
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Re-plantation of avulsed permanent incisor after 4 days of trauma
Haya Alomari; Chaza Kouchaji*
Department of Pedodontics, Damascus University, Syria.
*Corresponding Author : Chaza Kouchaji
Faculty of Dental Medicine, Department of Pedodontics, Damascus University, Syria.
Email: Chaza.kouchaje@damascusuniversity.edu.sy
Received : Feb 26, 2021
Accepted : Apr 07, 2021
Published : Apr 09, 2021
Archived : www.jcimcr.org
Copyright : © Kouchaji C (2021).
Abstract
Tooth avulsion in children and adolescents demands urgent treatment to enhance the chances of successful re-implantation. This case report describes the treatment of an 11-year-old girl who suffered an avulsion of the maxillary right central incisor followed by delayed re-implantation after the tooth was stored in a dry medium for 4 days. Although the tooth was kept in unfavorable conditions, tooth reimplantation was done because the patient was young and it was advantageous to avoid psychological harm as well as esthetic and functional issues.
Keywords: Re-Plantation; Avulsed permanent incisor; 4 Days; Trauma.
Citation: Alomari H, Kouchaji C. Re-plantation of avulsed permanent incisor after 4 days of trauma. J Clin Images Med Case Rep. 2021; 2(2): 1046.
Introduction
Tooth avulsion is a complete displacement of a tooth from its socket and is seen in about 0.5-3% of dental injuries [1-3]. Avulsion cases in children increases between the ages of 7 and 9 years due to the immaturity of roots in addition to the low resistance of the alveolar bone/Periodontal Ligament (PDL) against extrusive forces during the eruption period of the teeth [1,3].
The cause of avulsion depends on the type of dentition. Avulsion in primary teeth is usually due to the hitting of hard objects with the teeth, while avulsion in permanent teeth is generally caused from falls, sports, fights, or child abuse [4-5].
In both types of dentition, avulsion usually happens in maxilla, and the most avulsed teeth are the maxillary central incisors. Increased overjet and incompetent lips are potential etiological factors in such avulsion cases [2,4,6]. In spite of the fact that avulsion usually involves one tooth, there have been cases reported tooth-supporting tissue injuries, lip injuries, and multiple avulsions [7,8].
The main goal in treating an avulsed tooth is to conserve and treat the supporting tooth tissues and to replant the avulsed teeth in its socket. The success rate of this operation relys on the patient’s general health, maturity of the root, the time the tooth is out of its socket, and storage medium [9-11]. The period of extra-oral time and the storage medium have the most definitive effect on the PDL cells’ status [10,11]. The goal of this case report was to exhibit a case of a delayed replantation of avulsed maxillary central incisor after an extended dry extra-alveolar period.
Case report
A 11-year-old girl was referred to the department of Pediatric Dentistry, Faculty of Dentistry Damascus University, Syria, after a stairs fall. The avulsed tooth was not placed in any storage medium and was brought to the university dry after 4 days of the accident.
The patient’s parents reported that the child has no systemic diseases. On examination, no extra-oral injury was detected. The intraoral examination revealed that the maxillary right permanent central incisor (Tooth 11) was avulsed. The left central incisor (Tooth 21) showed enamel-dentin cracking, fracture and mild intrusion. The patient had permanent dentition and her oral hygiene was fair.
