blood cells and red blood cells (Figure 6). We described the findings in the observation section on the report with the suggestion to send the CSF for a cytology test (Figure 7).
Negative results were obtained for tuberculosis from gram stain, Ziehl-Neelsen stain, culture and GeneXpert test. Sixteen days after the patient was hospitalized, a new evaluation was made by the neurology service in contrasted magnetic resonance imaging (MRI). They observed hyperintensity data, right frontotemporal edema with a meningeal enhancement at right temporal level with a suggestion of meningeal carcinoma. The disorientation of the patient continued so another lumbar puncture was made and the CSF was sent to cytological testing at the Instituto Nacional de Neurocirugía. After six days, a positive result was reported with an infiltration by malignant neoplasia characterized by neoplastic cells with basophilic, scarcely vacuolated citoplasma, megalia and nuclear pleomorphism findings. Considering the poor health of the patient, the prognosis and the advancement of the disease; the patient was discharged for optimal welfare with home care.
Discusión
Due to the fatal consequences of meningeal carcinoma, it is important for the health care personnel to pay careful attention whenever a patient presents even slight neurological changes (cerebral, cranial and spinal) symptoms such as headache, mental changes, nausea, vomiting, dizziness, diplopia, dysphasia, hearing loss, confusion, loss of eyesight, neck pain or back pain among others [2,6,12,14]. Whenever these symptoms appear in a patient, it is necessary to consult with neurological services which can provide an early diagnosis and subsequent treatment that can prevent greater neurological damage and extend the life span of the patient as much as possible [9]. The challenges the diagnosis presents include appropriate observation and supervision by the health care personnel in order to request laboratory tests (imaging, cytochemical and pathological). It is important to mention that when assessing the clinical history of the patient, both the symptoms and the results of the imaging test could be inconclusive (for example in the case presented, the first imaging was of non utility), the chemist analysis can present subtle changes which are also inconclusive. In the literature, it is mentioned that low glucose levels, high protein and leukocyte levels are common in patients with meningeal carcinoma [2,5-7,12,14]; in this case we found low glucose levels but the protein level was normal, and the leukocyte counting was just slightly elevated. Thus, the only other possibility to find an anomaly is cellularity; however there is a high probability of not finding any tumoral cells [10,13] (nor in the clinic lab nor in the cytological study). In addition to these difficulties, in the diagnostic process it is common for a time period of seven days to pass until a result of a cytological test is released. (For example, it is approximately 7 days in INER). The gold standard for a meningeal carcinoma is a positive result from a cytological test, the health care personnel must consider, that in order to increase the possibility of finding tumoral cells in a patient with meningeal carcinoma, more than one sample (2 or 3) of CSF should be taken over the duration of a few days apart for posterior studies [2,4,8,13]. It is also possible that with the support of the imaging study, the health care personnel decided to do either a lumbar or a ventricular puncture [6]. The CSF analysis in the clinical laboratory presents a first approach to possible abnormalities that could relate to pathologies presented on the patient. In order to make this possible, it is important to consider all the factors that have an impact on the sample quality and in the posterior analysis (pre- analytical, analytical and post-analytical factors). As a pre-analytical consideration, it is important for the CSF sample to be transported as soon as possible because of the degradation that the cells may suffer. This degradation jeopardizes the sample stability and therefore the opportunity of obtaining an accurate result. With this consideration it becomes important that the medical personnel provide the clinical information for a better sample process. In the analytical process, the CSF test (cytochemical) is offered by the organic liquid service on the Clinic Laboratory on INER. It is constituted by a physical observation (color, aspect), a chemical study (consistent on glucose, microproteins, lactic dehydrogenase and chloride levels), a microscopic analysis of red and white blood cells concentration and a differential count of white blood cells. The microscopic analysis of the CSF stain (Wright) is made by a concentration technique in which a cytocentrifuge is used to preserve the cells’ characteristics. By using this methodology, we can observe the cellularity present on the sample and report the dominance of white blood cells existing but also presents us with the possibility of observing any nonnormality on white blood cells or the presence of cells that are not normal in this fluid. For this purpose, the analyst must be used to the “normal type of cells” in the fluid under analysis (such as ependymal cells on CSF) in order to recognize abnormal cells when located, make an appropriate report and even suggest to the doctor a complementary test for an accurate diagnostic. The main characteristics that should be considered as non normal and therefore should be reported are: polymorphism with big cells and nucleus of different sizes, a high nucleus to cytoplasm ratio (N:C ratio), basophilic cytoplasm and a three-dimensional disposition. Every single time that an analyst in the clinical laboratory observes cells with any of these characteristics, the finding should be reported with a description in order to alert the doctor and guide them to complementary studies such as cytology. The principal post-analytical consideration is the appropriate report of the findings. In the case presented, we reported the findings on the microscopic observation of cells that were not normal in this fluid, we made a remark on the findings of cluster of cells with three-dimensional disposition (normally associated with adenocarcinoma), signet ring like cells and cannibalism. Later on, the diagnosis of meningeal carcinoma as a result of a lung adenocarcinoma was confirmed by the result of the cytological study (Papanicolaou stain).
