
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
A unique association of diaphragmatic hernia and pulmonary tuberculosis in an infant
Karolina Dolezalova; Marketa Bloomfield; Martin Magner*
Department of Pediatrics, First Faculty of Medicine, Charles University and Thomayer University Hospital in Prague, Czech Republic.
*Corresponding Author : Martin Magner
Pediatric Department, First Faculty of Medicine,
Charles University and Thomayer University Hospital in Prague, Videnska 800, 120 00 Prague, Czech
Republic.
Email: martin.magner@vfn.cz
Received : Mar 11, 2021
Accepted : Apr 23, 2021
Published : Apr 27, 2021
Archived : www.jcimcr.org
Copyright : © Magner M (2021).
Abbreviations: CXR: Chest X Ray; CT: Computed Tomography; CDH: Congenital Diaphragmatic Hernia; TB: Tuberculosis.
Citation: Dolezalova K, Bloomfield M, Magner M. A unique association of diaphragmatic hernia and pulmonary tuberculosis in an infant. J Clin Images Med Case Rep. 2021; 2(2): 1072.
Case report
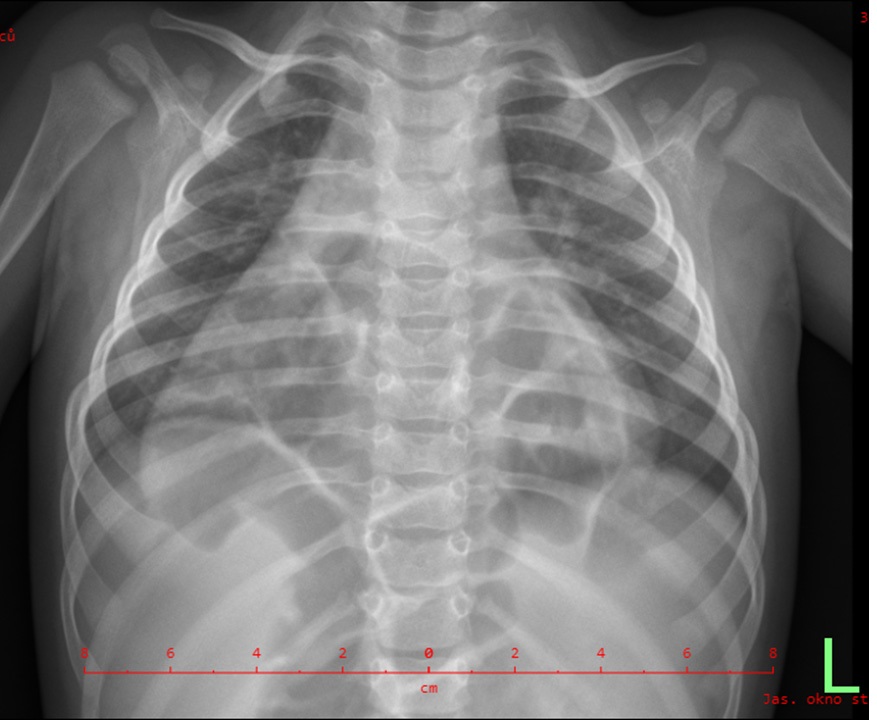
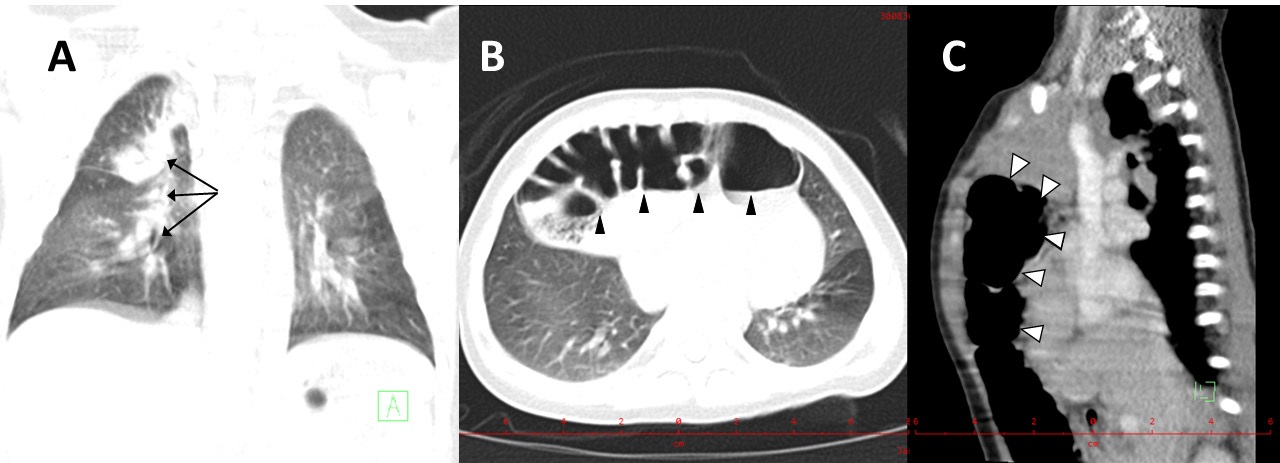
We report a healthy-appearing 7-month-old girl of non-related ancestry, uneventful pre - and postnatal development and past medical history, who was investigated for lung Tuberculosis (TB) in her mother. Tuberculin skin test was highly positive (20 mm induration, normal range 0-5 mm in unvaccinated children). Chest X-ray (CXR) revealed a surprising image suggestive of the presence of abdominal contents in the thoracic cavity (Figure 1); the unobscured lung parenchyma showed no signs of TB. Computed Tomography (CT) imaging detected branching linear opacities and patchy consolidation in the right upper lobe, intrathoracic lymphadenopathy and confirmed retrosternal dislocation of colon (Figure 2 A,B,C). Thus, the diagnosis of concurrent lung TB and Congenital Diaphragmatic Hernia (CDH) was established. The 4-drug regimen of antituberculotics was initiated, i.e. isoniazid, rifampicin, pyrazinamide and ethambutol. The hernia repair was deferred to prevent abdominal dissemination of Mycobacterium tuberculosis.
