
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 6
Simultaneous intrathoracic and intrabiliary rupture of hepatic hydatid cysts
Basma Dghoughi*; Basma Beqqali; Hajar Andour; Hiba Zahi; Nabil Moatassim Billah; Itimad Nassar; Kaoutar Imrani
Department of Central Radiology, Ibn Sina Hospital Center, Rabat Morocco.
*Corresponding Author : Basma Dghoughi
Department of Central Radiology, Ibn Sina Hospital Center, Rabat Morocco.
Tel: 00212668145175;
Email: basma.dghoughi01@gmail.com
Received : May 01, 2025
Accepted : May 23, 2025
Published : May 30, 2025
Archived : www.jcimcr.org
Copyright : © Dghoughi B (2025).
Citation: Dghoughi B, Beqqali B, Andour H, Zahi H, Billah NM et.al. Simultaneous intrathoracic and intrabiliary rupture of hepatic hydatid cysts. J Clin Images Med Case Rep. 2025; 6(5): 3614.
Description
Hydatidosis is a parasitic disease caused by Echinococcus granulosus, a zoonotic cestode that is worldwide distribution, but especially endemic in some areas such as the Mediterranean region. It is caused by accidental ingestion of E. granulosus eggs, leading to cyst formation in organs, primarily the liver (50-70%), but also in the lungs, spleen, kidneys, and brain [1].
Ultrasonography (USG) is the preferred screening method for hepatic hydatid cysts (HHC) and is also used to verify the efficiency of treatment. Computed Tomography (CT) exhibits high sensitivity and specificity in the diagnosis of hydatid disease. It plays a crucial role in detecting calcifications in the cyst wall, evaluating complications, illustrating bone lesions, and is highly recommended to search for extra hepatic localizations. Magnetic Resonance Imaging (MRI) excels in displaying biliary connections [2]. HHC is often asymptomatic, but larger cysts may cause abdominal pain, or complications: compression (of the biliary tract resulting in jaundice, portal vein resulting in portal hypertension, or inferior vena cava resulting in Budd Chiari syndrome), rupture (intra biliary, intra thoracic or peritoneal), super infection and hemorrhage [3]. Morbidity is usually secondary to the cyst’s free peritoneal rupture with or without anaphylaxis [1].
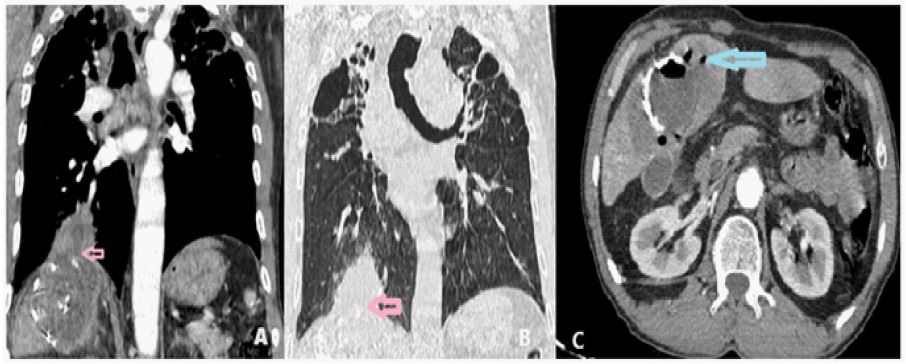
A 63-year-old man from a rural area of Morocco, recently diagnosed with HHC, presented for thoracic CT to examine potential cyst spread. He had a productive cough. CT imaging revealed emphysematous lungs and a thick-walled cystic formation in the right paracardial area, surrounded by ground-glass opacity, and communicating with a calcified liver dome cyst through a diaphragmatic defect. The adjacent bronchus were thickened but no intrabronchial material was seen. Abdominal slices showed another cyst in the segment V, containing air, with signs of biliary rupture and aerobilia. MRI confirmed communication with the gallbladder and a duodenal fistula, explaining the air presence in bile ducts.
Declarations
Acknowledgements: The authors would like to express their gratitude to the professors and all the colleagues who participated in the completion of this work.
Conflict of interest: No conflicts of interest.
Funding: No fundings were received for this work.
Ethical approval: No approval is required.
Consent: written consent was obtained from the patient for anonymous use of his data.
References
- T. Gessese. Review on Epidemiology and Public Health Significance of Hydatidosis. Vet Med Int. vol. 2020; 2020. doi: 10.1155/2020/8859116.
- Pooja Mehta, Niranjan Khandelwal, and Mahesh Prakash. Radiological manifestations of hydatid disease and its complications. Trop Parasitol. 2016. doi: 10.4103/2229-5070.190812.
- E. Ferrer-Inaebnit, F. X. Molina-Romero, J. J. Segura-Sampedro, X. González-Argenté, and J. M. Morón-Canis. A review of the diagnosis and management of liver hydatid cyst. Revista Espanola de Enfermedades Digestivas. 2022; 114(1): 35–41. doi: 10.17235/reed.2021.7896/2021.