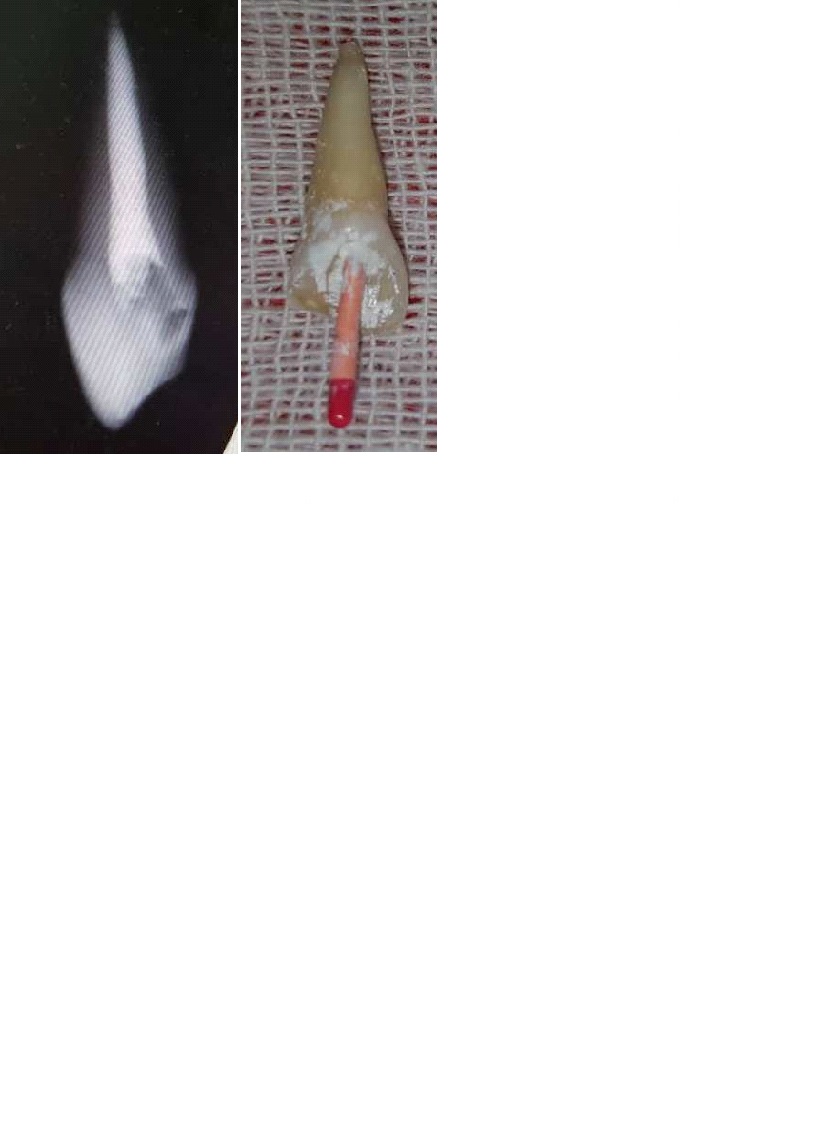
Periapical radiographs showed no alveolar bone fracture. Examination of the avulsed tooth revealed that the crown had an enamel-dentin fracture and that the root had a nearly closed apex. The tooth was washed with saline and water.

Root canal treatment was completed extra-orally, and the root filling was done with Gutta Percha (Figure 2).
Then the PDL was removed (in order to slow down the ankylotic process) by gentle scaling and gauze (Figure 3).

Local anesthetic was administered, after irrigating with saline, blood was induced in the empty socket.
The tooth was replanted using light pressure for about 10 minutes. The teeth were splinted from canine to canine (9 mm round orthodontic wire) (Figure 4).

Oral hygiene instructions and information about having a soft diet and the necessity to rinse with a chlorhexidine during the fixation period were provided. In addition to describing prophylactic antibiotic with amoxicillin at a dose of 625 mg/day. The parents were told to return regularly for clinical and radiographic follow-up. The patient was reviewed after two weeks, there was a clear gingival healing and no radiological evidence of pathological changes was detected. The patient was seen again four weeks after, and the splinting wire was removed at this appointment.
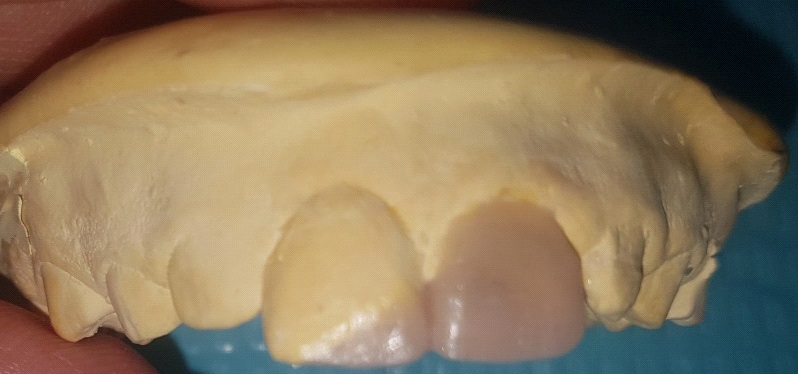
The teeth were restored with a Composite Resin restoration (3m Dentin, Ivoclar Enamel shade A2) (Figure 5) after making a silicone guide (Figure 5) for better shaping.

The case is still under observation and reviewing.
Discussion
The guidelines for the treatment of avulsed permanent teeth differ, but all the guidelines agree that the ideal approach for an avulsed tooth is immediate replantation [3,4].
The treatment decision of an avulsed teeth depends on the maturity of the root apex (open or closed) and the status of the PDL cells which is related on the storage medium and the extra-oral period of time [9,10,12,13]. The time crucially influences the results and has a direct relation with the survival of PDL cells. Clinical studies have indicated that teeth replanted within 5 minutes after avulsion have the best prognosis [14].