CDH represents the most common intrathoracic fetal anomaly (1:3,000 live births; male to female ratio 2:1). The abdominal contents protrude into the thoracic cavity through a developmental defect in the diaphragm. Ranging from a small aperture in the posterior muscle rim to a complete absence of diaphragm, it may interfere with normal lung development. Postero-lateral hernias, also known as Bochdalek hernias, are the most common (70-75%), followed by anterior defects or Morgagni hernias and central hernias [1]. Clinical presentation is variable; most typically, tachydyspnea, tachycardia, cyanosis and caved-in appearance of the abdomen are apparent shortly after birth. CDH is often diagnosed via antenatal ultrasound. In some cases, it remains oligosymptomatic till adulthood. The incidence of TB in the Czech Republic is very low (4,3/100 000) [2]. The population at highest risk are the youngest children living in TB households [3].
The occurrence of lung TB in a patient with CDH has not been reported so far and we presume the association to be coincidental. Of note, several cases of late-presenting CDH, treated erroneously as TB due to a misinterpreted CXR, have been referred [4]. Our case demonstrates the necessity to actively investigate TB household contacts, even if asymptomatic. It also emphasizes the utility of CT imaging in case of negative or inconclusive chest X ray in selective screening for tuberculosis in infants at high risk of TB acquisition.
Funding: Supported by MZ ČR RVO – Thomayer University Hospital TN 00064190.
References
- Chandrasekharan Praveen Kumar, Rawat Munmun, Madappa Rajeshwari, Rothstein David H, Lakshminrusimha Satyan. Congenital Diaphragmatic Hernia - A Review - PubMed. Matern Health Neonatol Perinatol. 2017.
- Basic Overview of Tuberculosis Epidemiology in the Czech Republic in 2019 Czech Health Statistics Published by the Institute of Health Information and Statistics of the Czech Republic Palackého nám. 4, Prague, Czech Republic www.uzis.cz. 2019.
- Lancella L, Vecchio A Lo, Chiappini E, Tadolini M, Cirillo D, Tortoli E, et al. How to manage children who have come into contact with patients affected by tuberculosis. Journal of Clinical Tuberculosis and Other Mycobacterial Diseases. 2015.
- Shaaibu AS, El-Habeeb AM, Mustapha IM, Danjaji AU. Delayed presentation of congenital diaphragmatic hernia masquerading as pulmonary tuberculosis in a 4-year-old girl. Pyramid J Med. 2019; 2.