
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Anterior chest wall mucormycosis: A presentation of an aggressive fungal infection
Seema Khanna1; Sanjeev Kumar Gupta1; Satendra Kumar1; Ragini Tilak2; Umang Kumar Agrawal3*
1Professor, Department of General Surgery, IMS BHU, Varanasi, India.
2Professor, Department of Microbiology, IMS BHU, Varanasi, India.
3Junior Resident, Department of General Surgery, IMS BHU, Varanasi, India.
*Corresponding Author : Umang Kumar Agrawal
Junior Resident, Department of General Surgery, IMS BHU, Varanasi, India.
Email: doctorumang.agrawal@gmail.com
Received : May 05, 2025
Accepted : May 29, 2025
Published : Jun 05, 2025
Archived : www.jcimcr.org
Copyright : © Agrawal UK (2025).
Abstract
Mucormycosis is an aggressive, opportunistic fungal infection caused by fungi of the order Mucorales. It typically affects immunocompromised patients and is mostly associated with rhino-orbital-cerebral, pulmonary, and cutaneous involvement. Anterior chest wall mucormycosis is exceedingly rare and poses diagnostic and therapeutic challenges due to its aggressive nature and the proximity to critical structures. This report highlights an unusual presentation of mucormycosis involving the anterior chest wall and emphasizes the importance of multidisciplinary care.
Keywords: Mucormycosis; Anterior chest wall; Antifungal therapy; Surgical debridement.
Abbreviations: CRP: C-Reactive Protein; TLC: Total Leukocyte Count.
Citation: Khanna S, Kumar Gupta S, Kumar S, Tilak S, Kumar Agrawal U. Anterior chest wall mucormycosis: A presentation of an aggressive fungal infection. J Clin Images Med Case Rep. 2025; 6(6): 3621.
Introduction
Mucormycosis, caused by fungi of the order Mucorales, is a life-threatening infection predominantly seen in immunocompromised hosts. Rhino-orbital-cerebral and pulmonary forms are most common, while cutaneous manifestations, particularly on the anterior chest wall, are rare. The incidence of mucormycosis surged during the COVID-19 pandemic, linked to uncontrolled diabetes and corticosteroid use. Cutaneous mucormycosis often arises post-trauma or surgery, but hematogenous spread in diabetics is also documented. Diagnosis relies on histopathology and fungal culture, while treatment necessitates a combination of aggressive debridement and antifungal therapy. We report a rare case of anterior chest wall mucormycosis caused by Saksenaea vermiformis and its successful management.
Case report
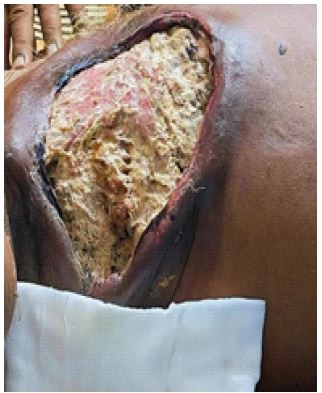
A 72-year-old male with a 5-year history of poorly controlled diabetes mellitus presented with a progressive swelling over the anterior chest wall for 15 days, which was associated with pain. There was history of fever for 5 days which was insidious in onset, high grade and intermittent in nature. There was no history of associated cough or dyspnoea, trauma, weight loss, malaise or night sweats. The patient had no other significant past medical history. Physical examination revealed an erythematous, tender, indurated swelling measuring 10 cm × 8 cm over the right anterior chest wall with areas of necrosis and black eschar formation with irregular, raised wound margins with purulent exudate. The wound also involved anterior chest wall muscles including the intercostal muscles. On palpation, the wound was tender and bled on touch (Figure 1). There was no associated lymphadenopathy. There were no other significant findings on systemic examination. The laboratory findings revealed a fasting blood glucose level of 280 mg/dl, with TLC of 22,000/microliter (or μL) with CRP level of 31.8 mg/dl (Normal < 0.3 mg/dl) at the time of presentation. Other haematological and biochemical parameters were within normal limits. The radiographic imaging revealed normal lung fields with soft tissue opacity over the anterior chest wall and the ultrasonography showed extensive soft tissue thickening with subcutaneous edema with cobblestoning pattern noted on the right side of chest wall associated with mildly thick organized collection of volume 1.3 x 1.2 x 1.4 cm suggestive of cellulitis with pus pockets.