Conclusion
Even though the Cytology laboratory is responsible for examining the cells of the fluids and who reports a positive or negative result, in this case we marked the importance of the clinical laboratory since this first description was made in a time period of two hours from the reception of the sample to the report and therefore the doctor had an increase in suspicion of neoplastic cells infiltration from the lung adenocarcinoma. In the presented case, we could corroborate that for an integral attention to the patient it is necessary for there to be more interdisciplinary work: the suspicion of the doctor, the consultation with the neurological service, the imaging studies, the obtention of CSF and immediate transportation to the laboratory (with a medical request that provides information about the clinical suspicion for a “intentional search”), the knowledge of the staff of the clinical laboratory, and the report of the findings. It is also important to establish communication routes that vinculate the staff of the laboratory with the doctor, in a way that can guarantee effective communication for the benefit of the patient.
References
- Ano S, Satoh H, Nakazawa K, Ohtsuka M, Anami Y, et al. Malignant meningitis secondary to lung adenocarcinoma: an unusual relapse. Intern Med. 2007; 46(20): 1749-51.
- Batool A, Kasi A. Leptomeningeal Carcinomatosis. 2023 Mar 27. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. 2024; 29763037.
- Dixit R, Goyal M, Nowal P, Indushekhar V. Adenocarcinoma lung presenting with meningeal carcinomatosis. Monaldi Arch Chest Dis. 2021; 92 (2).
- Fields MM. How to recognize and treat neoplastic meningitis. J Adv Pract Oncol. 2013; 4(3): 155-60.
- Lee SJ, Lee JI, Nam DH, Ahn YC, Han JH, et al. Leptomeningeal carcinomatosis in non-small-cell lung cancer patients: impact on survival and correlated prognostic factors. J Thorac Oncol. 2013; 8(2): 185-91.
- Lombardi G, Zustovich F, Farina P, Della Puppa A, Manara R, et al. Neoplastic meningitis from solid tumors: new diagnostic and therapeutic approaches. Oncologist. 2011; 16(8): 1175-88.
- Ramos-Clemente RJ, Duran FE, Pérez RM, Domínguez HJ. Un paciente con. Carcinomatosis Meníngea por invasión dural de Metástasis Craneal. Rev Clín Med Fam. 2010; 3(3): 237-239.
- Ríos MC Castillo, Moreno MM, Junco MR, Echavarría ME Almira SE, Pérez F, Oyifioda AE. Carcinomatosis Leptomeníngea: Presentación de un caso y revisión del tema. Revista Chilena de Neurocirugía. 2013; 39: 160-165.
- Rodríguez MJ, Macias MR, Gomez-Ulla AJ. Carcinomatosis meníngea: distintos casos con los mismos resultados. Med Paliat. 2014; 21 (3): 121-125.
- Sabater AL, Sadaba LM, de Nova E. Ocular symptoms secondary to meningeal carcinomatosis in a patient with lung adenocarcinoma: a case report. BMC Ophthalmol. 2012; 12: 65.
- Suresh PK, Kini JR, Basavaiah SH, Kini H, Khadilkar UN, et al. Neoplastic Meningitis: A Study from a Tertiary Care Hospital from Coastal India. J Cytol. 2018; 35(4): 255-259.
- Wasserstrom WR, Glass JP, Posner JB. Diagnosis and treatment of leptomeningeal metastases from solid tumors: experience with 90 patients. Cancer. 1982; 49 (4): 759-72.
- Yoo IK, Lee HS, Kim CD, Chun HJ, Jeen YT, et al. Rare case of pancreatic cancer with leptomeningeal carcinomatosis. World J Gastroenterol. 2015; 21(3): 1020-3.
- Zamora BT, Bolaños BH, Cáceres AM, Arias LS. Carcinomatosis meníngea, un desafío diagnóstico. Reporte de caso. Revista Facultad Ciencias de la Salud Universidad del Cauca. 20(1): 46-49.