
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Primary strumal carcinoid tumor of the ovary arising from a heterochronous struma ovarii in young female patient
Kuang-Ting Liu1,2; Yueh-Ching Chang1,2; Yu-Chieh Lin1,3; Junn-Liang Chang1,3,4*
1 Department of Pathology and Laboratory Medicine, Taoyuan Armed Forces General Hospital, Taoyuan City, Taiwan, R.O.C.
2 Hsin Sheng Junior College of Medical Care and Management, Taoyuan City, Taiwan, R.O.C.
3 Department of Pathology, Tri-Service General Hospital, Teipai City, Taiwan, R.O.C.
4 Department of Biomedical Engineering, Ming Chuan University, Taipei, Taiwan, R.O.C.
*Corresponding Author : Junn-Liang Chang
Department of Pathology and Laboratory Medicine, Taoyuan Armed Forces General Hospital,
32551, No. 168, Chung-Shing Rd, Long-Tang
District, Taoyuan City, Taiwan, R.O.C.
Email: junn9liang@yahoo.com.tw
Received : Mar 11, 2021
Accepted : Apr 16, 2021
Published : Apr 21, 2021
Archived : www.jcimcr.org
Copyright : © Chang JL (2021).
Abstract
Primary ovarian carcinoid tumors are extremely rare. Ovarian strumal carcinoid is usually derived from mature cystic teratoma, an ovarian germ cell tumor composed of two distinctive components characteristic thyroid tissue intermixed with a carcinoid tumor. The incidence of stromal carcinoid tumor is accounting for 0.3-1% of all ovarian tumors and 3% of all mature teratomas. Herein, we report a 25-year-old female presented with severe abdominal pain. She had right struma ovarii after Laparoscopic-Assisted Ovarian Cystectomy (LAOC) procedure one year ago. The sonography of abdomen images study demonstrated a well capsulated cystic mass measured up to 11 cm in dimension. The mature cystic teratoma was the first diagnostic possibility. She underwent the laparoscopy-assisted left ovarian cystectomy. Histopathological and immunohistochemical examinations confirmed strumal Carcinoid Tumor of the Ovary (SCTO) arising from strum ovarii in the left ovary. She was recovered well and was still asymptomatic after two years follow-up. In conclusion, we first describe the primary SCTO arising from a heterochronous struma ovarii. The symptoms of SCTO are usually non-specific and misleading. Therefore, it is important to fully understand the characteristics, diagnosis and management of SCTO. Diagnosis should be confirmed by pathology and immunohistochemistry, and clinically metastatic carcinoid should be excluded.
Keywords: Struma ovarii; Strumal carcinoid tumor; Germ cell tumor; Mature cystic teratoma; Immunohistochemistry.
Citation: Liu KT, Chang YC, Lin YC, Chang JL. Primary strumal carcinoid tumor of the ovary arising from a heterochronous struma ovarii in young female patient. J Clin Images Med Case Rep. 2021; 2(2): 1057.
Introduction
Mature Cystic Teratomas (MCT) or dermoid cyst constitute 10-20% of all ovarian tumors. Primary ovarian carcinoids are uncommon, accounting for 0.3% of all carcinoid tumors and the majority of them are associated with MCT [1,2]. Ovarian struma is a very rare and represent 0.3-1% incidence of all ovarian neoplasms and 3% of mature teratomas. Strumal carcinoid is an extraordinary rare kind of ovarian tumor consisting of thyroid tissue intermixed with neuroendocrine tumor component. Strumal carcinoid of the ovary is belongs to the group of monodermal teratomas, a type of germ-cell tumor characterized by an intimate mixture of thyroid tissue and carcinoid [1]. Ovarian carcinoid tumors are very rare, less than 0.1% of all ovarian cancers [2-4]. The symptoms of SCTO are usually non-specific and misleading. Therefore, it is important to fully understand the characteristics, diagnosis and treatment of SCTO. Primary SCTOs are usually unilateral, confined to the ovaries, and metastasis histologically indistinguishable [3-5]. Diagnosis should be confirmed by immunohistochemistry, and secondary carcinoid should be excluded. We report an unusual case of SCTO with heterochronous mature cystic teratoma and strumal carcinoid tumor from one of two ovarian mature cystic teratomas in young female patient.
Case presentation
A 25-year-old female presented with severe abdominal pain, especially over the LLQ region since this midnight. She was parity 1011 of history. Gynecological and obstetrical history: Menarche at age 12 years with regular menstrual cycles. She had struma ovarii accompanied by mature cystic teratoma of the right ovary after LAOC procedure one year ago. The vital signs showed stable. Physical examination showed abdomen revealed ovoid in shape, a palpable mass about 12 cm over the lower abdomen with moderate tenderness. Her extremities and the neurological examination was essential negative. Her past and medical history was unremarkable.
