
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
An interesting case of 3‘P’s – Primary Pericardial Primitive neuroectodermal tumor in an infant: A case report
Vikas Reddy Maddali1; Praveen Nagula2; Srinivas Ravi3; Krishna Mala Konda Reddy4
1 Resident in Cardiology, Department of Cardiology, Osmania General Hospital, Hyderabad, Telangana, India.
2 Assistant Professor in Cardiology, Department of Cardiology, Osmania General Hospital, Hyderabad, Telangana, India.
3Associate Professor in Cardiology, Department of Cardiology, Osmania General Hospital, Hyderabad, Telangana, India.
4Professor and Head of the Department, Department of Cardiology, Osmania General Hospital, Hyderabad, Telangana, India.
*Corresponding Author : Vikas Reddy Maddali
Resident in Cardiology, Department of Cardiology, Osmania General Hospital, Hyderabad, Telangana, India.
Email: vikasreddy04@gmail.com
Received : Feb 04, 2021
Accepted : Mar 02, 2021
Published : Mar 05, 2021
Archived : www.jcimcr.org
Copyright : © Maddali VR (2021).
Abstract
Cardiac malignancies presenting in the infancy are rare. Primitive neuroectodermal tumor (PNET), a high-grade malignant tumor is one among them. The most common sites of occurrence of primary PNET are the peripheral nervous system, bone, and deep soft tissues. It is extremely rare in the pericardium. To the best of our knowledge, only three patients with primary PNET of the pericardium have been reported so far in the literature. We report a case of primary PNET of the pericardium in a 11-months-old female child, who was referred to our hospital with complaints of dyspnea and difficulty in feeding of 5 days duration. At presentation, she had massive pericardial effusion with tamponade and an echogenic intrapericardial mass. An emergency pericardiocentesis was done to relieve the tamponade. After stabilization, the Computer tomography (CT) imaging of the chest revealed a soft tissue mass with non-enhancing cystic areas in the pericardium with features suggestive of PNET. After two days, the child had a cardiac arrest and succumbed to death.
Keywords: Cardiac malignancies, Pericardial tumor, Primitive neuroectodermal tumor, Cardiac tamponade, Pericardiocentesis.
Citation: Maddali VR, Nagula P, Ravi S, Reddy KMK. An interesting case of 3‘P’s – Primary Pericardial Primitive neuroectodermal tumor in an infant: A case report. J Clin Images Med Case Rep. 2021; 2(2): 1020.
Introduction
Primary malignant tumors of the heart and pericardium are extremely rare with a prevalence of about 0.001%-0.3% [1,2]. Among them, the primitive neuroectodermal tumors (PNET) are even more infrequent. They were first recognized by Arthur Purdy Stout in 1918 and are classified under small round cell tumors [3]. These aggressive, highly malignant tumors are thought to be derived from neuroectodermal cells through a balanced reciprocal translocation t(11;22) involving the EWSR1 (Ewing sarcoma breakpoint region 1) and FLI-1(Friend leukemia integration 1 transcription factor) genes. The most common sites of occurrence of primary tumor are in the peripheral nervous system, bone, and deep soft tissues [4,5]. Primary PNET in the pericardium is extremely rare, with only three cases reported in the literature [8-10]. We report another case of primary PNET arising in the pericardium of a 11-months-old female child.
