
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Role of pectoralis major flap in resource limited settings (developing world): A case report of huge neck cancer done in Tanzania
Victor Mashamba1*; Shaban Mawala2; Emmerenceana Mahulu3; Ashfaq Abdulshakoor4; Amina Hassan4; Aron Kiberiti4; Joyce Kasongwa4; Sadick Sizya5; Angela mwakimonga6
1Consultant surgeon, Head and Neck unit, Department of Otorhinolaryngology, Muhimbili National Hospital, Dar es Salaam-Tanzania.
2General ENT surgeon, Department of Otorhinolaryngology, Muhimbili National Hospital, Dar es Salaam-Tanzania.
3General ENT surgeon, Department of Otorhinolaryngology, Sokoine regional Hospital, Lindi, Tanzania.
4Resident Department of Otorhinolaryngology, Muhimbili University of Health and Allied Sciences 65001, Dar es Salaam-Tanzania.
5Registrar, Department of Otorhinolaryngology, Muhimbili National Hospital, Dar es Salaam-Tanzania.
6Consultant pathologist, Department of pathology, Muhimbili University of Health & Allied Sciences, 65001, Dar es Salaam-Tanzania.
*Corresponding Author : Victor Mashamba
Consultant surgeon, Head and Neck Unit, Department
of Otorhinolaryngology, Muhimbili National Hospital,
Dar es Salaam-Tanzania.
Email: victor_mashamba@yahoo.com
Received : Feb 12, 2021
Accepted : Mar 26, 2021
Published : Mar 30, 2021
Archived : www.jcimcr.org
Copyright : © Mashamba V (2021).
Abstract
Skin cancers are common in head and neck region particularly Basal cell carcinoma and Squamous cell carcinoma. Treatment options includes wide local excision with neck dissection followed by adjuvant radiation/chemo/chemoradiation. We report a case of a huge skin cancer of the neck about 8.5 cm in its greatest dimensions and reconstructive techniques of the defect using pectoralis major flap in a 61-years old Albino patient, what’s important is good understanding of anatomy and surgical land marks to identify the thoracoacromial artery which is the main feeder to the flap. Reconstruction was successful with acceptable morbidity and the patient was sent for chemoradiation with no reported recurrence. Presentation from this case demonstrates that the pectoralis major flap still remains the ‘workhorse’ of reconstruction in Tanzania. It is advocated to be used in resource limited countries, effectively with acceptable morbidity and results.
Keywords: Squamous cell carcinoma, Pectoralis major flap, Neck dissection, Squamous cell carcinoma (SCC), Wide local excision (WLE), Thoracoacromial artery, Muhimbili.
Citation: Mashamba V, Mawala S, Mahulu E, Abdulshakoor A, Hassan A, et al. Role of pectoralis major flap in resource limited settings (developing world): A case report of huge neck cancer done in Tanzania. J Clin Images Med Case Rep. 2021; 2(2): 1036.
Introduction
The majority of skin cancers of the head and neck are nonmelanoma skin cancers (NMSC). Basal cell carcinoma and squamous cell carcinoma are the most frequent types of NMSC. Various options for treatment of skin cancer are available to the patient and physician, allowing high cure rates and excellent functional and cosmetic outcomes. Sunscreen protection and early evaluation of suspicious areas remain the first line of defense against skin cancers [1]. Treatment options including wide local excision, Mohs surgery, sentinel lymph node biopsy, and cervical lymphadenectomy and adjuvant radiation when warranted offer a high cure rate, while balancing excellent functional and cosmetic outcomes [2]. Free flap surgery is a routine procedure in many developed countries for reconstruction of head and neck defects with good surgical outcomes. In many developing countries, however, these services are not available due to lack of expertise of free flaps [3].
Reconstruction of oncosurgical defects in the head and neck region presents a challenge due to the complex anatomy and functional demands of this region. Nowadays, microvascular free flaps are considered the gold standard for reconstruction, whereas pedicled flaps are commonly utilized as a salvage procedure [4]. The limitations, however, of microvascular reconstruction techniques lie in the fact that the expertise and facilities for this specialized surgery are not available at many centers; the procedure is costly; and operating time is greatly increased which entails higher anesthetic risk for critically ill patients [5].