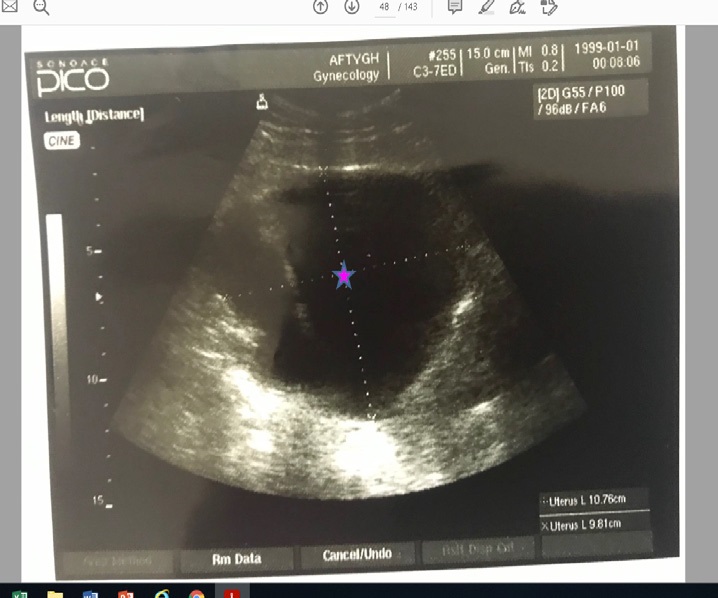
The chest-x ray film showed no abnormal finding. The pelvic ultrasonography images study demonstrated a well capsulated cystic mass with hypoechoic with a thin hypointense capsule with well-defined borders and fat-like signal intensity, a focal heterogenously enhancing content measured up to 11cm in dimension as shown in Figure 1, and a few of fluid collection in the cul-de-sac, which impresses of mature cystic teratoma was the first diagnostic possibility. The right ovary is not seen. The laboratory analysis showed within normal limits included blood routine, biochemistry and negative for tumor markers CA125, CA19.9, and negative for pregnancy test. Prior to surgery, a hormonal analysis of the thyroid function was performed, the result of which was within normal limits. She underwent the laparoscopy-assisted left ovarian cystectomy after 2nd admitted two days at our hospital. She recovered well and was discharged on the 5th post-operative day with no any complications.
Histopathological findings
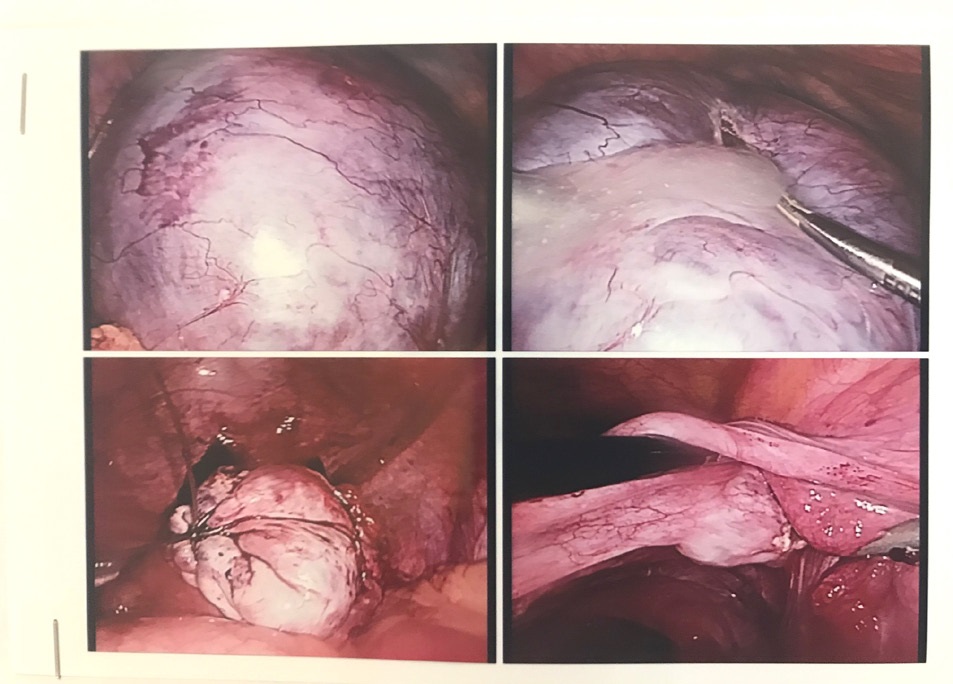
On gross examination, a yellowish brown left ovarian tumor was 10 by 5 by 2 cm, with vague nodularity as intra-operative finding as shown in Figure 2. The cut sections exhibited wellencapsulated solid mass was predominantly solid mass with two cystic areas filled with skin appendages and a tuft of hair.