Case report
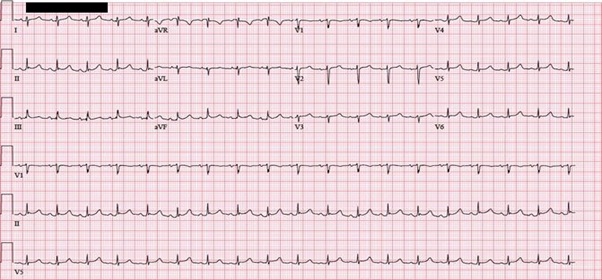
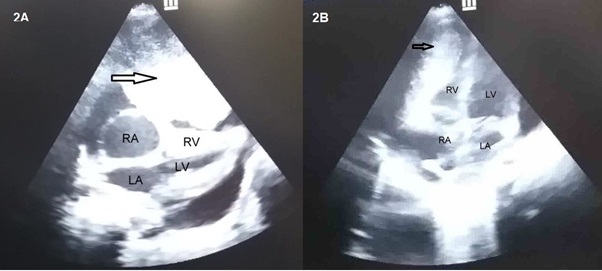
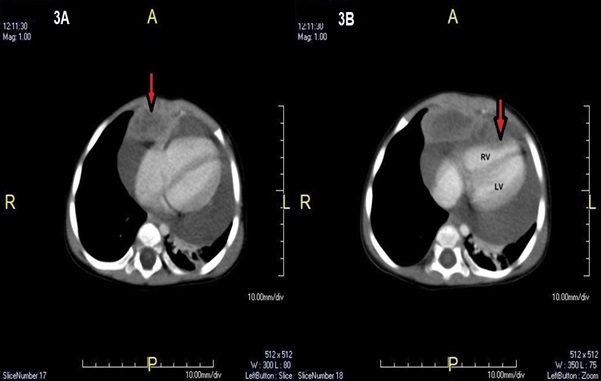
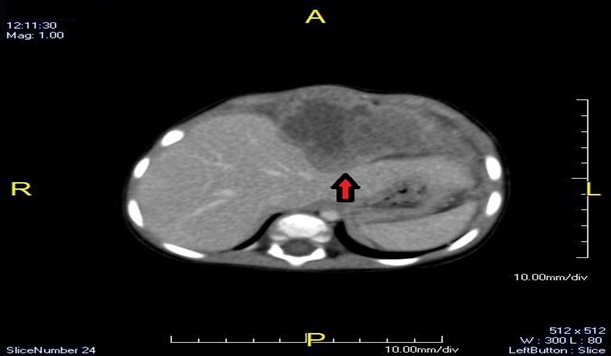
A 11-months-old female child, born at 38 weeks gestation by normal vaginal delivery with birth weight of 2.3 kg was admitted in our institute. The child presented to a local paediatrician, with complaints of breathlessness and feeding difficulty of 5 days duration. The child was then referred to our department, to rule out cardiac cause for her symptoms. She had no symptoms prior to this episode. At admission, she was dyspneic and irritable with excess sweating. On examination, there was precordial bulge and excessive intercostal retractions. The child was tachypneic and had a pulse rate of 180/min. The blood pressure recorded was 80/50 mmHg. On auscultation, muffled heart sounds were present with clear lung fields. The electrocardiogram showed sinus tachycardia with low voltage complexes (Figure 1). Bedside 2D echocardiography revealed a large pericardial collection with right atrial and right ventricular free wall collapse, suggestive of cardiac tamponade (Figure 2A). There was a large mass within the pericardium compressing the right ventricle (Figure 2B and 3B) and also indenting the left lobe of liver. Emergency Pericardial tapping for relieving tamponade was done. Approximately 350 ml of hemorrhagic pericardial fluid was aspirated and sent for analysis. The cytological examination of pericardial fluid revealed predominant lymphocytic infiltrate with reactive mesothelial cells and few atypical cells in the proteinaceous background. The Adenosine deaminase (ADA) levels were normal with no evidence of malignant cells. Computer tomography (CT) imaging of the chest revealed 85 X 71 X 58 mm well defined heterogeneously enhancing hypodense lesion arising from the pericardium (Figure 3A) noted in the antero-inferior mediastinum extending into epigastrium with non-enhancing cystic areas in the lesion. The features were suggestive of a primitive neuroectodermal tumor (PNET). The lesion was indenting the left lobe of liver (Figure 4). Large pericardial effusion was also noted. There was segmental atelectasis of the lung in the left upper lobe apico-posterior segment, and the left lower lobe lateral basal segment. Abdominal and brain CT scans were normal, with no evidence of primary tumor elsewhere. Based on the CT image findings, a provisional diagnosis of primary pericardial round cell tumor (PNET variant) has been made and the child was referred to our Cardiothoracic and vascular surgery department for the surgical resection of the tumor. Unfortunately, the next day child had a sudden cardiac arrest and expired despite several attempts of cardio-pulmonary resuscitation.
Discussion
Primary and secondary tumors of the heart are rare, and primary pericardial tumors are even more infrequent. According to the review by Meng et al. [6] and Patel et al. [7] primary pericardial tumors accounts for only 6% to 12% of all the primary tumors affecting heart. The PNET belongs to the Ewing’s sarcoma family and occurs mostly in extremities and soft tissue. Although secondary involvement of the pericardium by PNET with primary elsewhere have been reported, the primary PNET of pericardium remains exceptionally rare. To the best of our knowledge, only three cases of primary PNET of the pericardium have been reported [8-10]. Our case represents the fourth case in the English literature. The age of patients ranged from 13-51 years (average, 27.3 years), with a predilection for younger patients. In contrast to PNET of other sites, which showed male predominance, primary PNET of the pericardium appears to show female predominance (3 females and 1 male). Of these, two tumors were intra-pericardial in location as polypoid growths and presented with early clinical symptoms induced by cardiac tamponade i.e, dyspnea, chest discomfort and edema of lower extremities.