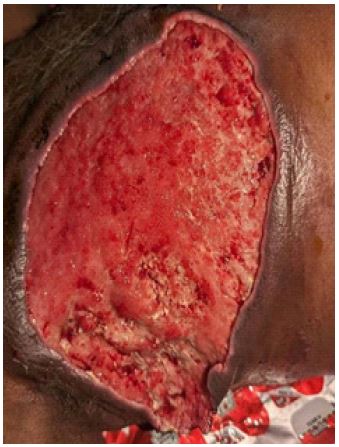

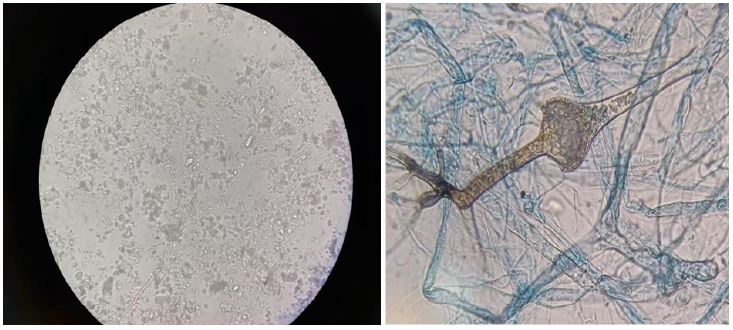
The biopsy from the wound suggested chronic inflammation with no evidence of malignancy. A complete tubercular work-up, culture from the ulcer, and serology were all negative. Tissue culture showed Klebsiella pneumoniae with sensitivity to Meropenem, Ertapenem and Imipenem. Due to the extensive tissue involvement, a fungal infection was suspected. Fungal staining and culture were also performed: the staining came out to be positive for fungal growth with the culture positive for Saksenaea vermiformis (Figure 6). Following the positive fungal culture, Amphotericin B was started intravenously at 1 mg/kg/day. Along with it, the entire wound and its margins (up to 2 cm) were debrided serially (Figure 2); however, it was not possible to clear the deep margins at the anterior chest wall (Figure 3). Wound was managed by daily dressing and debridement with the application of Amphotericin B topically over the wound following which the wound progressed towards healing (Figures 3 and 4). The entire surgical site was filled with granulation tissue within 12 days. Intravenous Amphotericin B was continued for 4 weeks and the serum potassium, blood urea and creatinine levels were monitored regularly followed by oral posaconazole for maintenance therapy. Intensive insulin therapy was initiated to optimize blood glucose levels. Broad-spectrum antibiotics were administered according to the culture sensitivity report to prevent secondary bacterial infections The patient showed gradual clinical improvement, with resolution of fever and reduction in swelling. Follow-up imaging and clinical examination at 3 months revealed no residual or recurrent infection with a healthy granulation covering the entire wound (Figure 5). There were no fresh complaints from the patient.
Discussion
Studies show that the development of mucormycosis was estimated to be 50 times higher during the COVID-19 pandemic compared to the pre-pandemic period. The studies have found a mortality rate of 43.5% in COVID-19–associated mucormycosis cases. Uncontrolled diabetes and high-dose corticosteroid therapy were significant risk factors [1]. Globally iincidence of Mucormycosis iincreased from 0.005-1.7 per million to much higher values post-COVID. In India, the prevalence in pre COVID times was 0.14 per 1,000 population, which was 80 times higher than in developed countries. While post-COVID it has risen to 7 cases per 1,000 COVID-19 patients (0.7%), which is a 5x increase compared to the general population [1,2]. Pre-COVID mortality has been reported to be 46%. Post-COVID mortality is 42.3% in COVID-associated cases. Diabetes-related mucormycosis mortality is 44–75% [1,2]. Mucormycosis of the anterior chest wall is an exceedingly rare presentation of an aggressive fungal infection. It typically occurs secondary to trauma, surgical wounds, or hematogenous spread in immunocompromised individuals. The rapid progression and potential for invasion into critical structures make early diagnosis and treatment imperative. Tissue necrosis and black eschar formation are the clinical hallmarks. Imaging is essential to determine the extent of involvement. Histopathology and fungal culture remain the gold standard for diagnosis [5,7]. Saksenaea vermiformis is a rare, thermotolerant fungus belonging to the order Mucorales. It is a member of the family Mucorales and is known for its pathogenic potential in humans and animals. This organism is one of the causative agents of mucormycosis, a severe and often life-threatening fungal infection. Like other Mucorales fungi, it can invade host tissues, especially following trauma or in immunocompromised individuals. It typically causes cutaneous and subcutaneous infections but can also lead to deeper or disseminated forms of mucormycosis in severe cases.