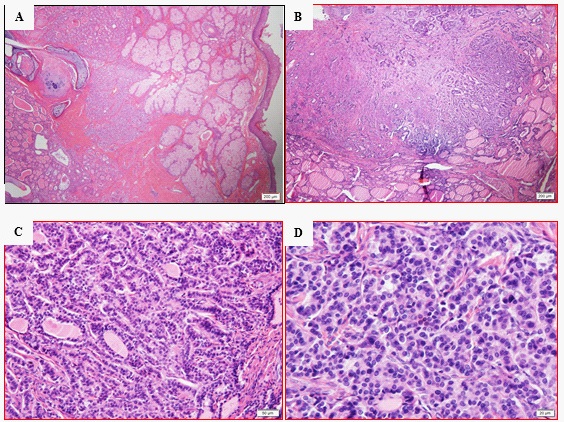
Morphologically, total sections of ovarian tumor composed of two distinct components as shown in Figure 3A-D. Demonstrated a part of the mature cystic teratoma (dermoid cyst), a cyst lined by stratified squamous epithelium with skin appendages contained skin appendage, cartilage and bony fragments, and demonstrated features of struma ovarii consisted of the thyroid tissue with adenomatous change with follicular adenoma such as embryonal, acinar, micro- and macro-follicular patterns, colloid content. In additional, a component of carcinoid tumor integrated by polygonal cells with light and eosinophilic, cytoplasm with rounded nuclei with mild pleomorphism and exhibited a trabecular, insular, acinar pattern resembling welldifferentiated neuroendocrine tumors of other origins. No capsular or vascular invasion or mitotic figure was identified.
Immunohistochemical examination as shown in Figure 4AD, these tumor cells revealed diffusely positively immunoreactivity for pan-CK, TTF1, CK7, galectin-3, NSE (neuron specific enolase) and S-100 protein stains, chromogranin, synaptophysin, insulinoma-associated protein 1 (INSM1) and focally CEA. No elevated proliferating labeling Ki-67 index (less than 5%), and negative for CK20. Pathological and immunohistochemical examinations confirmed Strumal Carcinoid Tumor of the Ovary (SCTO) arising from struma ovarii of the left ovary. The patient recovered well with no obvious complications and was discharged on the 3rd day post-surgery. Taken together, following resection of the bilateral ovarian masses histopathological and immunohistochemical analysis illustrated the pathological diagnosis of struma ovarii in the right ovary accompanied by the other stromal carcinoid tumor in the left ovary. Patient recovered well and was still asymptomatic or tumor recurrence identified after two years of follow-up.
Discussion
Ovarian Strumal Carcinoid (OSC) is an ovarian germ cell tumor composed of thyroid tissue mixed with a carcinoid tumor [1,2]. The incidence of this type of tumor is around 0.3-1% of all ovarian tumors and 3% of all mature teratomas [3-5]. The OSC frequently arises from mature cystic teratomas, which are the most common benign germ cell tumor in women, accounting for 58%, and between 27-44% of all ovarian tumors, including benign and malignant [5-6].
Struma ovarii is a rare ovarian benign tumor, classified as single layer ovarian teratoma by the WHO classification [7]. Pathologically, all or the majority of the tumor tissue was a particular type of mature teratoma, which was composed of thyroid tissue [4,7,8-10]. Strumal carcinoid of the ovary is an unusual form of ovarian teratoma composed of an intimate mixture of thyroid and carcinoid tissues [1-4].
Ovarian carcinoid tumors were first two ovarian carcinoid were reported by Stewart et al. in 1939 [11]. Ovarian carcinoid tumors may be present as primary or metastatic. Differentiation diagnosis is always difficult. However, if bilateral or peritoneal deposition, when lack of teratoma elements, and lymphovascular invasion are signs of metastatic carcinoid. We report a primary strumal carcinoid tumor of the ovary arising from a heterochronous struma ovarian in young woman in present case.
Carcinoid tumors in ovarian and testicular teratomas are considered to be neuroendocrine cells derived from the epithelium of the gastrointestinal or respiratory tract. Carcinoid tumors can be studied in the ovaries as a primary tumor with metastasis in the gastrointestinal tract or other locations. And with mature cystic teratoma or a primary pure tumor as the components of the organ.