In contrast, the pectoralis major myocutaneous (PMMC) flap is still considered the ‘work horse of pedicled flaps’ for head and neck reconstruction, since its description by Ariyan in 1979 [6], and it still remains popular in developing countries around the globe [7]. The advantages of this flap are excellent vascularity, proximity to the head and neck region, simplicity of harvesting, and its bulk, all of which have benefits for covering vital structures of neck [8]. The pectoralis major flap comprises the pectoralis major muscle, with or without overlying skin. It has an axial blood supply and is based superiorly on the pectoral branch of the thoracoacromial artery. It is very useful in the head and neck, and can inter alia be used for reconstructions of soft tissue defects of the oropharynx, oral cavity, hypopharynx, and skin of the neck; to augment pharyngeal repairs following salvage laryngectomy following previous chemoradiotherapy; and to cover carotid or jugular vein blowouts etc. [9].
There is no single case reported of head and neck reconstruction using a pectoralis major flap in Tanzania and to the best of our knowledge, this is the only documented case in Tanzania. We report a case of a huge skin cancer of the neck and reconstructive techniques of the defect using pectoralis major flap in a 61-years old Albino patient.
Case report
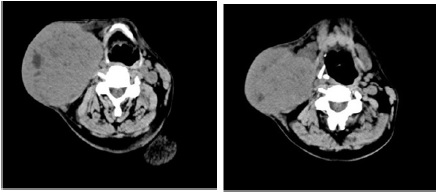
A 61-year old male, Albino patient presented to our department complaining of a painless swelling on the right side of the neck for the past 3 months. The mass had been growing insidiously. There was no history of fever, excessive night sweats or throat symptoms, and there was no history of prior head and/ or neck irradiation, chewing tobacco or alcohol consumption. He was married to two wives, both Albinos. On examination there was a huge mass on the right side of the neck involving levels II to IV, but with no airway compromise or difficulty in swallowing. The mass was nodular and non-tender, slightly mobile and the overlying skin was tense with areas of ulceration with contact bleeding. The mass measured 8.5 cm in its greatest dimension (Figure1). No palpable regional lymph nodes were noted. Fibreoptic nasolaryngoscopy examination was normal. Computerized tomography scan showed a large right neck mass with areas of calcification and necrosis involving the sternocleidomastoid muscle and compressing the carotid sheath medially (Figure 2). The patient was planned for surgery after preoperative work up. Informed consent was obtained from the patient for surgery and to use his images for the purpose of this report.
Surgical technique
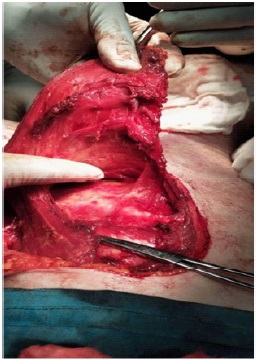
The patient was placed in a supine position with the chest exposed. The operation was done under general anesthesia without muscle relaxation. Wide local excision of the primary mass (at least 1 cm wide tumor margin) was done which was followed by ipsilateral radical neck dissection (Figures 3 & 4).
Surface Marking (Pectoralis major flap)
The vascular axis of the pectoral branch of the thoracoacromial artery was drawn on the chest wall as a line that descends perpendicularly from the middle of the clavicle and then bends and follows an imaginary line from acromion toward xiphisternum (Figure 5). The size, shape, and location of the skin paddle were determined by the size, shape of the surgical defect, and its distance from the midclavicular point of the flap. A skin island was drawn according to the size and shape of the surgical defect.
Flap elevation
Skin was incised around the skin paddle. An incision was extended laterally along the anterior axillary fold and dissection was extended onto the surface of the pectoralis major muscle (Figure 6). The skin above the skin paddle was then widely elevated from the pectoralis major muscle with cautery up to the clavicle (Figure 7). The pectoralis major muscle was then incised alongside the sternum with cautery and dissected from the ribs and intercostal muscles. Dissection along the lateral border of the pectoralis major muscle was done and the dissection plane between the pectoralis minor and major muscles and the vascular pedicle was found. Finger dissection towards the clavicle was done in this intermuscular plane so that the pectoralis major and its vascular pedicle (pectoral branch of thoracoacromial artery) were freed from the pectoralis minor (Figure 8). The pectoralis major muscle was then divided lateral to the pedicle while keeping the pedicle in view, thereby freeing it from the humerus. The pectoralis major muscle was then freed. The flap was then passed into the neck superficial to the clavicle through a wide subcutaneous tunnel and inspection was done to make sure that the vascular pedicle was not twisted (Figure 9). Adequate length of the flap was obtained through passing the flap above the clavicle. The recipient site was closed with minimal skin tension (Figure 10). The donor site was closed primarily and a drain inserted.