Clinical manifestations: It may present as cutaneous or invasive disease.
1. Cutaneous mucormycosis:
Often initiated by trauma, such as wounds, burns, or surgery, allowing the fungus to enter the body. Presents as necrotic lesions that may rapidly progress if not treated promptly.
Cutaneous mucormycosis can appear in two distinct ways:
• Superficial infections often start as blisters that ulcerate over time due to fungal invasion of the skin’s blood supply.
• Gangrenous infections progress more rapidly and typically have worse outcomes [6].
2. Invasive disease: Rarely, Saksenaea vermiformis can cause invasive infections involving bones or internal organs, especially in patients with suppressed immunity [3,4].
Cutaneous infections generally follow injuries like burns, insect bites, or surgical wounds. In our case, no obvious injuries were identified. Routine tests ruled out other conditions, and clinically, when no improvement was seen, a fungal infection was suspected and confirmed through laboratory culture.
The standard therapy for mucormycosis is Amphotericin B, administered at doses of 1-1.5 mg per kilogram of body weight daily. In this case, the patient received the medication for four weeks, along with serial surgical debridement of the infected tissue. No obvious side effects, such as low potassium levels and kidney function impairment occurred. Debridement was crucial for controlling the infection. A combination of mechanical and chemical debridement was done. Aggressive surgical debridement is critical to remove infected tissue. Liposomal amphotericin B is the first-line antifungal agent, with posaconazole or isavuconazole used for maintenance or refractory cases. Optimizing underlying risk factors, such as diabetes control, is essential. A recent development in the management of mucormycosis is Deferasirox, an iron chelator which is given in the dose of 20 mg/kg/day & reduces the availability of free iron, necessary for fungal growth. This can be combined with posaconazole as a salvage therapy for extensive lesions, or for those who are resistant to polyenes [7]. A prompt, multidisciplinary management improves survival and reduces the risk of recurrence.
Conclusion
Anterior chest wall mucormycosis is a rare but aggressive infection. This case implies and signifies the importance of early recognition, multidisciplinary care, and combined surgical and medical management in achieving favourable outcomes. The duration of any antifungal therapy depends mostly on the clinical response and a serial aggressive debridement should be performed to achieve a faster cure and to avoid long-term chemotherapy and its potential side effects. Reports also emphasize that early intervention dramatically improves survival rates, with mortality decreasing from over 80% to as low as 50% when treatment is initiated promptly. The idea is to contribute to the growing body of evidence advocating for heightened clinical awareness and timely, aggressive management to improve patient outcomes in this serious, challenging and life-threatening infection.
Declarations
Disclosure: The authors confirm that no external funding was received for any aspect of this work.
Conflicts of interest: The authors have no conflicts of interests to declare.
References
- Khiabani K, Amirzade-Iranaq MH, Ahmadi H. An Update on COVID‐19 Associated Mucormycosis Characteristics, Risk Factors, and Outcomes: A Systematic Review and Meta-Analysis. Curr Fungal Infect Rep. 2023; 17: 282-295.
- Bhambhani D, Bhambhani G, Thomas S, et al. Comparison Between Pre-COVID and Post-COVID Mucormycosis: A Systematic Review and Meta-analysis. J. Maxillofacial. Oral Surg. 2024; 23: 135-144.
- Selberg B, Edwards J Jr, Ibrahim A. Novel perspectives on mucormycosis: pathophysiology, presentation, and management. Clin Microbiol Rev. 2005; 18(3): 556-569.
- Roden MM, Zoetis TE, Buchanan WL, et al. Epidemiology and outcome of mucormycosis: a review of 929 reported cases. Clin Infect Dis. 2005; 41(5): 634-653.
- Skiada A, Pavlis I, Drogari-Apiranthitou M. Epidemiology and diagnosis of mucormycosis: An update. J Fungi (Basel). 2020; 6(4): 265.
- Gkegkes ID, Kotrogiannis I, Konstantara F, Karetsou A, Tsiplakou S, et al. Cutaneous mucormycosis by Saksenaea vasiformis: An unusual case report and review of literature. Mycopathologia. 2019; 184(1): 159-167.
- Cornely OA, Alastruey-Izquierdo A, Arenz D, et al. Global guideline for the diagnosis and management of mucormycosis: an initiative of the European Confederation of Medical Mycology in cooperation with the Mycoses Study Group Education and Research Consortium. Lancet Infect Dis. 2019; 19(12): 405-421.