
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
3D preoperative assessment for locally advanced pancreatic cancer undergoing modified-Appleby procedure with reversed autologous arterial graft reconstruction: A case report
Christian Cotsoglou*; Stefano Granieri; Sissi Paleino; Andrea Chierici
General Surgery Unit, Ospedale di Vimercate, ASST Brianza, Via Santi Cosma e Damiano 10, 20871, Vimercate, Italy.
*Corresponding Author : Christian Cotsoglou
Department of General Surgery, Vimercate Hospital,
ASST di Vimercate, via Santi Cosma e Damiano 10,
29871 Vimercate (MB), Italy.
Email: christian.cotsoglou@asst-brianza.it
Received : Mar 15, 2021
Accepted : Apr 19, 2021
Published : Apr 21, 2021
Archived : www.jcimcr.org
Copyright : © Cotsoglou C (2021).
Abstract
Advanced pancreatic ductal adenocarcinoma represents one of the most challenging oncologic diseases nowadays for many reasons: it is burdened by one of the poorest prognoses, it is often diagnosed when in an advanced stage and it demands a multimodal approach which is necessary to assign the proper patient-specific treatment. When feasible, surgical resection combined with systemic treatment is still the best curative choice and can require complex vascular resections and reconstructions to obtain R0 margins. In these cases, a detailed preoperative assessment made of blood tests, thoracoabdominal imaging and histological definition of the tumor is fundamental.
Unfortunately, the current imaging techniques are not completely reliable in defining the extension of the contact between the neoplasm and the surrounding arteries and veins, especially when considering borderline and locally advanced diseases.
The use of 3D reconstructions can improve the perception of crucial anatomical details for the diagnostic evaluation and the surgical procedure.
Citation: Cotsoglou C, Granieri S, Paleino S, Chierici A. 3D preoperative assessment for locally advanced pancreatic cancer undergoing modified-Appleby procedure with reversed autologous arterial graft reconstruction: A case report. J Clin Images Med Case Rep. 2021; 2(2): 1060.
Introduction
Pancreatic Ductal Adenocarcinoma (PDAC) carries the lowest survival rate among all major organ cancers with a median overall survival from the moment of diagnosis of 4-6 months and it is the third leading contributor of cancer mortality [1]. Moreover, a recent German study predicts that PDAC will become the second most common cause of cancer-related death in Europe by 2030 [2]. Due to its rapid invasive tendency towards adjacent structures, lymphnodes and distant parenchymatous organs, only 10-20% of patients are suitable for upfront surgery at diagnosis [3]. New neoadjuvant chemotherapy regimens have extended the possibility for patients with advanced cancers to undergo surgical treatment and this is reflected in the most recent National Comprehensive Cancer Network guidelines for pancreatic adenocarcinoma [4]. Resectability of PADC depends on the kind of involvement of the main local vessels. Preoperative assessment of vascular involvement by PDAC has consequently become of primary relevance to set up the correct multimodal strategy to offer the best approach for the patient. This case report represents a striking example of how the application of the most updated findings about PDAC treatment, the skills gained in liver transplantation surgery on vascular resections and reconstructions and the most developed imaging devices allow proper treatment of advanced stage diseases.
