
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
FDG embolism mimicking lung metastasis
Amin Haghighat Jahromi1,2*; Carl K Hoh1
Department of Radiology, University of California, San Diego, California, USA.
*Corresponding Author : Amin Haghighat Jahromi
Department of Radiology, University of California, San
Diego, California, USA.
Email: ajahromi@ucsd.edu
Received : Mar 27, 2021
Accepted : Apr 27, 2021
Published : Apr 30, 2021
Archived : www.jcimcr.org
Copyright : © Jahromi AH (2021).
Abstract
2-[18F]-FDG embolism artifact is a PET pitfall that may cause misinterpretation as lung metastasis. This rare phenomenon results from clumping of the radiotracer with platelet aggregates during intravenous administration. It should be considered, especially if there is no corroborating anatomic correlate for focal pulmonary FDG activity and if the radiotracer is administered through a central venous catheter. Herein, we present images of a 3-year-old girl with history of abdominal neuroblastoma and lung metastasis, showing FDG embolism artifact, subsequently resolved in the repeat imaging. Our case reinforces the importance of knowing this artifact as misinterpretation can have a significant effect on patient management.
Keywords: FDG embolism; PET/CT; Pitfall.
Citation: Jahromi AH, Hoh CK. FDG embolism mimicking lung metastasis. J Clin Images Med Case Rep. 2021; 2(2): 1086.
Description
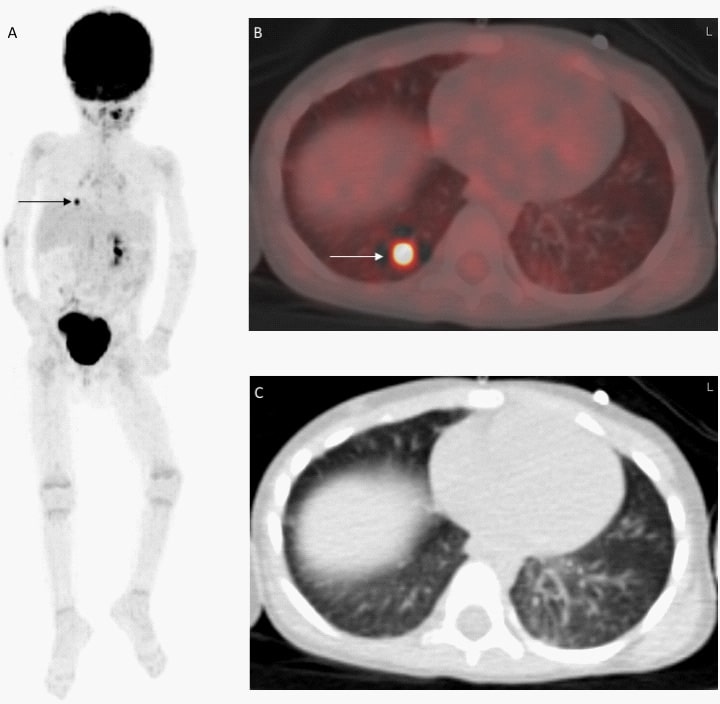
A 3-year-old girl with history of abdominal neuroblastoma and lung metastasis underwent staging with 2-[18F]-fluoro-2- deoxy-D-glucose (2-[18F]-FDG) positron emission tomographycomputed tomography (PET-CT) for assessment of treatment response. According to her last 2-[18F]-FDG PET-CT, she had no recurrent or metastatic disease, following treatment. The only positive finding in the current PET-CT was focal FDG activity in the right lung, suspicious for metastatic neuroblastoma (Panels A and B). However, there was no anatomic correlate, attributed to small size of the metastatic nodule in the low-dose CT, considering her history of metastatic pulmonary nodules (Panel C). Subsequently, she received a dedicated chest CT which again did not show any pulmonary nodule to account for the radiotracer activity. She underwent a repeat PET-CT which showed resolution of the FDG focus. The finding is attributed to FDG embolism artifact, postulated to result from clumping of the radiotracer with platelet aggregates during intravenous administration, especially through the central venous catheter, such as this patient [1]. This artefact is well described in adult patients, less in paediatric population. However, it is well known that catheter administration of radiopharmaceutical should be avoided. This pitfall may cause misinterpretation as lung metastasis [2], therefore FDG embolism should be considered especially if there is no corroborating anatomic correlate and if FDG administration route is through a central venous catheter [3].
Author contributions: Conceptualization A.H. and C.H.; data curation, A.H.; writing-original draft preparation, A.H.; writingreview and editing, A.H. and C.H.; supervision, C.H. All authors have read and agreed to the published version of the manuscript.
Funding: Amin Haghighat Jahromi is supported by NIH T32- 4T32EB005970 grant.
Consent for publication: The patient’s mother provided written informed consent for the publication of this case.
References
- Tokmak H. Focal FDG Uptake in Lung Parenchyma Without Structural Alterations on CT. World J Nucl Med. 2013; 12: 38-40.
- Kavanagh PV, Stevenson AW, Chen MY, Clark PB. Nonneoplastic diseases in the chest showing increased activity on FDG PET. AJR Am J Roentgenol. 2004; 183: 1133-1141.
- Hany TF, Heuberger J, von Schulthess GK. Iatrogenic FDG foci in the lungs: A pitfall of PET image interpretation. Eur Radiol. 2003; 13: 2122-2127.