After a 60 minutes or more of dry time, all PDL cells are Nonviable [3,4]. The storage and transport media during the extra-oral time are also of critical importance. The tooth should be kept in a convenient media, such as saline, milk, HBSS or saliva until it is replanted by a dentist when the extra-oral time is prolonged, [15,16].
In the present case, the teeth were kept in dry piece of paper, and the extra-oral dry time was more than 60 minutes (4 days). If the tooth has been dry for more than 60 min before replantation, it is indicated that the RCT may be done extra-orally before replantation or later. Because there were no chances of obtaining pulp space revascularization and the periodontal ligament will be necrotic and not expected to heal, it was decided to treat the root canals extra-orally.
Depending on the traumatology guidelines and articles on delayed replantation cases, PDL cells will be necrotic following delayed replantation, resulting in a poor long-term prognosis [1,3,4,17].
Replanted teeth should be followed-up carefully and clinical/ radiographical findings should be kept. Ankylosis is frequently associated with infraposition of the replanted tooth. The replanted teeth of this case showed signs of ankylosis.
Conclusion
Despite an extended extra-alveolar dry storage time, teeth with delayed replantation may be retained in a constant and functional position in mouth. In patients for whom growth has not stopped, using the replanted tooth to maintain the supporting bone for some years until implant is applicable and can be considered a suitable therapeutic option.
References
- Andreasen JO, Andreasen FM. Classification, etiology and epidemiology, in Textbook and Color Atlas of Traumatic Injuries to the Teeth, pp, Mosby, Munksgard, Copenhagen, Denmark. 1994; 151-179.
- Andreasen JO, Andreasen FM, Examination and diagnosis of dental injuries, in Textbook and Color Atlas of Traumatic Injuries to the Teeth, Mosby, Copenhagen, Denmark. 1994; 195-217.
- Andreasen JO, Andreasen FM, Day P, et al. International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: Avulsion of permanent teeth. Dental Traumatology. 2012; 28: 88–96.
- Kaba AD, Maréchaux SC. A fourteen-year follow-up study of traumatic injuries to the permanent dentition. ASDC Journal of Dentistry for Children. 1989; 56: 417–425.
- Andreasen JO. Etiology and pathogenesis of traumatic dental injuries. A clinical study of 1,298 cases. Scandinavian Journal of Dental Research. 1970; 78: 329–342.
- Brin I, Ben-Bassat Y, Heling I, Brezniak N. Profile of an orthodontic patient at risk of dental trauma. Dental Traumatology. 2000; 16: 111–115.
- Filippi A, Pohl Y, Kirschner H, Replantation of avulsed primary anterior teeth. Treatment and limitations. Journal of Dentistry for Children. 1997; 64: 272–275.
- Andreasen JO, Andreasen FM, Essentials of Traumatic Injuries to the Teeth. A Step-By-Step Treatment Guide, Munksgaard, Conpenhagen, Denmark, 2nd edition. 2001.
- Andreasen JO, Andreasen FM. Avulsions in Textbook and Color Atlas of Traumatic Injuries to the Teeth. Eds. Mosby, Munksgard, Copenhagen, Denmark. 1994; 383-425.
- Cohenca N, Karni S, Eidlitz D, Nuni E, Mosho Nov J. New treatment protocols for avulsed teeth. Refuat Hapeh Vehashinayim. 2004; 21: 48–53.
- Andreasen JO. Effect of extra-alveolar period and storage media upon periodontal and pulpal healing after replantation of mature permanent incisors in monkeys. International Journal of Oral Surgery. 1981; 10: 43–53.
- Ram D, Cohenca ON. Therapeutic protocols for avulsed permanent teeth. Review and clinical update. Pediatric Dentistry. 2004; 26: 251–255.
- Andreasen JO, Borum MK, Andreasen FM. Replantation of 400 avulsed permanent incisors. 3. Factors related to root growth,” Endodontics & Dental Traumatology. 1995; 11: 69–75.
- Andersson L, Bodin I. Avulsed human teeth replanted within 15 minutes - A long-term clinical follow-up study. Dental Traumatology. 1990; 6: 37–42.
- Barrett EJ, Kenny DJ. Avulsed permanent teeth: A review of the literature and treatment guidelines. Endodontics and Dental Traumatology. 1997; 13: 153–163.
- Pohl Y, Filippi A, Kirschner H. Results after replantation of avulsed permanent teeth. II. Periodontal healing and the role of physiologic storage and antiresorptive-regenerative therapy. Dental Traumatology. 2005; 21: 93–101.
- Patel S, Dumsha TC, Sydiskis RJ. Determining Periodontal Ligament (PDL) cell vitality from exarticulated teeth stored in saline or milk using fluorescein diacetate. International Endodontic Journal. 1994; 27: 1–5.