Strumal Carcinoid of the Ovary (SCTO) is a rare monodermal germ cell tumor, compose of the components teratoma histomorphologic ally characterized by an innimate mixture of thyroid tissue contains less than 50% and admixtures neuroendocrine tumor (carcinoid) tissue [11-13].
SCTO estimates for about 2% of Mature Cystic Teratoma (MCT), and are most common in the age of 50 to 60 years. Primary ovarian carcinoids account less than 1% of all carcinoid tumors, and constitute less than 0.1% of all ovarian tumors [1,2,10,15]. Primary ovarian carcinoid tumors are common unilateral, confined to the ovaries, and has no histological metastasis.
Histological classification, according to WHO [3,8], there are divided into four distinctive types include insular, trabecular, mucinous, stromal carcinoid and mixed (insular and trabecular). Insular carcinoid is the most common type about 50%. One third of cases present clinical as related to carcinoid syndrome [12-14].
Primary ovarian strumal carcinoid tumor is rarely and is considered as a borderline malignant tumor. Most the SCTOs are commonly found in perimenopausal or post-menopausal women, usually presenting with ovarian heterogeneous mass, or as an incidental finding clinically. The age of presentation varies between 21 and 77 years old similar to our case. These tumors can vary in size, up to 26 cm or larger [1,2]. The SCTOs are usually unilateral as in our case, although, there are bilateral cases described. In 10% of cases, the contralateral ovary contains another tumor, usually a mature cystic teratoma (dermoid cyst) or struma ovarii as in our present case. Sixty percent of strumal carcinoids show within dermoid cysts or solid mature teratomas. The average survival time of 14 years in primary, and metastatic median survival time was about 6 years. In previous studies, carcinoid tumors manifest variable clinical behaviour especially abdominal pain as present case. The majority of SCTO may associate with carcinoid syndrome, the clinical symptoms such as, cutaneous flushing, diarrhea, bronchoconstruction and right-sided cardiac valve disease [15-18], however, there no presented in our case.
The strumal carcinoid arising in one mature cystic teratoma is similar to carcinoids found elsewhere as our case. The differential diagnosis include metastatic thyroid carcinoma to the ovary, ovarian clear cell carcinoma, sex cord stromal tumor , melanoma, struma ovarii in matrue teratoma or cystic struma ovarii, mature cystic teratoma, etc. The nuclear features of neuroendocrine tumors characteristics as salt and pepper chromatin may be indicated, but can also be detected in follicular cells of strumal carcinoids.
The morphological features of SCTO is consisted of two distinct components. Immunomhistochemically [19], neoplastic thyroid-like tissue intermixed with tumor areas show classical features of neuroendocrine tumors, displays struma ovarii with a thyroid follicle-like structure with positive for Thyroid Transcription Factor 1 (TTF1), thyroglobulin, CD56, CK 19 [17- 19], and negative for Hector Battifora and Mesothelioma 1 (HBME1), and a neuroendocrine cell component with a trabecular arrangement and island growth with definitly positive for insulinoma-associated protein 1 (INSM1), synaptophysin, chromogranin, CD56, and CK7 negative.
Primary carcinoid tumors arising in mature teratomas are tumors with low malignancy potential in most cases [1-4,7,15- 18]. Recently, an attempt is made to recognize the surgical aggressiveness by evaluation of the patient’s age. Previously, the carcinoid component of the strumal carcinoid has been suggested a malignant transformation of struma ovarii. However, it is almost always benignant behavior clinically, and management with a simple oophorectomy or salpingo-oophorectomy and carry good prognosis. The overall 5-year survival rate for patients with carcinoids regardless of location is 44-56% [18]. The presence of regional and distant metastases are associated with a worsening in the prognosis. Hormone and vasoactive amine secretion from the carcinoid tumor cells cause carcinoid syndrome [11]. In our case did not present with any features of carcinoid syndrome. In addition, the total abdominal hysterectomy with bilateral salpingo-oophorectomy has been commonly recommended in postmenopausal patients. Premenopausal women with tumors confined to the ovary may be treated with fertility-sparing surgery, as tumors are usually unilateral and carry a good prognosis, but careful staging to exclude occult metastases is important [17-20].
Conclusion
In conclusion, SCTO is an extremely rare ovarian tumor. The symptoms of the majority SCTO are usually nonspecific and misleading. We describe a young female patient with a primary strumal carcinoid of the ovary arising from a heterochronous struma ovarii complained abdominal pain, without evidence of carcinoid syndrome or abnormal thyroid functions. In additional, a comprehensive understanding of the clinical characteristic SCTO, diagnosis and management is very important. Diagnosis of strumal carcinoid must to be confirmed on histopathology and immunohistochemistry.