Case report
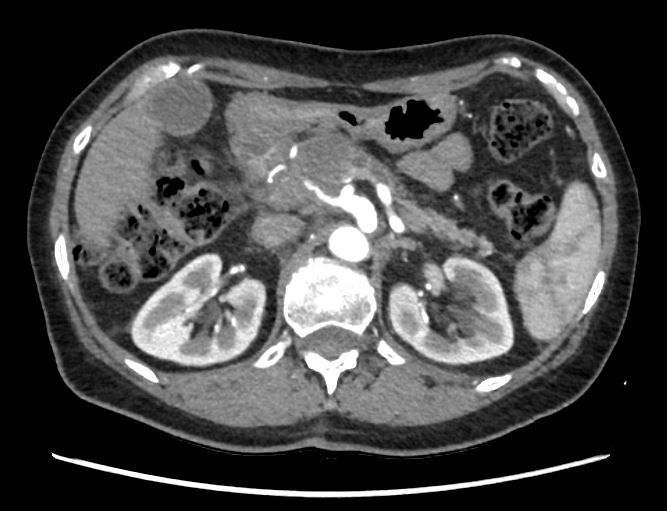
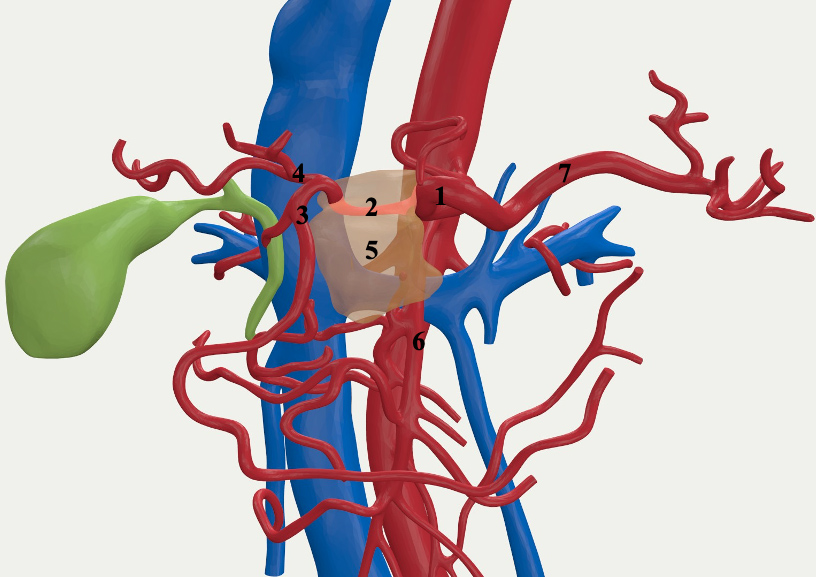
A 61 years old woman was addressed to our center after realizing an abdominal echography for epigastric pain that showed a pancreatic body lesion. The pathologic staging, including a thoraco-abdominal contrast enhanced CT-scan (ceCTscan) and a pancreatic endoscopic ultrasonography (EUS) with Fine Needle Agiobiopsy (FNAB) found a PDAC with complete involvement of the common hepatic artery (CHA), ≤180° contact with the Celiac Axis (CA), mild contact with the GastroduoDenal Artery (GDA) and ≤180° contact with the Superior Mesenteric Vein (SMV) considered as “Locally Advanced” following the NCCN guidelines [4]; CA19.9 was 5192U/L. A neoadjuvant chemotherapy regimen with Nab-paclitaxel/Gemcitabine was introduced and then followed by radiotherapy associated with Capecitabine. Afterwards, the new staging exams revealed a partial PDAC remission with persistent invasion of the CHA and persistent contact with the CA and GDA (Figure 1); no distant metastases were found. CA19.9 was 230U/L. A ce-CTscan based 3D reconstruction was also realized to assess more precisely the relations between the tumor and the adjacent vessels after systemic therapy to verify if a surgical approach was indicated. The reconstruction showed the presence of contact between the PDAC and the CA but no involvement of the GDA and the SMV (Figure 2).
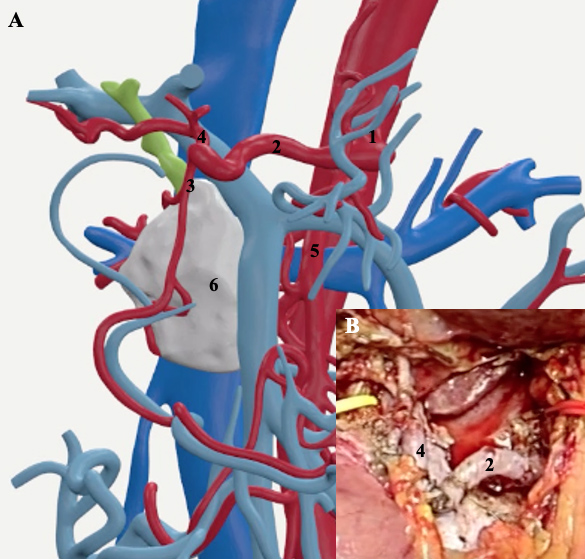
Therefore, the patient was admitted to our Unit to undergo a modified-Appleby procedure [5]. The angiography showed a spontaneous retrograde liver revascularization through the GDA with complete CHA occlusion needing no embolization. Three days later, the patient underwent a distal splenopancreatectomy with CHA resection. When the CHA was clamped at its origin before undergoing resection, an intraoperative liver echo-doppler evidenced an hepatic artery resistive index (HARI) of 0.31 (normal range: 0.55-0.7 [6]) probably due to GDA narrowing caused by the fibrosis of the surrounding tissues due to radiotherapy. Thus, we decided to perform a vascular reconstruction after CHA resection. To re-establish the arterial flow to the liver, we used an autologous arterial graft: the splenic artery was harvested from the specimen, overturned and interposed between the CA and the distal CHA with two end-to-end sutures (Figure 3A-B). The postoperative course was uneventful; discharge took place at postoperative day 5. Histological examination demonstrated a pT2N0M0R0 PDAC. After 3 months, a ceCT-scan showed no cancer recurrence and patency of the reconstructed CHA.