Discussion
Some authors have described their experience of patients treated with pectoralis major flap, and the vast majority reported only minor complications that did not require second procedures for correction: orocutaneous fistulas (16.5%), suture line dehiscence (12%), neck wound complications (11%), and donor site complications (1.3%) [10]. In this single case which was done in Tanzania, no any complication occurred, and sutures were removed after 7 days of surgery
For this case, basic surgical instruments were used. Raising a pectoralis major just requires a knife, forceps and retractors as surgical instrumentation, a few hours of operative time, and short training time [11]. What’s important is a good understanding of the anatomy and surgical landmarks to identify the thoracoacromial artery which is the main feeder to the flap. Care was taken not to twist the artery when passing the flap through the tunnel over the clavicle into the neck.
For the above reasons, pectoralis major should be a workhorse for head and neck reconstruction in Tanzania. Some authors state that the most important benefit of pectoralis flap is flap survival. Total microvascular flap loss may be seen even in the hands of skilled surgeons, but total pectoralis flap failure is very rare even in inexperienced hands, due to its dependable vascularity and its shorter procedural learning curve [13].
In the developed countries, with the advent of increased knowledge, clinical skills and availability of better infrastructure, free flap reconstruction remains the gold standard and the first choice of reconstruction of the head and neck surgeon. Pectoralis major flaps, however, are kept reserved for salvage of failures of free flaps, compromised patients, or are planned as soft tissue fillers in combination with free flaps [12]. However, in Tanzania, due to lack of necessary training and exposure to free flap surgical procedures; inadequate armamentarium; higher patient load; and economic realities, such reconstructions though desirable, are not always possible.
Conclusion
This case demonstrates that the pectoralis major flap should remain the ‘workhorse’ of reconstruction in Tanzania. It is advocated to be used in developing countries, such as ours, and can be used effectively with acceptable morbidity and with good results. Good understanding of anatomy and surgical know how is crucial when harvesting this flap. Even in this era of free flap dominance, reconstruction using pectoralis major flaps is here to stay.
References
- Ouyang Y et al. Semin Plast Surg. Skin cancer of the head and neck. 2010; 24(2): 117-26.
- Mydlarz WK, Weber RS et.al Surg Oncol Clin N Am., Cutaneous malignancy of the head and neck. 2015; 24(3): 593-613.
- Nangole WF, et al. Free Flaps in a Resource Constrained Environment: A Five-Year Experience—Outcomes and Lessons Learned. Plastic Surgery International. 2015; 194174: 6 pages.
- Novakovic D, Patel RS, et al. Salvage of failed free flaps used in head and neck reconstruction. Head Neck Oncol. 2009; 1: 33.
- Chaudhary R, Akhtar MS, et al. Use of pectoralis major myocutaneous flap for resurfacing the soft tissue defects of head and neck. J Orofac Sci. 2014; 6: 88–93.
- Ariyan S, et al. The pectoralis major myocutaneous flap. A versatile flap for reconstruction in the head and neck. PlastReconstr Surg. 1979; 63: 73–81.
- Pinto FR, Malena CR, et al. Pectoralis major myocutaneous flaps for head and neck reconstruction: factors influencing occurrences of complications and the final outcome. Sao Paulo Med J. 2010; 128: 336–341.
- Leite AKN, de Matos LL, et al. Pectoralis major myocutaneous flap for head and neck reconstruction: Risk factors for fistula formation. Acta Otorhinolaryngol Ital. 2014; 34: 389–393.
- Fagan JJ. The Open Access Atlas of Otolaryngology, Head & Neck Operative Surgery. Pectoralis major flap.( https://vula.uct.ac.za/ access/content/.../Pectoralis%20major%20flap-1.pdf)
- Mehrhof AI, Rosenstock A, et al. The pectoralis major myocutaneous flap in head and neck reconstruction. Analysis of complications. Am J Surg. 1983; 146: 478-82.
- Gadre KS, Gadre P, et al. Pectoralis major myocutaneous flap-still a workhorse for maxillofacial reconstruction in developing countries. J Oral Maxillofac Surg. 2013; 71: 2005.
- Saito A, Minakawa H, et al. Indications and outcomes for pedicled pectoralis major myocutaneous flaps at a primary microvascular head and neck reconstructive center. Mod Plast Surg. 2012; 2: 103–107.