Acknowledgements: I would like to thank for the Department of Department of Obstetrics and Gynecology, Dr. ZhengXian Lin provide the pictures and descriptions of the pelvic sonography and intra-operative findings of the present case.
References
- Robboy SJ, Scully RE. Stromal carcinoid of the ovary. An analysis of 50 cases of a distinctive tumor composed of thyroid tissue and carcinoid. Cancer. 1980; 46: 2019-2034.
- Davis KP, Hartmann LK, Keeney GL, et al. Primary ovarian carcinoid tumors. Gynecol Oncol. 1996; 61: 259-265.
- Sharma R, Biswas B, Wahal SP, Sharma S, Kaushal V. Primary ovarian carcinoid in mature cystic teratoma: A rare entity. Clin Cancer Investig J. 2014; 3: 80-82.
- Wei S, Baloch ZW, LiVolsi VA. Pathology of struma ovarii: A report of 96 Cases. Endocr Pathol. 2015; 26: 342-348.
- Bouomrani S, Rekik F, Guermazi M, Yahyaoul S. Carcinoid tumor on mature cystic ovarian teratoma in a young woman. J Gynecol Women’s Health. 2019; 14: 555880.
- Gonzalez MD, Navarrete SV, Pena RJ, Escamez Leon MC. Primary ovarian carcinoid tumor arising within a mature cystic teratoma in a 32-years-old patient. Gynecol Reproduct Endocrinol -UK. 2018; 2: 2-4.
- Yamada S, Hisaoka M, Tanimotoc A, Urabed R, Sasaguria Y. Two cases of strumal carcinoid of the ovary: The enigma of its histogenesis. Rev Esp Patol. 2011; 44: 49-54.
- Gorin I, Sastre-Garau X. Strumal carcinoid tumor of the ovary. J Clin Oncol. 2008; 26: 2780-2781.
- Theurer S, Ingenwerth M, Herold T, Herrmann K, Schmid KW. Immunohistochemical profile and 47-Gene Next-Generation Sequencing (NGS) solid tumor panel analysis of a series of 13 strumal carcinoids. Endocr Pathol. 2020; 31: 101-107.
- Stewart MJ, Willis RA, De Saram GSW. Argentaffine carcinoma (carcinoid tumour) arising in ovarian teratomas; A report of two cases. J Pathol Bacteriol. 1939; 49: 207-2012.
- Qiao PF, Gao Y, Niu GM. Struma ovarii accompanied by mature cystic teratoma of the other ovary: A case report and literature review. Oncol Lett. 2015; 9: 2053-2055.
- Antovska VS, Trajanova M, Krstevska I, Gosheva I, Chelebieva J, Prodanova I. Ovarian strumal carcinoid tumour: Case report. Open Access Maced J Med Sci. 2018; 6: 540-543.
- Kachhawa G, Kumar S, Singh G, Mathur S, Kumar L, Sharma J. Ovarian strumal carcinoid presenting as severe progressive constipation. J Surg Case Rep. 2011; 8: 5-8.
- Braunschweig R, Hurlimann J, Gloor E, Campiche M. Ovarian carcinoid tumors: Immunohistochemical and ultrastructural study of 8 cases. Ann Pathol. 1994; 14: 155-162.
- Soga J, Osaka M, Yakawa Y. Carcinoids of the ovary: An analysis of 329 reported cases. J Exp Clin Cancer Res. 2000; 19: 271-280.
- Kusku E, Eroglu D, Ozdemir BH et al. Primary carcinoid tumor of the ovary: A case report. Eur J Gynaecol Oncol. 2003; 24: 574- 576.
- Modlin IM, Sander A. An analysis of 8305 cases of carcinoid tumors. Cancer. 1997; 79: 813-829.
- Rabczyński JK, Zabel M, Prudlak L, Kochman AT, Lewandowski M. Strumal carcinoid of ovary. A case report with immunohistochemical investigations. Clin Exp Obstet Gynecol. 1999; 26: 112- 114.
- Lenicek T, Tomas D, Soljacić-Vranes H, et al. Strumal carcinoid of the ovary: Report of two cases. Acta Clin Croat. 2012; 51: 649- 653.
- Metwally IH, Elalfy AF, Awny S, Elzahaby IA, Abdelghani RM. Primary ovarian carcinoid: A report of two cases and a decade registry. J Egypt Nat Can Inst. 2016; 28: 267–275.