Discussion
Once considered an absolute contraindication to surgery, vascular resections and reconstructions are now accepted in the surgical treatment of invasive PDAC and can improve overall survival compared to both borderline resectable and locally advanced tumors treated with palliation [7]. The indication to perform a pancreatic resection after neoadjuvant therapy depends on very strict and precise criteria that must be assessed preoperatively. The radiologic means used to determine these characteristics are: ceCT-scan, Magnetic Resonance Imaging (MRI), Positron-Emission Tomograpy (PET) and Endoscopic Ultrasound (EUS). A recent multicentric trial [8], mainly based on ceCT-scan analysis, demonstrated that while there is excellent agreement between surgeons in determining the presence of arterial abutment and locally advanced PDAC, low agreement was observed in the determination of tumor infiltration of venous structures and resectability in borderline resectable PDACs. As a matter of fact, ceCT-scan has limited efficacy in clearly define R0 resectability and T-stage in these situations and its performances are worsened by neoadjuvant therapy [9,10].
Pancreatic high-definition 3D reconstruction based on ceCTscan is a recently developed tool that is gaining increasing attention. While its usefulness in resident training is already demonstrated [11], its importance in defining the tumors anatomical characteristics has not been definitely confirmed. In particular, there is a lack of evidence in weather 3D reconstruction could refine the preoperative staging in borderline situations.
This case report represents a clear example of how 3D reconstruction represents a valuable tool in unclear anatomical situations and can improve the effectiveness of preoperative assessment; combined with the expertise gained in the transplantation field for vascular reconstructions it allows to allocate the best possible cure to each specific patient.
References
- Bengtsson A, Andersson R, Ansari D. The actual 5-year survivors of pancreatic ductal adenocarcinoma based on real-world data. Sci Rep. 2020; 10: 1-9.
- Quante AS, Ming C, Rottmann M, et al. Projections of cancer incidence and cancer-related deaths in Germany by 2020 and 2030. Cancer Med. 2016; 5: 2649-2656.
- Kwon J, Shin SH, Yoo D, et al. Arterial resection during pancreatectomy for pancreatic ductal adenocarcinoma with arterial invasion: A single-center experience with 109 patients. Medicine (Baltimore). 2020; 99: e22115.
- National Comprehensive Cancer Network. Pancreatic adenocarcinoma. Published 1AD.
- Cannella R, Borhani A, Zureikat A, Tublin M. Appleby Procedure (Distal Pancreatectomy With Celiac Artery Resection) for Locally Advanced Pancreatic Carcinoma: Indications, Outcomes, and Imaging. Am J Roentgenol. 2019; 213: 35-44.
- McNaughton DA, Abu-Yousef MM. Doppler US of the liver made simple. Radiographics. 2011; 31.
- Del Chiaro M, Rangelova E, Halimi A, et al. Pancreatectomy with arterial resection is superior to palliation in patients with borderline resectable or locally advanced pancreatic cancer. Hpb. 2019; 21: 219-225.
- Wittel UA, Lubgan D, Ghadimi M, et al. Consensus in determining the resectability of locally progressed pancreatic ductal adenocarcinoma – results of the Conko-007 multicenter trial. BMC Cancer. 2019; 19: 1-9.
- Barreto S, Loveday B, Windsor J, Pandanaboyana S. Detecting tumour response and predicting resectability after neoadjuvant therapy for borderline resectable and locally advanced pancreatic cancer. ANZ J Surg. 2018.
- Cassinotto C, Cortade J, Belleannée G, et al. An evaluation of the accuracy of CT when determining resectability of pancreatic head adenocarcinoma after neoadjuvant treatment. Eur J Radiol. 2013; 82: 589-593.
- Lin C, Gao J, Zheng H, et al. Three-Dimensional Visualization Technology Used in Pancreatic Surgery: A Valuable Tool for Surgical Trainees. Published online 2020: 866-873.