The PNET is derived from neural crest cells exhibiting neuroectodermal differentiation, as confirmed by the expression of CD99, synaptophysin, and CD56. The differential diagnoses include malignant mesothelioma, rhabdomyosarcoma and synovial sarcoma. The latter two tumors also being CD99 positive, may cause more diagnostic confusion. The PNET shows the specific t(11;22) translocation, which is not present in the other tumors.
Treatment involves a combination of chemotherapy, radiotherapy and surgery. The chemotherapy includes a standard regimen of doxorubicin, vincristine, cyclophosphamide and dactinomycin alternating with courses of ifosfamide and etoposide. Compared with surgical excision alone, its combination with chemotherapy and radiotherapy, had a better 2-year survival rate (23-44% vs 59-67%) and decrease rate of distant metastasis from (12-32% vs 46-65%) [11]. Radiotherapy is strongly recommended in surgically inoperable tumors. According to our review, among the three patients with primary PNET of the pericardium reported in the literature, two patients who received chemotherapy and underwent surgery were alive [9,10] while the other died shortly [8] after the diagnosis similar to our case. The growth pattern of PNET was related to the prognosis, the intra-pericardial polypoid growth pattern had better prognosis compared to diffuse growth pattern. However, before drawing such conclusion more cases need to be studied and followed up for further development of an effective therapeutic protocol.
Learning objectives
1. Cardiac malignancies presenting in the infancy are rare.
2. Primitive neuroectodermal tumor (PNET), a high-grade
malignant tumor commonly occurs in the peripheral nervous system, bone, and deep soft tissues. It is extremely rare in the pericardium.
3. The growth pattern of PNET was related to the prognosis, the intra-pericardial polypoid growth pattern had better prognosis compared to diffuse growth pattern.
Conclusion
Primary pericardial PNET is an exceedingly rare tumor. This report illustrates that the pericardium is a possible site for primary PNET. Despite the diagnosis of primary pericardial PNET, prognosis is dismal due to its infiltrative and invasive nature.
References
- Ostrowski S, Marcinkiewicz A, Kośmider A, Jaszewski R. Sarcomas of the heart as a difficult interdisciplinary problem. Arch Med Sci. 2014; 10: 135-148.
- Mc Allister Ha Jr. Primary tumors of the heart and pericardium. Pathol Annu. 1979; 14: 325- 355.
- Pomara G, Cappello F, Cuttano MG, Rappa F, Morelli G, Mancini P and Selli C: Primitive Neuroectodermal Tumor (PNET) of the kidney: A case report. BMC Cancer. 4: 32004.
- Hart MN, Earle KM. Primitive neuroectodermal tumors of the brain in children. Cancer. 1973; 32: 890-897.
- Besirli K, Arslan C, Tüzün H, Oz B. The primitive neuroectodermal tumor of the heart. Eur J Cardiothorac Surg. 2000; 18: 619-621.
- Meng Q, Lai H, Lima J, Tong W, Qian Y, Lai S. Echocardiographic and pathologic characteristics of primary cardiac tumors: a study of 149 cases. Int J Cardiol. 2002; 84: 69-75.
- Patel J, Sheppard MN. Pathological study of primary cardiac and pericardial tumours in a specialist UK centre: surgical and autopsy series. Cardiovasc Pathol 2010; 19: 343-352.
- Mohandas KM, Chinoy RF, Merchant NH, Lotliker RG, Desai PB. Malignant small cell tumour (Askin-Rosai) of the pericardium. Postgrad Med J 1992; 68: 140-142.
- Azribi F, Razak AR, Bough G, Lee D, Rowe D, Bown N, Dildey P, Clark S, Plummer R. Extraosseous pericardial Ewing’s sarcoma. J Clin Oncol 2010; 28: e48-50.
- Zhenwei Chen, Rongming Chen, Chising Ng, Hongqi Shi. Primary pericardial primitive neuroectodermal tumor: A case report and review of literature. Int J Clin Exp Pathol. 2018; 11(4): 2155-2159.
- Saeedinia S, Nouri M, Alimohammadi M, Moradi H, Amirjamshidi A. Primary spinal extradural Ewing’s sarcoma (primitive neuroectodermal tumor): Report of a case and meta-analysis of the reported cases in the literature. Surg Neurol Int. 2012; 3: 55.